Article Text

Abstract
Objective: To determine the proportion of consultations requested by general internal medicine services that communicate key components of the consultation process to medical subspecialists.
Design: Retrospective chart review by two researchers, using a standardised chart abstraction instrument (93.1% agreement, κ 0.85).
Setting: Calgary, Alberta, Canada.
Sample: A random sample of medical consultations was selected from those generated on two medical teaching units (MTUs) from 2003 to 2004.
Measurements: The primary measure of interest was whether a “clear clinical question” was posed to the subspecialist, a binary variable.
Results: Two hundred consultations were sampled from the 2885 subspecialty consultations. Of the selected consultations, 94.0% (188/200) were available for review. A clear clinical question was posed in 69.7% (131/188) of consultations (CI 0.63 to 0.74). In a secondary analysis involving a larger sample permitting comparison across subspecialties, 95.1% (368/387) of the consultations, representative of the subspecialties, were available for review. An MTU member contacted the subspecialist for 74.2% of consultations. If a consultation was urgent, a member of the MTU contacted the subspecialist in 81.0% of consultations. Of these urgent consultations, 63.3% had a clear clinical question.
Conclusion: More than one in four consultations does not contain a clear clinical question, illustrating suboptimal communication between physicians. Innovative strategies that provide a sustainable solution for overcoming barriers to communication could have a significant impact on quality of care.
Statistics from Altmetric.com
Communication is an essential part of coordinating healthcare services, particularly when providing healthcare to patients with multiple comorbidities involving an extensive team of specialists. Consultation is the first step in establishing communication with other providers.
Goldman et al (1983) wrote a landmark paper discussing the “Ten Commandments for Effective Consultation” outlining the role of the attending physician.1 These guidelines have assisted attending physicians in communicating the appropriate information to medical subspecialists for efficient, and effective consultations with the goal of improving patient care.23 In the initiation phase of consultation, the attending physicians are asked to formulate a clear clinical question and contact the consultant.14 A recent article by Salerno et al, which amends the commandments for the present day physician, continues to emphasise the importance of communication and endorse an even more interactive relationship between consultant and attending physician.5
The purpose of our study was to determine the percentage of consultation requests from general internal medicine (GIM) services that pose a clear clinical question to medical subspecialists. The secondary objective was to assess the frequency of direct communication between the GIM service and the consulting specialist, and to describe differences in the consultation process by subspecialty.
METHODS
Study population
Patients discharged from the medical teaching units (MTU) at two academic, tertiary care hospitals in Alberta, Canada in 2003–2004 were identified through an administrative database. The two hospitals are publicly administered, servicing an urban and rural population of one million. The MTU is a GIM service with an attending general internist who oversees patient care by two senior residents, junior residents from various subspecialties and medical students.
The administrative database documented MTU patients who received a consultation during admission. Consultation requests to any of the 12 medical subspecialties were identified: gastroenterology, dermatology, nephrology, respirology, cardiology, neurology, oncology, rheumatology, geriatrics, haematology, endocrinology and infectious disease.
A two-step sampling scheme was undertaken. First, a sample of the consultation requests to medical subspecialties was randomly selected, using a random numbers table, from the total number of consultations occurring on the MTU. This initial sample therefore contained a proportional representation of consults from each of the medical subspecialties; those services that were utilised with the greatest frequency represented a larger part of the initial sample. We then conducted a second sampling step for our secondary analysis. Additional consultations were selected purposefully to obtain a more equal representation from each subspecialty. Consultations were randomly selected from each of the specific subspecialties that had fewer than 30 consultations until there were at least 30 consultation requests from each group.
All selected consultation cases (from both sampling steps) were then subjected to a detailed chart review. A numeric patient identifier, subspecialty consulted and date of consultation were used to locate selected consultations for review.
Consultations at both sites are recorded in the form of a computerised entry. The consultations are unscripted, and thus allow the initiator of the consult to place their own text into the system without any prompting or editing in the software. Initiators of the consultation also select how the consultant is contacted from a list of four options (staff physician, resident, nurse or unit clerk to contact the consultant) and the time frame for the consultation request (urgent, within 24 h, within 48 h).
