A randomised controlled trial comparing two schedules of antenatal visits: the antenatal care project
BMJ 1996; 312 doi: https://doi.org/10.1136/bmj.312.7030.546 (Published 02 March 1996) Cite this as: BMJ 1996;312:546
- Jim Sikorski, general practitionera,
- Jennifer Wilson, research midwifea,
- Sarah Clement, research fellowa,
- Sarah Das, research midwifea,
- Nigel Smeeton, lecturer in medical statisticsb
- a Antenatal Care Project, Department of General Practice, United Medical and Dental Schools, London SE11 6SP
- b Department of Public Health Medicine, United Medical and Dental Schools, Guy's Hospital, London SE1 9RT
- Correspondence to: Dr Sikorski.
- Accepted 4 January 1996
Abstract
Objective: To compare the clinical and psychosocial effectiveness of the traditional British antenatal visit schedule (traditional care) with a reduced schedule of visits (new style care) for low risk women, together with maternal and professional satisfaction with care.
Design: Randomised controlled trial.
Setting: Places in south east London providing antenatal care for women receiving shared care and planning to deliver in one of three hospitals or at home.
Subjects: 2794 women at low risk fulfilling the trial's inclusion criteria between June 1993 and July 1994.
Main outcome measures: Measures of fetal and maternal morbidity, health service use, psychosocial outcomes, and maternal and professional satisfaction.
Results: Pregnant women allocated to new style care had fewer day admissions (0.8 v 1.0; P=0.002) and ultrasound scans (1.6 v 1.7; P=0.003) and were less often suspected of carrying fetuses that were small for gestational age (odds ration 0.73; 95% confidence interval 0.54 to 0.99). They also had some poorer psychosocial outcomes: for example, they were more worried about fetal wellbeing antenatally and coping with the baby postnatally, and they had more negative attitudes to their babies, both in pregnancy and postnatally. These women were also more dissatisfied with the number of visits they received (odds ratio 2.50; 2.00 to 3.11).
Conclusions: Patterns of antenatal care involving fewer routine visits for women at low risk may lead to reduced psychosocial effectiveness and dissatisfaction with frequency of visits. The number of antenatal day admissions and ultrasound scans performed may also be reduced. For the variables reported, the visit schedules studied are similar in their clinical effectiveness. Uncertainty remains as to the clinical effectiveness of reduced visit schedules for rare pregnancy problems.
Key messages
Key messages
Women offered a reduced schedule of antenatal visits had a similar rate of caesarean sections for pregnancy related hypertensive disorders
Women having fewer antenatal visits had fewer ultrasound scans and fewer antenatal day admissions
Fewer antenatal visits may lead to poorer psychosocial outcomes and greater dissatisfaction among women
More flexible approaches to the provision of psychosocial support and the reassurance of women about fetal wellbeing may be needed if reduced schedules of antenatal visits are to be introduced
Introduction
The examination of long established patterns of antenatal care in the United Kingdom owes much to the questioning of Hall and colleagues,1 but little systematic work has been carried out since the evaluation of their scheme in Aberdeen.2 Failures to find any association between late booking (after 28 weeks' gestation) and either adverse maternal or neonatal outcomes,3 or between the number of visits received and the onset of eclampsia4 have cast further doubts on the effectiveness of traditional patterns of antenatal visits. A new pattern of antenatal visits for women who are considered to be at low risk has been advocated by the Royal College of Obstetricians and Gynaecologists,5 and new schemes have been adopted in some settings.6 7 Evidence to support the apparent safety of these schedules has been drawn from international comparisons.8 9
The publication of Changing Childbirth, the report of the expert maternity group on the future of the maternity services, and its subsequent adoption as policy by the Department of Health has brought particular pressure for organisational change. This report recommends that the total number of antenatal visits for women with uncomplicated pregnancies should be reviewed in the light of the available evidence.10
Despite considerable observational data on the safety of patterns of care offering fewer than the traditional number of visits, only one prospective trial of alternative visit schedules has been published11; although providing further useful data, it has several limitations. By allocating patients to groups according to their birth dates, it did not use true randomisation, and its findings were not analysed on an intention to treat basis. The sample size was small (n=401), and we question the authors' interpretation of the study's findings relating to women's satisfaction.
