
Abstract
Purpose: There is considerable interest in the association between food insecurity (FIS) and various cardiovascular risk factors such as dyslipidemia. Although the association between FIS and dyslipidemia has been studied across various methodologies and populations, there is no comprehensive systematic review and meta-analysis of these data.
Methods: A systematic literature search was conducted. Cross-sectional peer-review studies assessing the association between FIS and dyslipidemia were identified. Data extracted included population characteristics, study sizes, covariates explored, and laboratory assessments of dyslipidemia. Effect sizes were extracted or calculated, then synthesized across studies using a random effect model, and the heterogeneity, publication bias, and subgroup dependence for each meta-analysis were assessed.
Results: For adults, meta-analysis demonstrated no significantly elevated odds for FIS individuals to have a concomitant abnormal lipid measurement. Covariate-unadjusted analysis of standardized mean differences showed no significant differences in lipid measurements between food-insecure and food-secure individuals. In contrast to quantitative laboratory results, food-insecure patients were more likely to self-report previous diagnoses of dyslipidemia.
Conclusions: Although current data do not suggest an association between FIS and dyslipidemia, more longitudinal studies and studies targeting women, children, the elderly, and patients with chronic diseases such as diabetes are needed to further address this issue.
- Cholesterol
- Chronic Disease
- Cross-Sectional Studies
- Dyslipidemias
- Food Insecurity
- Hunger
- LDL Triglyceride
- Risk Factors
- Social Determinants of Health
Background
Food insecurity (FIS) is a complex phenomenon that generally refers to inadequate access to food of sufficient nutritional quality to promote health.1 FIS can be due to a wide range of factors including poverty, access to public resources like transportation, and the presence of food deserts.2⇓⇓–5 It is for this reason FIS has been linked to other important and well-established social determinants of health such as race, income level, housing, disability, and citizenship status.6⇓⇓⇓–10
In addition to its relevance to various social determinants of health, multiple mechanisms have been proposed for a link between FIS and cardiovascular disease.11⇓⇓–14 One possible link is mediated through cardiovascular risk factors such as high blood pressure, diabetes, and dyslipidemia.12,14 For dyslipidemia, there are at least 2 potentially off-setting effects of FIS on patients' lipid measurements. The first is that FIS leads to nutritionally poor diets (ie, increased intake of foods high in saturated or trans fats and/or low in fiber) that may be further complicated or exacerbated by cultural and socioeconomic factors.15⇓–17 In contrast, a subset of severely food-insecure patients may consume overall fewer calories than their food-secure counterparts, which may lead to improved lipid measurements.18,19 It remains unclear if the strength of such associations (effect sizes such as odds ratios [ORs] or standardized mean differences [SMDs]) is either measurable or clinically significant.
As both FIS and dyslipidemia each have high prevalence5,20⇓⇓⇓⇓⇓⇓–27 and well-documented deleterious health effects,28⇓⇓⇓⇓⇓⇓⇓⇓⇓–38 identifying an association between the 2 factors could have relevance to clinicians. As a result, there has been considerable effort in the literature to measure the possible association between FIS and dyslipidemia in a number of cross-sectional studies spanning diverse populations and various lipid markers such as total cholesterol (TC), low-density lipoprotein (LDL), triglycerides (TG), and high-density lipoproteins (HDL).39 However, there has yet to be a comprehensive systematic review and meta-analysis to synthesize these results.
Methods
Data Sources
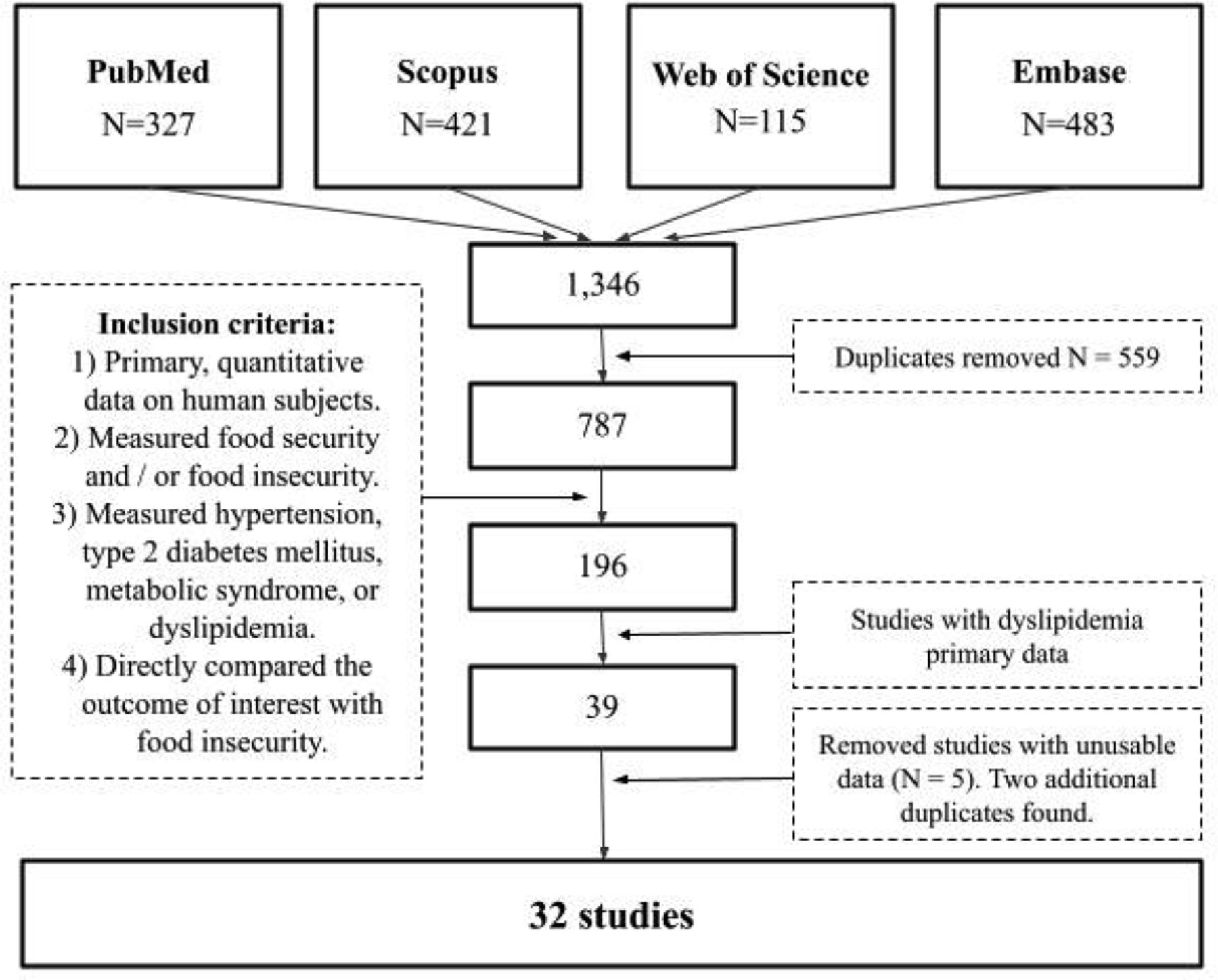