Study measurements
A chart abstraction instrument was developed for retrospective review of the clinical question of each consultation selected. Consultations were reviewed by one of two independent reviewers. The primary data measure for a clear clinical question was binary. Consultations that contained subject information, a specific issue to address (ie, diagnosis or investigation) and an action to be taken by the consultant (ie, management, procedural request, treatment suggestions) were considered “clear.” An example of a clear clinical question was: “Patient.... with S milleri bacteremia and an exudative pleural effusion. Please see regarding discontinuing antibiotics.” Consultations without any one of the three components were judged to be “unclear;” these may have provided only descriptive patient information and did not identify a specific issue or an action to be taken by the consultant. An example of an unclear clinical question was: “Acute renal failure and rhabdomyolysis with decreased urine output.” The chart abstraction instrument was standardised for 30 consultations with agreement of 93.1% between reviewers for this key variable (κ 0.85).
The chart abstraction instrument also collected descriptive data. The subspecialty service and general reason for consultation were recorded. Principles of initiating a consultation were measured categorically, including: urgency of consultation, and attempt to contact the subspecialist. The time interval for consultation request was categorised as “stat,” “today/urgent,” and within “24 h” or “48 h.” Consultations requested in 24 h or less were grouped under the heading of “Urgent.”3 How the consultant was contacted was also recorded; “unit clerk,” “resident,” “medical student,” “nurse,” “staff” or “not at all.” Contact by the staff physician, a resident or a medical student was judged to indicate that the consultant was “contacted by a member of the MTU.”
Sample size consideration
The a priori sample size calculation for determining the frequency of a clear clinical consultation question with a confidence interval of ±7.5%, suggested a minimum of 171 consultations assuming an estimated frequency of clear clinical questions of 50%. Given this calculation, for the primary analysis, a random sample of 200 consultations was selected from all those that were eligible.
Data analysis
Statistical analysis was descriptive with simple reporting of proportions and in some instances binomial 95% confidence intervals. We also used chi-squared tests to compare the proportion of consultations with a clear clinical question, direct contact by a member of the MTU with the consultant and urgent consultations across medical subspecialties.
RESULTS
Determination of sample
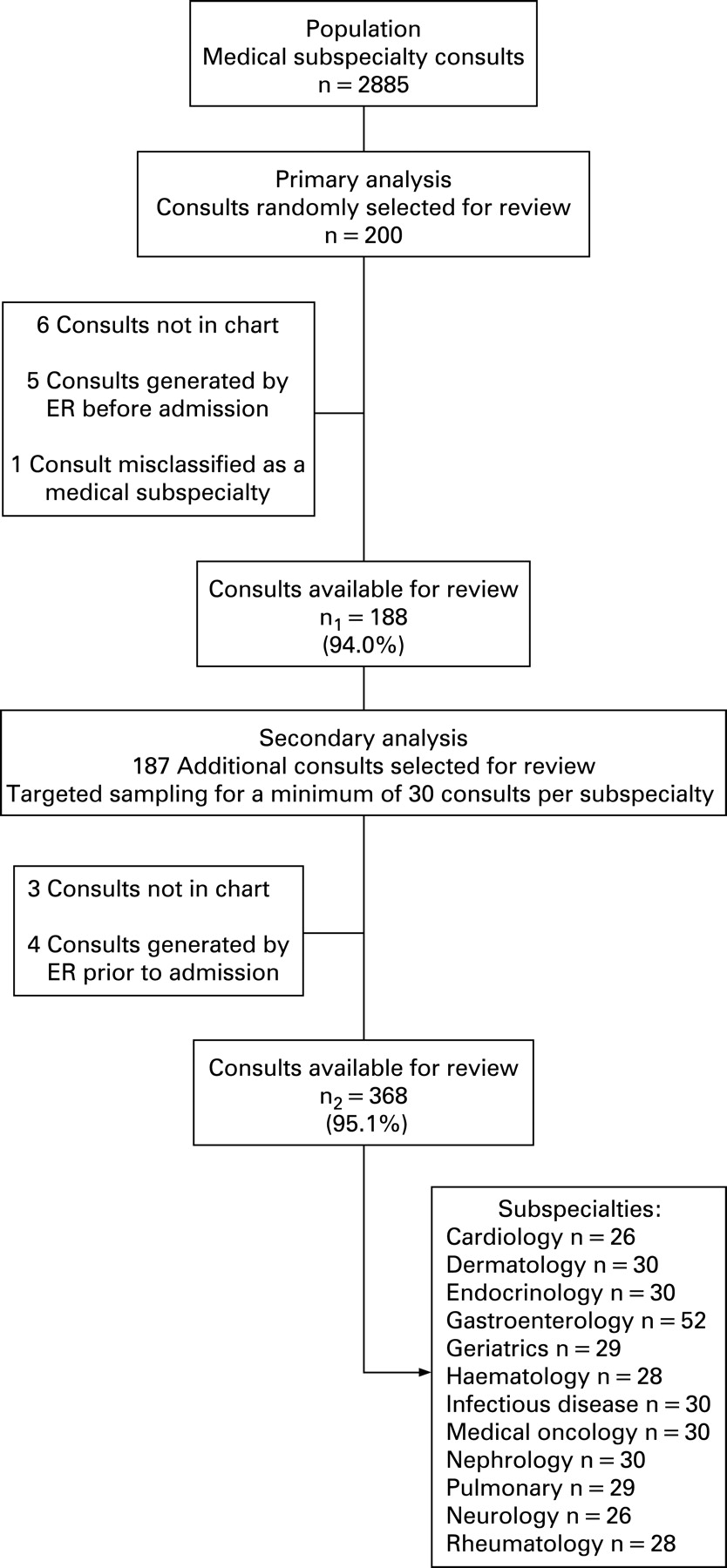
