
Abstract
Introduction: COVID-19 policies such as quarantining, social isolation, and lockdowns are an essential public health measure to reduce the spread of disease but may lead to reduced physical activity. Little is known if these changes are associated with changes in physical or mental health.
Methods: Between September 2017 and December 2018 (baseline) and March 2020 and February 2021 (follow-up), we obtained self-reported demographic, health, and walking (only at follow-up) data on 2042 adults in primary care with multiple chronic health conditions. We examined whether the perceived amount of time engaged in walking was different compared with prepandemic levels and if this was associated with changes in Patient-Reported Outcomes Measurement Information System-29 mental and physical health summary scores. Multivariable linear regression controlling for demographic, health, and neighborhood information were used to assess this association.
Results: Of the 2042 participants, 9% reported more walking, 28% reported less, and 52% reported the same amount compared with prepandemic levels. Nearly 1/3 of participants reported less walking during the pandemic. Multivariable models revealed that walking less or not at all was associated with negative changes in mental (ß = −1.0; 95% CI [−1.6, −0.5]; ß = −2.2; 95% CI [−2.9, −1.4]) and physical (ß = −0.9; 95% CI [−1.5, −0.3]; ß = −3.1; 95% CI [−4.0, −2.3]) health, respectively. Increasing walking was significantly associated with a positive change in physical health (ß = 1.3; 95% CI [0.3, 2.2]).
Conclusions: These findings demonstrate the importance of walking during the COVID-19 pandemic. Promotion of physical activity should be taken into consideration when mandating restrictions to slow the spread of disease. Primary care providers can assess patient’s walking patterns and implement brief interventions to help patients improve their physical and mental health through walking.
Introduction
The COVID-19 policies that restrict movement such as quarantining, social isolation, and lockdowns are an essential public health measure to reduce the spread of disease. However, these same restrictions may have unintentionally reduced some forms of physical activity, such as walking. Walking is one of the most popular form of physical activity, where an estimated 60% of adults walk at least 10 minutes for exercise each week.1,2 Walking has also been shown to improve anxiety, depression, and physical function.3,4,5,6 Recent research has shown that walking dramatically declined in the early stages of the pandemic.7 Little is known if the pandemic’s restrictions changed walking habits among patients with multiple chronic conditions (MCC) and its impact on their health. This study sought to investigate the relationship between walking habits during COVID-19 and health among primary care patients with MCC.
Methods
Between September 2017 and December 2018 (baseline) and March 2020 and February 2021 (follow-up), we obtained self-reported demographic, health, and walking (only at follow-up) data on 2042 adults from a multi-center randomized control trial that spanned 41 primary care practices in 13 states, described elsewhere.8 All participants evidenced utilization of primary care and at least 1 chronic medical and behavioral health condition, or at least two chronic medical conditions from the following list: heart disease, diabetes, lung disease, arthritis, mood disorder, insomnia, substance abuse, chronic pain, or irritable bowel syndrome. Electronic health records were used to determine eligibility.
The primary outcomes were the change in mental and physical health summary scores calculated from the Patient-Reported Outcomes Measurement Information System-29 (PROMIS-29).9 Scores are standardized to the US population with mean of 50 and standard deviation of 10. Higher scores indicate better functional health.
The primary predictor was perceived changes in walking habits from pre- and during COVID-19 (Table 1). A secondary predictor was the time reported per walking trip.
Walking Habits During COVID-19
Baseline health status as measured by the PROMIS-29 was included as a covariate in the models. Other covariates considered were age, sex (male vs female), race (White vs other), ethnicity (Hispanic vs non-Hispanic), marital status (married or living-as-married vs not), employment status (employed full-time, part-time, student or homemaker vs not), annual household income household income (<$30,000 vs ≥$30,000), education (high school graduate or less vs associates degree or more), the number of qualifying chronic conditions, and census-tract Social Deprivation Index (SDI)10, population density, and rural status measured by the Rural Urban Commuting Areas (RUCA) codes.11
Statistical Analysis
Multivariable linear regression was used. If a covariate changed the coefficient on walking by more than ±10% in a model with no other covariates, it was included in the final model as a potential confounder. All tests were 2-tailed; the threshold for statistical significance was P < .05. Stata 16.1 (StataCorp, College Station, TX) was used for data management and statistical analysis. All study procedures were approved by The University of Vermont Committees on Human Research (CHRMS#16 to 554). Informed consent was provided by all study participants.