In the light of this lack of evidence, and in view of the relatively high rates of fetal and maternal morbidity and mortality associated with late second trimester pre-eclampsia, it has been suggested that the number of antenatal visits for nulliparous women in the second trimester should not be reduced without further evidence of safety.12 Antenatal care has a number of psychosocial functions, such as the provision of reassurance, social support, and information. It is important to establish what effects a reduction in the number of routine visits might have on these functions.13 At the same time, the importance of satisfaction has been highlighted in Changing Childbirth.10 Measures of this, together with health professionals' attitudes to change, are an essential part of the evaluation of any change in routine care.
The main aims of the antenatal care project were to compare the clinical and psychosocial effectiveness of two schedules of antenatal visits, as well as to assess their acceptability to women and their caregivers. We also aimed to examine some of the organisational effects of the two schedules, including continuity of caregiver.
HYPOTHESES
A major clinical concern relating to a reduction in the number of routine antenatal visits is the possibility of increased maternal morbidity associated with late detection of, or failure to detect, pregnancy related hypertensive disorders. We consider that the incidence of caesarean section for such disorders is a reasonable proxy measure for this morbidity. The primary null hypothesis for the trial was that the reduced schedule of visits would not lead to an increase of 1% or more in the rate of caesarean section for pregnancy related hypertensive disorders.
Because antenatal care has a number of other important clinical and non-clinical functions, two further hypotheses were that the reduced and the traditional schedules of visits would not differ in other aspects of clinical effectiveness; and that they would not differ in their psychosocial effectiveness. The final two hypotheses were that the two schedules would not differ in their acceptability to women, nor in their acceptability to the health care professionals who provide antenatal care.
Subjects and methods STUDY POPULATION
All women booking for maternity care at Lewisham or Guy's Hospitals, or at community sites within the catchment areas of these hospitals, between June 1993 and July 1994 were given an information leaflet explaining the project before their initial antenatal appointment. From December 1993, women booking at St Thomas's Hospital, or in the surrounding community, were also included in the study. Information leaflets were available in seven languages as well as English.
At this booking appointment each woman's eligibility was checked by the midwife (see Appendix for selection criteria) and her written consent was sought. It was emphasised at this stage that women could receive extra visits at any time should they, or their caregivers, consider this to be necessary.
VISIT SCHEDULES
A visit was defined as an encounter between a pregnant woman and a midwife or doctor for the purpose of assessing maternal or fetal wellbeing. Day or inpatient admissions and visits solely for ultrasound or phlebotomy were not counted as visits. The schedules were described as “traditional” (13 visits—the control group) or “new style” (seven visits for nulliparous women and six visits for multiparous women—the study group). They were developed in discussion with obstetricians and midwives within Lewisham and Guy's Hospitals and therefore reflect a local agreement rather than the adoption of external recommendations. (See Appendix for timing of visits.)
All general practitioners within the Lambeth, Southwark and Lewisham Family Health Services Authority who normally referred women to one of the three hospitals were contacted by one of the two research midwives or the project leader. Eighty three out of 105 practices were visited in person. In all, 464 general practitioners (98%) agreed to take part. The study did not attempt to change the balance of professional involvement in women's antenatal care. At the beginning of their pregnancies all but 6% of women (who attended a hospital based midwives' clinic) were receiving shared care—that is, most of their care was given by general practitioners and midwives in the community, with occasional hospital visits.
RANDOMISATION
Randomisation was performed at the booking appointment with random permuted blocks of eight and 16, stratifying by the six offices at which the recruiting midwives were based (Lewisham, Guy's and St Thomas' antenatal clinics, Guy's and St Thomas' community midwives' offices, and the office of a midwifery group practice at Lewisham Hospital).14 Sequentially numbered, non-resealable opaque envelopes containing details of either the traditional or new style visit schedules were used. This number was then assigned to each woman in the trial. The woman's pregnancy health record (maternity notes) was labelled to indicate her number and the schedule to which she had been assigned, and a form giving brief details of her name, address, number, etc was returned to the project office.