During the study period from 2003 to 2004, medical subspecialists received 2885 consultations from the MTU. Of the 200 randomly selected consultations for the primary analysis, 94.0% (188/200) were available for chart review. The other 12 consultations were not found on the chart (6/12), were generated by the emergency department prior to admission (5/12) or were misclassified as a medical consultation (1/12). The sample for the primary analysis provided a true representation of consultation patterns on the MTU. For the secondary analysis a larger sample of consultations was obtained to have a more equal representation across the subspecialties; 95.1% (368/387) of the total sample were reviewed (fig 1).

Overall assessment of clear clinical question
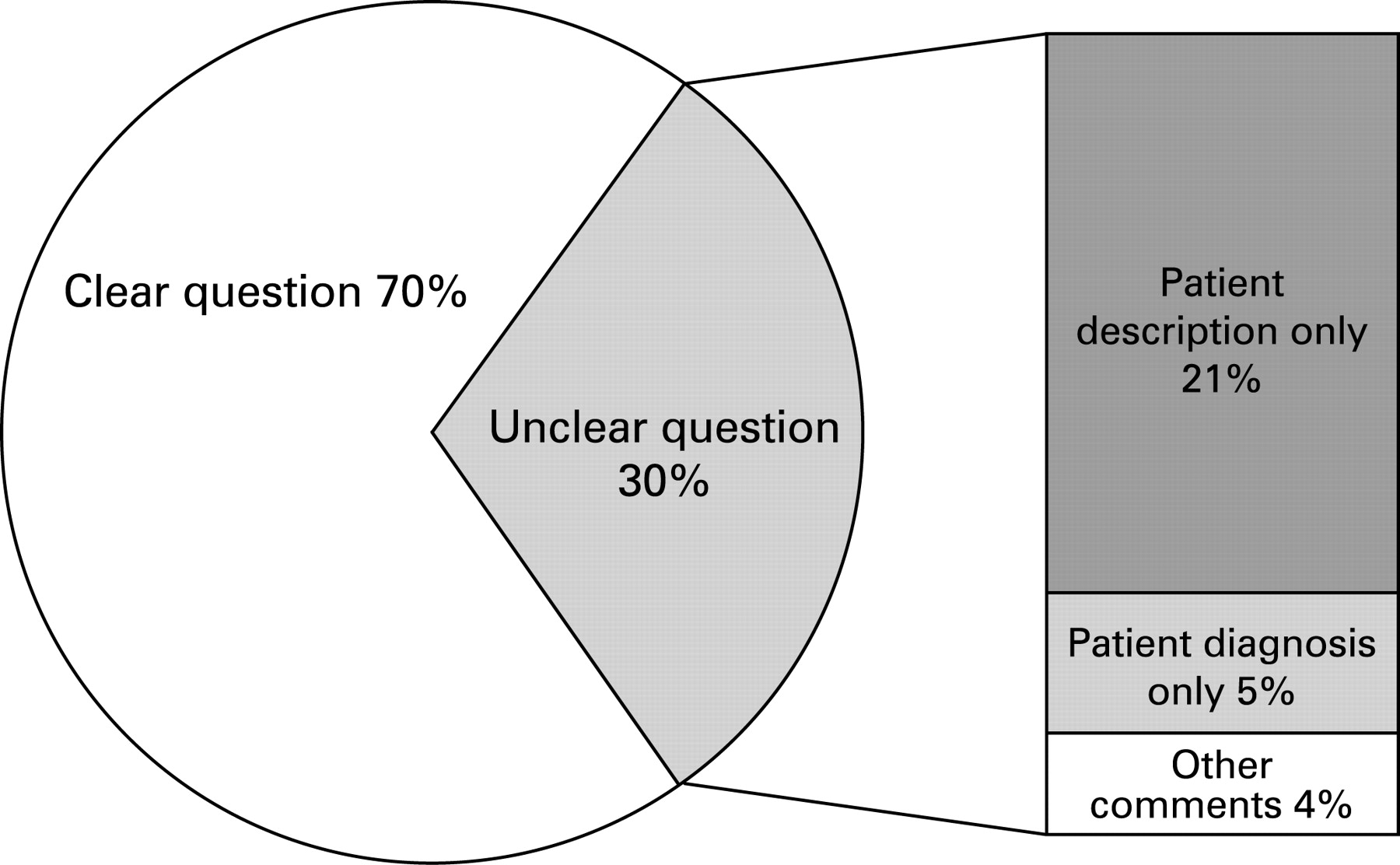
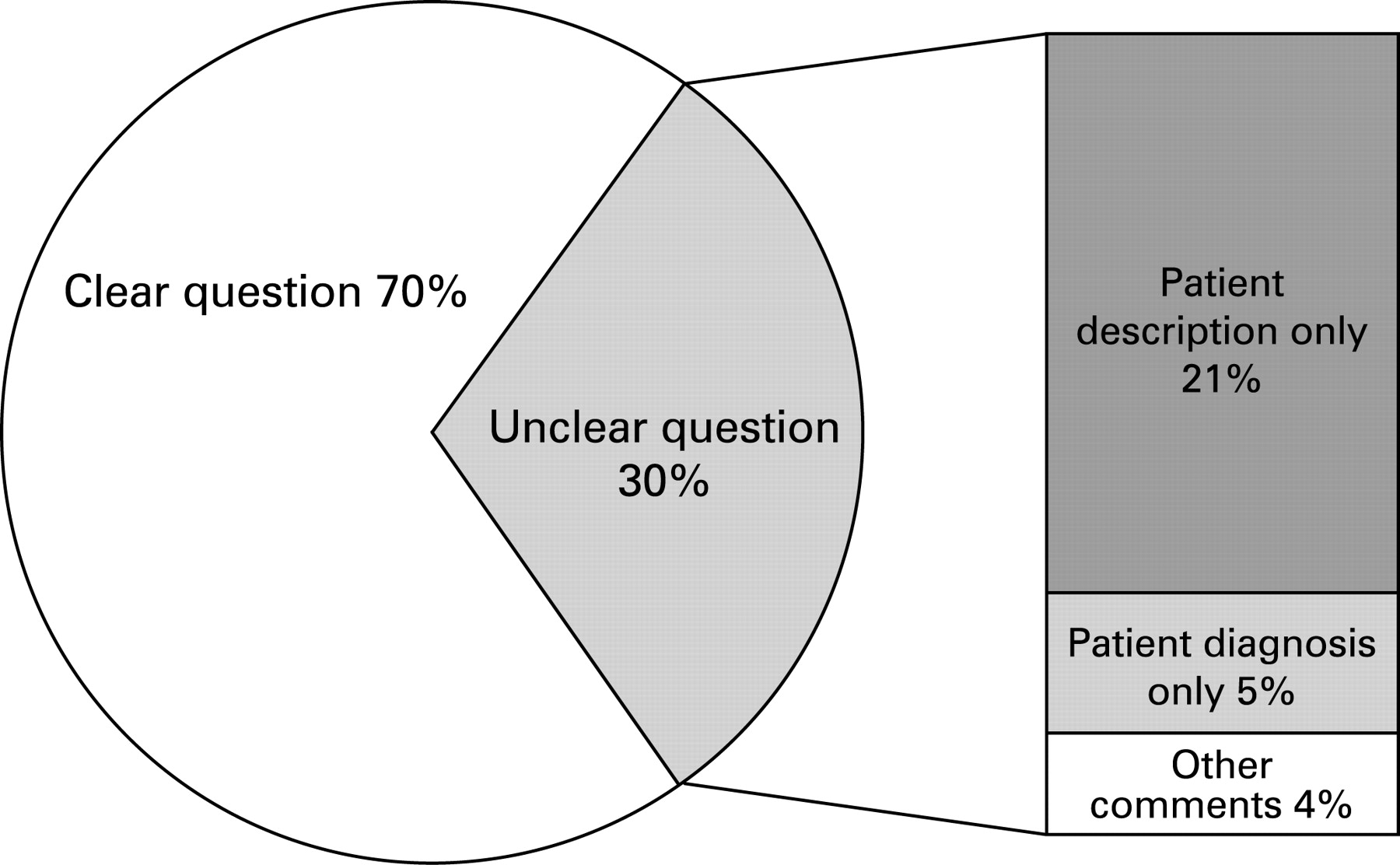
A clear clinical question was posed in 131 consultations, 69.7% (63% to 76%). Of the consultations without a clear clinical question, 40 had only a patient description, 10 had only a patient diagnosis, and seven had other comments (fig 2). These other comments included “as discussed,” “transfer of care” and “patient known to you.”
{kind=link}
{kind=link}
Analysis of subspecialties and secondary characteristics of consultation