Results
The median time between baseline and follow-up surveys was 636 days. The average age of participants was 64. The majority were female (66%), non-Hispanic (93%), White (78%), unmarried (53%), and unemployed or retired (67%), with half (50%) having an annual income less than <$30k/year. Most lived in urban (80%) and moderately deprived areas. The median number of chronic conditions was 4 (interquartile range = 3–5).
At the time of the survey, 49% of participants walked for 3 of the past 7 days for at least 10 minutes; 22% reported not walking at all and 25% reported walking all 7 days. Overall, the median reported walk-time was 25 minutes. Of 2042 participants, 9% reported more walking, 28% reported less, and 52% reported the same amount compared with prepandemic levels. Participants that walked less were younger and more likely to be female and nonwhite than participants that walked the same amount since the pandemic began (Table 2).
Participant Characteristics (n = 2042)
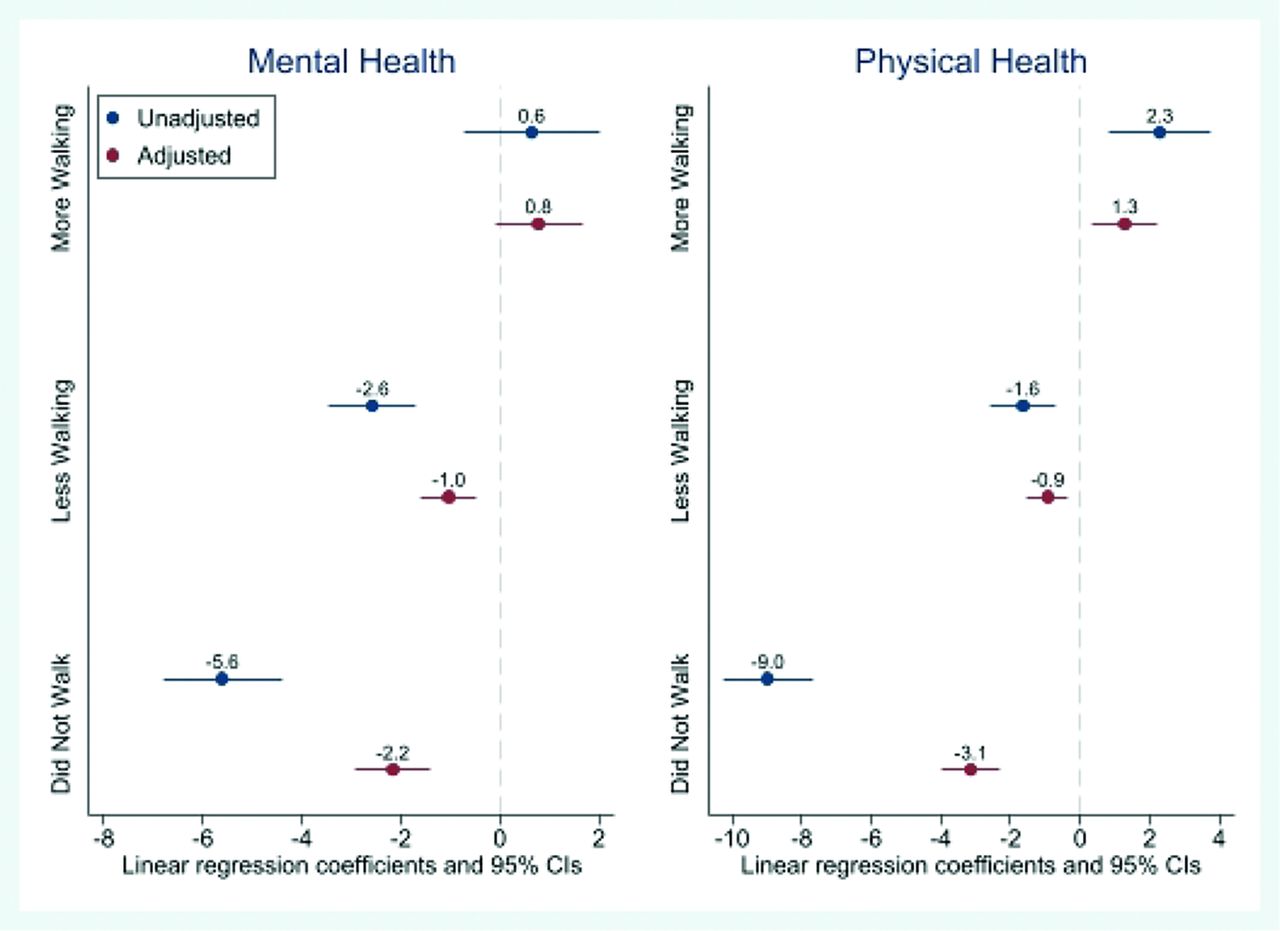
After adjustment for age, sex, race, income, ethnicity, marital status, employment status, rurality, SDI, population density, baseline mental and physical health scores, and number of chronic conditions, reducing walking during the pandemic was significantly associated with a negative change in mental (ß = −1.0; 95% CI [−1.6, −0.5]) and physical (ß = −0.9; 95% CI [−1.5, −0.3]) health scores compared with walking the same amount before the onset of the pandemic. However, increasing walking was significantly associated with a positive change in physical health scores (ß = 1.3; 95% CI [0.3, 2.2]). Not walking at all was significantly associated with deteriorating mental and physical health (Figure 1).

Unadjusted and adjusted change in mental and physical health associated with changes in walking during the COVID-19 pandemic. Higher scores indicate better health. Abbreviation: CI, confidence interval.
A secondary analysis controlling for the same covariates revealed that increased walking time was linearly associated with improvement in mental and physical health scores. Specifically, after adjustment for age, sex, race, income, ethnicity, marital status, employment status, rurality, SDI, population density, baseline mental and physical health scores, and number of chronic conditions, for each additional 10 minutes of reported walking time, mental and physical health improved by (ß = 0.17; 95% CI [0.11, 0.22]) and (ß = 0.41; 95% CI [0.34, 0.49]), respectively.
Discussion