MEASURES
Data relating to pregnancy related hypertensive disorders, smallness for gestational age, and other clinical variables, together with measures of health service use, were collected from the pregnancy health records by the two research midwives who were blinded to group allocation by paper covers put over each record. Pre-eclampsia was defined according to the criteria of the International Society for the Study of Hypertension in Pregnancy.15 Assessment of smallness for gestational age (<3rd centile and <10th centile) was made by plotting on centile charts the fetal abdominal circumference as measured by ultrasound scan16 and the baby's birth weight (using birth weight charts from Castlemead Publications, Welwyn Garden City). Twenty one per cent of records were reviewed by both research midwives; the overall interrater agreement was 98.6% (range for different variables 87.5% to 100%).
Women's views and psychosocial effectiveness were assessed by a maternal antenatal questionnaire at 34 weeks of pregnancy and a maternal postnatal questionnaire six weeks after birth. These questionnaires included the Edinburgh postnatal depression scale17 (which has been validated for use in pregnancy as well as postnatally18), the Cambridge worry scale (J Green et al, prenatal screening study, Cambridge), the baby adjective checklist (which contains 16 adjectives and from which the proportion of negative adjectives chosen to describe the baby is calculated),19 and the attitudes to the pregnancy and baby scale (which gives four scores; positive and negative attitudes to the fetus and positive and negative attitudes to the pregnancy),20 together with items from the Office of Population Censuses and Surveys's survey manual on women's experience of maternity care.21 The characteristics and views of women who chose not to participate in the trial were assessed by means of a non-participants' questionnaire devised specifically for the trial. Health professionals' views were ascertained before the trial began and during its last few weeks by using postal questionnaires devised for the trial. These were sent to all midwives, general practitioners, and obstetricians involved in the trial. All questionnaires used were piloted. Two postal reminders were sent at fortnightly intervals to non-responding women and health professionals.
SAMPLE SIZE
The intended sample size was based on the primary hypothesis. Review of the obstetric database at one of the hospital centres (Euroking, Guy's Hospital, 1991) indicated an incidence of 1% for caesarean section for pregnancy related hypertensive disorders. If this rate had increased by 1% or more (from 1% in the traditional group to 2% or more in the new style group) a minimum of 1415 women would have been needed in each group for the difference to be detected (95% significance level and power of 80%).22 The sample size needed to detect this one tailed effect was therefore 2830. Assuming a loss rate of not more than 10%, we estimated that 3144 women would need to be enrolled into the project.
ANALYSIS
Analysis was by intention to treat, using the Statistical Package for the Social Sciences (SPSS-PC),23 Confidence Interval Analysis,24 and Epi Info.25 To test the primary hypothesis a one tailed Fisher's exact test was used. Two tailed tests were carried out for all other variables, since the hypotheses to which they relate were not unidirectional. For continuous variables, Student's t test (for parametric variables) and the Mann-Whitney U test (for non-parametric variables) were used. For the continuous parametric variables, 95% confidence intervals were also calculated for differences between means but are not reported here. For categorical variables, odds ratios and 95% confidence intervals were calculated with Confidence Interval Analysis, except where there were small numbers, in which cases exact limits were calculated with Epi Info. Confidential interim analysis was performed.