One of the members of the MTU contacted the medical subspecialist for 74.2% (273/368) of consultations. The majority of consultations were requested for review within 24 h (45.3%, 167/368). Urgent consultations occurred in 42.9% (158/368) of medical subspecialty consultations. If a consultation was urgent, a member of the MTU contacted the subspecialist in 81.0% (128/158) of the consultations. Of these urgent consultations, 63.3% (100/158) had a clear clinical question. We assessed whether there was any association between the training status of requesting physicians and the likelihood of a clear question, and found that resident physicians posed clear questions in 77% (143/185) of their requests, while staff physicians posed clear questions in 64% (36/56) of consult requests (p = 0.051).
Differences between subspecialties in factors that affect the efficacy of consultation were seen in all areas (table 1), although none of the observed differences were statistically significant. Neurology was the least likely to receive a consult with a clear clinical question (61.5%, 16/26). Dermatology (63.3%, 19/30) and Geriatrics (55.2%, 16/30) were contacted by a member of the MTU regarding consultation much less frequently in comparison with the other subspecialties (74.4%, 274/368).
DISCUSSION
One-quarter of medical consultations are requested without a clear or implied clinical question recorded. A physician does not communicate a quarter of the consultations to the subspecialist. Even when the consultation is deemed to be urgent, the reason for consultation is often unclear, and the consultation is not discussed.