Our results demonstrate the importance of walking during the COVID-19 pandemic. Nearly a third of individuals were walking less than before the pandemic and reductions in walking were negatively associated with mental and physical health. Those walking more during the pandemic reported better health compared with the other groups. Our results are similar to those of other studies.12,13
There are likely several mechanisms that explain the changes in walking during the pandemic and the associated effects on health. We did not collect information on how restrictions affected walking habits and therefore cannot be sure if this was the mechanism of reduced walking. However, a recent study showed that walking attitudes were negatively impacted by the pandemic. The same group also found that perceived built environment was also associated with walking and health, and that these relationships varied by day of week.14 Another group found that walking a dog during the pandemic significantly reduced social isolation caused by the pandemic.15
This study had limitations. Participants could have been engaged in other forms of exercise besides walking that we did not ask about. However, walking is 1 of the most common forms of exercise among adults.1 Self-report of walking is subject to recall bias and the primary predictor of change in walking habits is unvalidated. The results may not be generalizable beyond primary care patients with multiple chronic conditions who tend to be older women. However, these populations are particularly vulnerable to the adverse effects of COVID-19 lockdowns.16 Although we only have data from 13 states, they do represent each region of the country. A major strength of this study was the ability to control for prepandemic health.
Promotion of physical activity should be taken into consideration when mandating restrictions to slow the spread of disease. Primary care providers can assess patient’s walking patterns and implement brief interventions to help patients improve their physical and mental health through walking.
Notes
This article was externally peer reviewed.
Conflict of interest: None.
Funding: This work was funded through a Patient-Centered Outcomes Research Institute (PCORI) Award (PCS-1409-24372). The views, statements, and opinions presented are solely the responsibility of the authors and do not necessarily represent the views of PCORI, its Board of Governors, or its Methodology Committee.
To see this article online, please go to: http://jabfm.org/content/35/5/000.full.
- Received for publication March 3, 2022.
- Revision received May 11, 2022.
- Accepted for publication June 10, 2022.





{kind=link}