Results
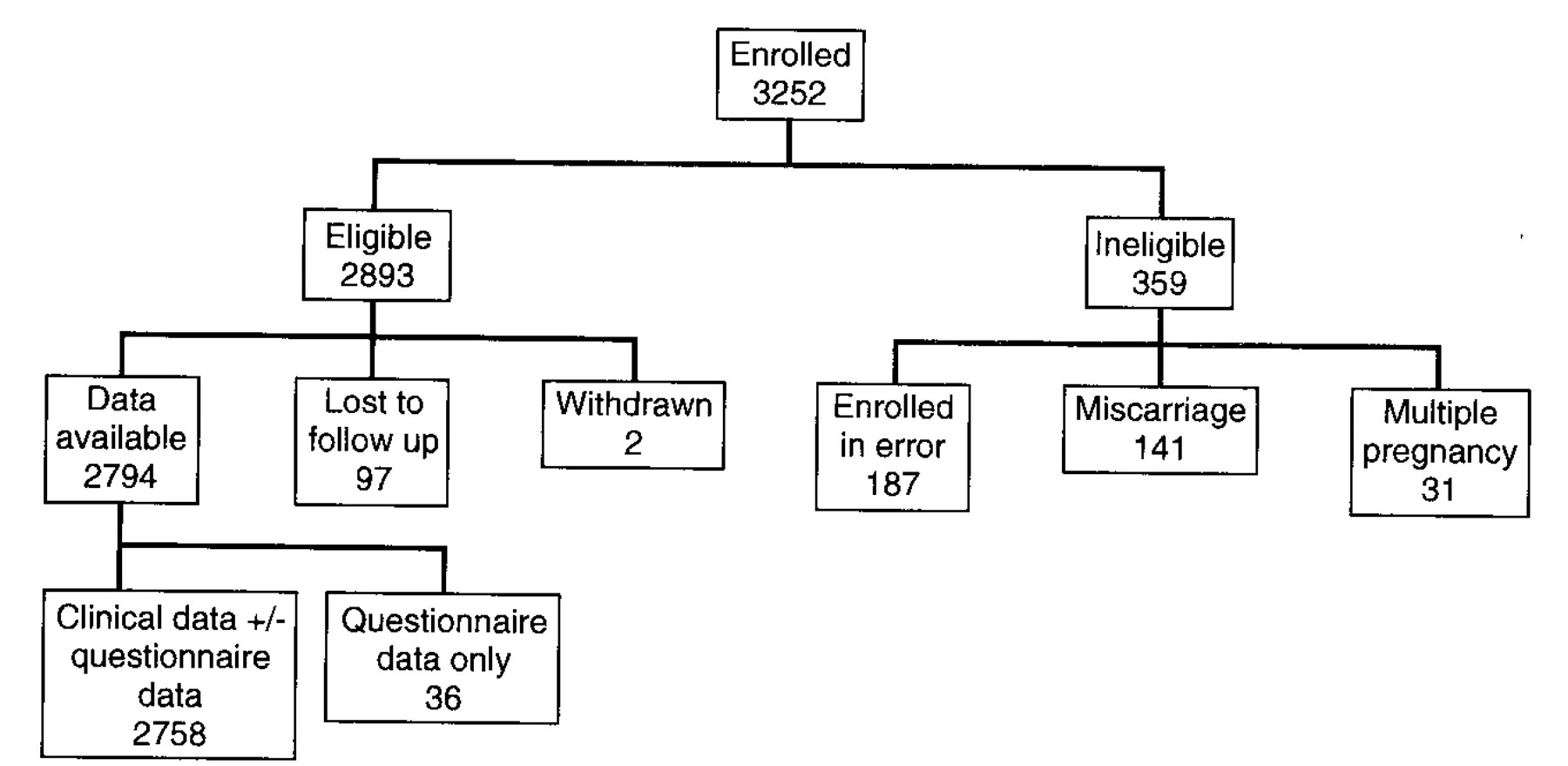
A total of 3252 women were enrolled into the trial, with 359 subsequently being excluded on grounds of ineligibility. Two women withdrew and did not wish to have any outcome data collected and 97 women were lost to follow up, leaving a final sample size of 2794 (traditional 1416, new style 1378; fig 1). Clinical data (with or without questionnaire data) were available for 2758 of these women; only questionnaire data were available for the remaining 36, whose pregnancy health records had been lost.
{kind=link}
When women were eligible to participate but chose not to, they were asked to complete the non-participation questionnaire at their antenatal booking visit. A total of 1162 non-participation questionnaires were returned, indicating that at least 26.3% of apparently eligible women invited to participate chose not to. A comparison of non-participants and participants showed that first time mothers (odds ratio 0.75; 95% confidence interval 0.65 to 0.86) and women from ethnic minority groups (0.59; 0.51 to 0.68) were less likely to participate. The most common reason, given by 75.7% (859/1134) of non-participants, was that they did not want fewer antenatal visits. Two hundred and thirty two of these women were asked for clarification of this decision: the two main reasons given were that they wanted extra reassurance (157; 68%) and ample opportunity to talk (87; 38%). Only a small minority gave concerns about the safety of reduced schedules (10; 4%) or seeing the reduced schedule as a health service cutback (9; 4%) as reasons for wanting traditional care.