A multidisciplinary team provides patient care on GIM services. Both verbal and documented communication between specialists and the attending physician is essential for ensuring that patients’ needs are addressed both in hospital and in the outpatient setting.67
The “Ten Commandments for Effective Consultation” suggest two important principles for initiating consultation.1 The first principle, “determining the question” for the subspecialist, includes recording a clear question and discussing the issue with the consultant to ensure that the patient’s needs are clear. The second is to establish urgency with the consultant. The emphasis is thus clearly placed on communication between physicians. A recent article updating the “Ten Commandments” showed that 75% of physicians desire the initial verbal communication that establishes the expectations of both physicians.5 Although physicians agree communication is important in the consultation process, they report contacting colleagues with only moderate frequency.8 Barriers to effective communication include lack of time, inconvenient methods of contacting other physicians and conflicting priorities.47
As communication is the first step for effective consultation, it directly impacts healthcare quality.67 An unclear consultation can result in inefficiency and strain relationships between multidisciplinary team members, and often does not serve the patient’s needs.47 Consultations that are misinterpreted by the consultant are less useful for the attending physician, and recommendations are, as a result, often not followed.4 If such consultations are not found to add value, they represent wasted system resources.910 Inefficiency or waste in the system of consultation is represented by at least two MUDA concepts;910 redundancy or waiting. Resources are wasted if an unclear clinical question results in the consultant not addressing the issue for the attending physician, and consultation can become redundant. This scenario unfortunately occurs too frequently in the consultation process. A study by Lee et al illustrates this in demonstrating complete disagreement between the attending physician and the consultant regarding the reason for consultation in 14% of cases.4 Misunderstandings in consultation result in prolonged periods of waiting. Longer lengths of stay result from delays in patient care if management or procedural recommendations were desired and not conveyed on the original consultation.11 Furthermore, failure to contact the consultant can lead to consultations that could, after some discussion, actually be dealt with non-urgently or on an outpatient basis.12 Given the volume of consultations generated by the GIM service (n = 2885) and the potential impact of miscommunication on patients and resources; we consider this to be an area in need of improvement. We suspect that similar inefficiencies would be found in any healthcare centre that uses an unstructured system for recording consultations. Addressing these issues by targeting the consultation process could enhance quality of care and patient satisfaction by reducing the chance of a prolonged length of stay, and minimising redundancy to limit wasted resources.6712
One approach to change is through provider education (eg, conducting simple teaching sessions on the importance of communication in the consultation process). However, such educational strategies often have only a short-term effect,13 particularly in an environment such as the MTU where there is frequent physician turnover relating to staff rotations. It is unlikely that a significant change would be sustained by education alone.13 Implementing a solution to the communication barriers may be more likely to facilitate permanent change.13 Innovative use of computerised physician order entry (CPOE) technologies hold some promise for enhancing accessibility and communication in the consultation process. One concept to explore is a consultation interface in CPOE systems that could prompt physicians requesting a consultation to clarify the clinical question and then directly contact the subspecialist via the paging system. Such a system could then also incorporate flexibility to address the different information needs of each subspecialty (eg, prompts for information on past cardiac history in cardiology consultations). Innovations developed in such a manner and on such a platform are the ones most likely to be successful in promoting change.13
Limitations
Our study assesses charted evidence of communication. We cannot definitively exclude direct verbal communication of a clear clinical question. We would assert based on anecdotal observations, however, that it is unlikely that uncharted verbal communication fully explains the 25% of consultations without a clear clinical question. Furthermore, even if there was some uncharted communication of information on the reason for consultation, the failure to document such information is still a quality shortfall given the importance of charted information for new providers involved in patient care to reconstruct events and the logical path of clinical decision-making in a given patient. The importance of clear documentation of logic in the patient record is heightened in a clinical setting such as the MTU, where a large number of physicians at various levels of training are involved in patient care, with frequent sign-overs occurring between providers.
A second limitation is that we were only evaluating the consultation practices on the MTUs of two tertiary care centres with a single method of generating consultation. Our results may not represent the quality of communication in other settings. However, the literature would suggest that similar suboptimal communication is occurring in other settings with different patient populations. In the absence of quality improvement interventions targeting communication, there is no theoretical basis for thinking it would be better. A third caveat is that the judgement of a clear clinical question is somewhat subjective. However, we carefully and explicitly operationalised this measure between two reviewers before undertaking our study, achieved with “near perfect” agreement (κ = 0.85) in the chart review for this crucial study variable.
CONCLUSION
Despite these limitations, our findings highlight suboptimal written and direct communication in the consultation process. Quality-improvement initiatives that target effective and comprehensive communication as a foundation for high quality of care need to be implemented. These could include a combination of provider education on the importance of communicating and strategic use of information technologies that encourage a clearly specified consultation question.
REFERENCES
Footnotes
Funding: WG is funded by the government of Canada Research Chair in health services research and by the Health Scholar Award from the Alberta Heritage Foundation for medical research.
Competing interests: None.