Response rates to the maternal antenatal questionnaire and maternal postnatal questionnaire were 70.2% and 63.2% respectively. These rates are above those expected for an inner city area.21 Table 1 shows the characteristics of the study and control groups.
Characteristics of women in trial of schedules of antenatal visits. Values are numbers (percentages) for dichotomous variables and mean (SD) for continuous variables
The difference between the mean number of visits for the traditional group and the new style group was smaller than intended (2.2; 10.8 v 8.6) but still highly significant (P < 0.001). Calculation of the mean number of visits intended, adjusting for gestational age at booking and delivery, showed that women in the traditional group received an average of 1.65 visits fewer than intended, while those in the new style group received an average 2.60 more visits than intended.
CLINICAL VARIABLES
The two groups did not differ significantly in the primary variable of caesarean section rate for pregnancy related hypertensive disorders (traditional 14/1396 (1.0%), new style 11/1359 (0.8%); P=0.630).
Table 2 shows that there were no significant differences between the two groups for variables relating to pregnancy related hypertensive disorders, labour, maternal morbidity, or perinatal morbidity. Analysis of variables relating to smallness for gestational age showed a significantly lower incidence of antenatal suspicion of smallness for gestational age in women receiving new style care than in those receiving traditional care (odds ratio 0.73; 0.54 to 0.99). However, there were no significant differences in correct antenatal diagnosis of smallness for gestational age for birth weights either below the 3rd centile or below the 10th centile. One multiparous woman in the new style group died postnatally from a cerebrovascular accident, having attended 20 antenatal visits.
Clinical variables. Values are numbers (percentages) with odds ratios (95% confidence intervals) for dichotomous variables and mean (SD) with P value for continuous variables
ORGANISATIONAL VARIABLES
Women in the traditional group received significantly more ultrasound scans than did women in the new style group (1.7 v 1.6; P=0.003); they also had more day admissions (1.0 v 0.8; P=0.002). The number of antenatal inpatient admissions and the number of nights spent in hospital antenatally did not differ significantly (table 3).
Organisational variables
Regarding continuity of caregiver, women in the new style group saw significantly fewer caregivers (5.2 v 5.7; P<0.001) and received less conflicting advice (odds ratio 0.77; 0.62 to 0.95). They also, however, saw their usual caregiver fewer times (3.1 v 4.1; P<0.001) and were more likely to say that they did not feel remembered from one visit to the next (odds ratio 1.52; 1.25 to 1.89). There was no difference in the proportions who had met their intrapartum midwife during their antenatal care (0.93; 0.70 to 1.23).
PSYCHOSOCIAL VARIABLES
Information—The groups were similar in feeling encouraged to ask questions at their antenatal visit (1.12; 0.90 to 1.39), feeling that things had been explained well (0.91; 0.66 to 1.26), and in wanting more medical (1.16; 0.96 to 1.39) or general (1.04; 0.87 to 1.25) advice. They were also similar in whether they discussed their birth preferences at visits (1.09; 0.87 to 1.36), made a birth plan (1.11; 0.91, 1.34), attended antenatal classes (0.94; 0.78, 1.14), or read more than three books about pregnancy (1.14; 0.93 to 1.38). The maternal postnatal questionnaire asked if women would have liked to have known more about various aspects of childbirth and life with a new baby. The only difference found was that women in the new style group were more likely to wish they had known more about feeding their baby (285/846 (33.7%) v 232/843 (27.5%); odds ratio 1.34; 1.09 to 1.65).
Social support—Women in the new style group were less likely to feel listened to at visits (0.75; 0.60 to 0.95) and were more likely to say that they wanted more time talking at visits (1.26; 1.05 to 1.52). There were no differences in antenatal or postnatal depression scores (table 4).
Psychosocial variables. Values are numbers (percentages) with odds ratios (95% confidence intervals) for dichotomous variables and mean (SD) with P value for continuous variables
Worry—Women receiving new style care were significantly more worried during pregnancy about whether their baby was thriving (1.7 v 1.5 (maximum score 5); P=0.010). Postnatally they were also more worried about coping with their baby (0.6 v 0.5 (maximum score 5); P=0.014; table 4).
Attitudes to fetus and baby—Women receiving new style care were found to have a more negative attitude to their fetus: they rated themselves as feeling more detached, concerned, and uncertain about their unborn baby (6.6 v 6.0 (maximum score 21); P=0.002). This effect continued into the postnatal period, when women in the new style group chose a higher proportion of negative words to describe their baby than women in the traditional group (0.207 v 0.188; P=0.028).
Health related behaviour—Women in the two groups did not differ significantly in whether they smoked (odds ratio 1.18; 0.95 to 1.47) or in their reported alcohol consumption in late pregnancy (P=0.854). There were also no differences in the proportions of women who gave up breast feeding (odds ratio 1.14; 0.90 to 1.44) or never started (0.99; 0.79 to 1.25).
Birth experience—The two groups did not differ in any variables relating to the birth, such as antenatal confidence about giving birth (P=0.374), satisfaction with the birth (P=0.777), or self ratings of coping with giving birth (P=0.815).
ACCEPTABILITY OF VISIT SCHEDULE
Women—For the purposes of this study we classified women as dissatisfied if, in the new style group, they would have preferred more visits or if, in the traditional group, they would have preferred fewer visits. Dissatisfaction is therefore a preference in the direction of the alternative type of care. Women in the new style group were much more likely to be dissatisfied with the number of visits they received than women in the traditional group (odds ratio 2.50; 2.00 to 3.11; table 5). This disparity in satisfaction was most evident in early pregnancy but persisted into the postnatal period (2.41; 1.90 to 3.07). Women's reporting of their partners' views (where an opinion was expressed) showed greater dissatisfaction in the new style group (10.75; 7.23 to 15.99). Women in the new style group were also more likely to feel that some of the gaps between visits were too long (2.20; 1.83 to 2.66). Although a greater proportion of women receiving new style care said they would choose the same schedule in a future pregnancy (1.41; 1.16 to 1.71), women in the traditional group rated their antenatal care more highly (3.8 v 3.6 (maximum score 5); P<0.001).
Acceptability variables
Professionals—The response rate for the questionnaire sent to all health professionals at the end of the trial was 62%. The majority (187/229; 82%) of professionals who replied reported that they would like to see a reduction (from the traditional 13 visits) in the overall number of routine antenatal visits. The remainder would not like to see a reduction (17; 7%) or were undecided (25; 11%). However, professionals were of the opinion that traditional care met the non-clinical needs of nulliparous women better than new style care (53% v 22%).
Discussion
This study is the first European randomised controlled trial specifically comparing different visit schedules in antenatal care. By its multidisciplinary approach, it gives weight to measures of both clinical and psychosocial effectiveness, as well as measuring the acceptability of the two schedules of visits to women and caregivers. An unpublished trial from Zimbabwe looked at different visit schedules (S P Munjanja, Royal College of Obstetricians and Gynaecologists' safe motherhood conference, London, 1992).
Our study, carried out in an area of considerable ethnic diversity with pockets of high socioeconomic deprivation, presented many logistical problems, not least of which was the coordination of the many maternity care providers involved. Despite these difficulties, the measured difference in the number of visits received between the two groups was similar to that found when Hall and colleagues compared the effects of their complete organisational change with historical controls (a fall from 11.2 visits in 1975 to 8.7 in 1981-2).2 It was also similar to the difference found in the study of Binstock and Wolde-Tsadik (11.3 v 8.2).11
LIMITATIONS OF THE STUDY
We accept the problems associated with choosing a proxy measure for the morbidity associated with pregnancy related hypertensive disorders. The many potential influences on caesarean section rates are well documented.26 The final sample size was marginally lower than intended, which meant that we were able to test the primary hypothesis with a power of only 79.6% rather than 80%. The primary hypothesis on which the sample size was based was unidirectional, reflecting the concern of clinicians that a new style of care should not lead to an increased caesarean section rate for pregnancy related hypertensive disorders. The interesting possibility that new style care might lead to a decrease in the primary variable was not tested; this would require a substantially larger sample size. Furthermore, our sample size precludes examination of rare but serious events such as perinatal loss, eclampsia, and maternal mortality.
We made no attempt to examine the economic aspects of care, nor was it possible in a randomised controlled trial to examine fully the impact that widespread introduction of our intervention might have. Should reduced antenatal visit schedules be introduced for the majority of women there may, for example, be benefits for women and health professionals resulting from the extra time available. As the women following the new style schedule formed a minority of the total pregnant population in south east London at the time, any such effects could not be measured.
Our study also illustrates the difficulties of maintaining changes in delivery of services in a pragmatic trial. That the difference in the number of visits actually received was smaller than intended also needs to be borne in mind when interpreting the findings. We were unable to identify the reasons for the convergence seen between the two groups in the mean number of visits received, although we expected that medical problems arising during pregnancy and women changing their booking for maternity care to other hospitals would lead to some non-adherence to the schedules. Women's responses to open ended questions on the maternal antenatal questionnaire suggested that the convergence in the mean number of visits received was the result of non-adherence to the schedules by both women and professionals.
CLINICAL EFFECTS
Our findings confirm that, for the clinical variables examined, new style care is as effective as traditional care. This supports the conclusions reached from observational data, both internationally9 and in the United Kingdom.2
It is interesting that women in the traditional group had more antenatal ultrasound scans and day admissions. The first of these findings replicates that of Binstock and Wolde-Tsadik.11 These extra scans and day admissions may have been associated with the higher index of suspicion of smallness for gestational age among clinicians caring for women in the traditional group. This increased use of resources was not associated with any other measurable clinical effect, beneficial or otherwise.
DISSATISFACTION
Women were more likely to be dissatisfied with the number of visits in new style care than the number in traditional care. Over half of the women in the group receiving new style care felt that some of the gaps between antenatal visits were too long. Although more women in this group said that they would choose the same schedule in future, this indirect measure of satisfaction involves speculation about future feelings and is less relevant than the dissatisfaction women reported in their current pregnancy. This dissatisfaction may be due to their feeling that they were less likely to feel listened to and that they were less happy with the time they had to talk at visits, than women receiving traditional care. Since non-participants' dissatisfaction with the idea of new style care also needs to be taken into consideration, it is important to remember that 26% of apparently eligible women chose not to participate, mainly because they did not wish to have fewer antenatal visits. The major problem with the new style schedule seems to be its lack of acceptability to women. Dissatisfaction is important because of the increasing importance accorded to patients' views in health care evaluation, together with the high priority it has been given in Changing Childbirth.10
Although it is clear that, in the context of this trial, women in the new style group were more dissatisfied, it is not known whether this dissatisfaction would persist if new style care became the norm. There is evidence from surveys of preference and satisfaction that individuals tend to be happier with existing rather than new forms of care.27 Widespread implementation of new style care may change expectations, and with them, satisfaction with care, but there is no evidence that this would be the case.
PSYCHOSOCIAL EFFECTIVENESS
The findings relating to the psychosocial effectiveness of the two schedules need careful interpretation. Although the reported differences in psychosocial effectiveness between the groups are significant, the magnitude of the differences is small. We recognise that, when multiple comparisons are made, some findings will occur by chance. However, since all the differences in psychosocial effectiveness are in the same direction—that is, in favour of traditional care—and since they tend to cluster together around similar concepts such as feelings about the fetus or baby and talking or listening, we feel that the differences in psychosocial effectiveness are meaningful. It should also be borne in mind that health professionals in the trial felt that traditional care was better than new style care for meeting the non-clinical needs of nulliparous women.
That significantly more women receiving new style care wanted more time talking at visits is indirect evidence supporting Hall et al's finding that reducing the number of antenatal visits does not lead to any increase in consultation length.2 We have reported elsewhere that, among maternity caregivers, longer antenatal consultations were the least supported of a number of possible changes in antenatal care.28
Our findings on continuity confirm those of Hall et al that reducing the number of visits leads to reductions in the number of different caregivers seen.2 We were able to show that, although this led to a decrease in conflicting advice, it also led to women feeling less well remembered from one visit to the next. This may be because they saw their usual caregiver fewer times.
CHANGES IN CARE SCHEDULES
Any policy changes in antenatal care should aim to maintain current levels of safety and psychosocial support for women. Since the two schedules in this trial were equally effective on all the clinical variables measured, providers may decide to offer women fewer visits than traditionally scheduled. However, we have shown that a reduced schedule of care is less effective psychosocially and less acceptable to women, even though women in the trial were encouraged to book extra appointments if they felt them to be necessary. Women may find it difficult to justify, both to their caregivers and to themselves, the use of health professionals' time for non-clinical, but important, reasons such as the need for support, information, or reassurance.
If fewer antenatal visits are to be offered, it is important to ensure that women feel able to have extra visits for psychosocial reasons, not solely when visits are clinically necessary. Flexible patterns of visits that are tailored to individual needs might be developed. It may also be useful to develop forms of care, other than the routine antenatal visit, for meeting women's psychosocial needs in pregnancy. Whatever system of antenatal care is adopted, or retained, it is important that it is evaluated to ensure that a high quality of service is provided to women.
Further research on antenatal visit schedules would permit the use of meta-analysis to clarify the effect of reduced schedules on rare clinical problems such as eclampsia and perinatal mortality; it should also address the health economic implications of different schedules. In addition, future studies might usefully focus on the acceptability and psychosocial effects of reduced schedules in other service contexts, such as in midwifery group practices, or in conjunction with alternative sources of support, information, and reassurance. Finally, research will be required to evaluate any development of flexible, individualised approaches to antenatal care.
We thank the women who took part in our study and gave us their views on the care they received. We are also grateful to our secretarial and clerical staff, Maureen Statham and Becky Green, and all the midwives, general practitioners, obstetricians, and administrative staff whose cooperation ensured the completion of the trial. We thank the many individuals who gave valuable advice and help throughout the trial, in particular our steering committee. JS thanks his partners, Drs H Graver, B Essex, A Platman, and S Thomas, for supporting his research interest.
Appendix
SELECTION CRITERIA
Women had a pregnancy of no more than 22 weeks' gestation at booking, estimated from the first day of the last normal menstrual period
Pregnancy had reached 24 weeks' gestation
Women were registered as patients of general practitioners agreeing to participate in the project
Women were booked for delivery at Lewisham, Guy's, or St Thomas's Hospitals or at home
Women had a reasonable understanding of, or literacy in (as considered by the midwife doing the enrolment), one of the following: English, Turkish, Vietnamese, Punjabi, Bengali, Cantonese, Spanish, or Portuguese
Women of low antenatal risk—that is, not excluded by clinical exclusion criteria:
Booking for specialist obstetric care (more than three routine antenatal visits to an obstetrician planned)
History of:
Previous fetal loss (18 weeks' gestation or later)
Previous neonatal death
Three or more consecutive spontaneous abortions
Cervical suture in a previous pregnancy
Baby born prematurely at less than 34 weeks' gestation
Baby weighing less than 2.5 kg
Severe pregnancy related hypertensive disorder with proteinuria in last pregnancy
Severe non-proteinuric hypertension requiring induction of labour, medication, or epidural for raised blood pressure in last pregnancy
Previous myomectomy or classical caesarean section
Essential hypertension, defined as having a diastolic blood pressure >90 mm Hg at booking, or given as part of medical history by woman in booking interview
Diabetes mellitus
Renal disease
Cardiac disease
Previous postnatal depression requiring medication (including puerperal psychosis)
Previous cone biopsy
Rhesus or ABO incompatibility antibodies in a previous pregnancy
Assisted conception, other than treatment with clomiphene alone
Women currently:
Being treated for tuberculosis
Taking drugs for a psychiatric disorder
Aged <16 or >/=40 years of age
Known substance abuser
Weighing less than 41 kg (for Asians), 47 kg (Afro-Caribbeans), or 45 kg (any other ethnic group)
Weighing more than 100 kg
With a multiple pregnancy
TIMING OF VISITS
Traditional-booking, 16, 20, 24, 28, 30, 32, 34, 36, 37, 38, 39, 40 weeks
New style (nulliparous)-booking, 24, 28, 32, 36, 38, 40 weeks
New style (multiparous)-booking, 26, 32, 36, 38, 40 weeks
Footnotes
-
Funding Primary Care Development Fund, South Thames Regional Health Authority, with additional funding from the Lambeth, Southwark and Lewisham Health Commission.
-
Conflict of interest None.