This systematic review and meta-analysis is the result of an initially broad, systematic literature search investigating the link between FIS and cardiometabolic risk factors. The initial search was registered in Prospero as of January 28, 2020 (registration CRD42020149560) and included all peer-reviewed human studies involving any population, any methodology, and any publication year in 4 databases: PubMed, Scopus, Embase, and Web of Science. The initial search took place on September 9, 2019 and involved the Medical Subject Headings of FIS with hypertension, diabetes, metabolic syndrome, and dyslipidemia.
Study Selection
Every abstract obtained in the initial search described above was randomized and screened using Abstrackr40,41; 4 authors inspected for relevance. Relevance was defined as: (1) the study investigated FIS or a comparable concept, (2) the study also investigated hypertension, diabetes, metabolic syndrome, or dyslipidemia, (3) the study reported quantitative primary data, and (4) the study was peer reviewed and available in English. Articles that were excluded by all 4 authors were discarded; those with approval from at least 1 author were further discussed and reviewed by an additional author. Interrater reliability was assessed for the entire group and permutations of reviewer pairs.42 Studies that satisfied the above conditions were then screened by at least 2 authors to identify those that contained primary data exploring direct associations between FIS and dyslipidemia; studies that contained data only through a third variable were discarded. Disagreements were revisited by an additional author. Included studies were then assessed through the AXIS tool for quality assessment of cross-sectional studies43 to assess for individual-study biases.
Data Extraction
Every study identified that met the above inclusion criteria underwent manual extraction of study population characteristics, sample size, study design, measurements, and all outcomes related to FIS and dyslipidemia. Extracted data were grouped by the measured outcomes available from each study in its relationship to FIS: LDL, HDL, TC, and TG. Based on the available primary data, meta-analyses were possible on ORs and SMDs (specifically Hedges' g). Effect sizes were extracted by 1 author and, when not reported in a study, were calculated manually using the study's reported primary data. Regarding studies that separated outcomes by FIS categories (ie, mild vs severe FIS), the primary data were either pooled to calculate 1 effect size or, if applicable, reported effect sizes were combined using the random effects (RE) model. More information on how studies were grouped can be found in the Online Appendix figures and tables.
Data Synthesis and Meta-Analysis
Meta-analyses were conducted only when 3 or more effect sizes were available from separate studies on a specific outcome measure. Analysis was conducted using the metafor package in R based on the RE size model, which does not assume sampled populations have identical probability distributions.44 Meta-analysis results were calculated using the DerSimonian-Laird estimator.45 For OR meta-analysis, the logarithm was used as the effect size. For each meta-analysis, study heterogeneity was calculated via the total variance (Q), the degrees of freedom (df), and the I2 statistic.46 Publication bias was evaluated by the Begg and Mazumdar rank correlation test for funnel plot asymmetry as well as Kendall's τ in Egger's regression test.47,48
Results
Study Characteristics
A total of 787 abstracts were reviewed by 4 authors, with significant group interrater agreement: Fleiss kappa = 0.68 [95% CI, 0.66, 0.71, n = 4] with each user having permutated interrater agreements above 0.6. One hundred ninety-six abstracts were then full-text evaluated, and 32 manuscripts were found to have primary data exploring the association between dyslipidemia and FIS (Online Appendix Figure 1). All studies identified in a previous 2017 preliminary nonmeta-analysis review were also discovered on this review.39 All studies had either a cross-sectional design or contained data specific to FIS that corresponded to baseline characteristics from a cohort study. Most studies were from the US, which had the highest number of patients; Malaysia and Iran were the other most represented countries.

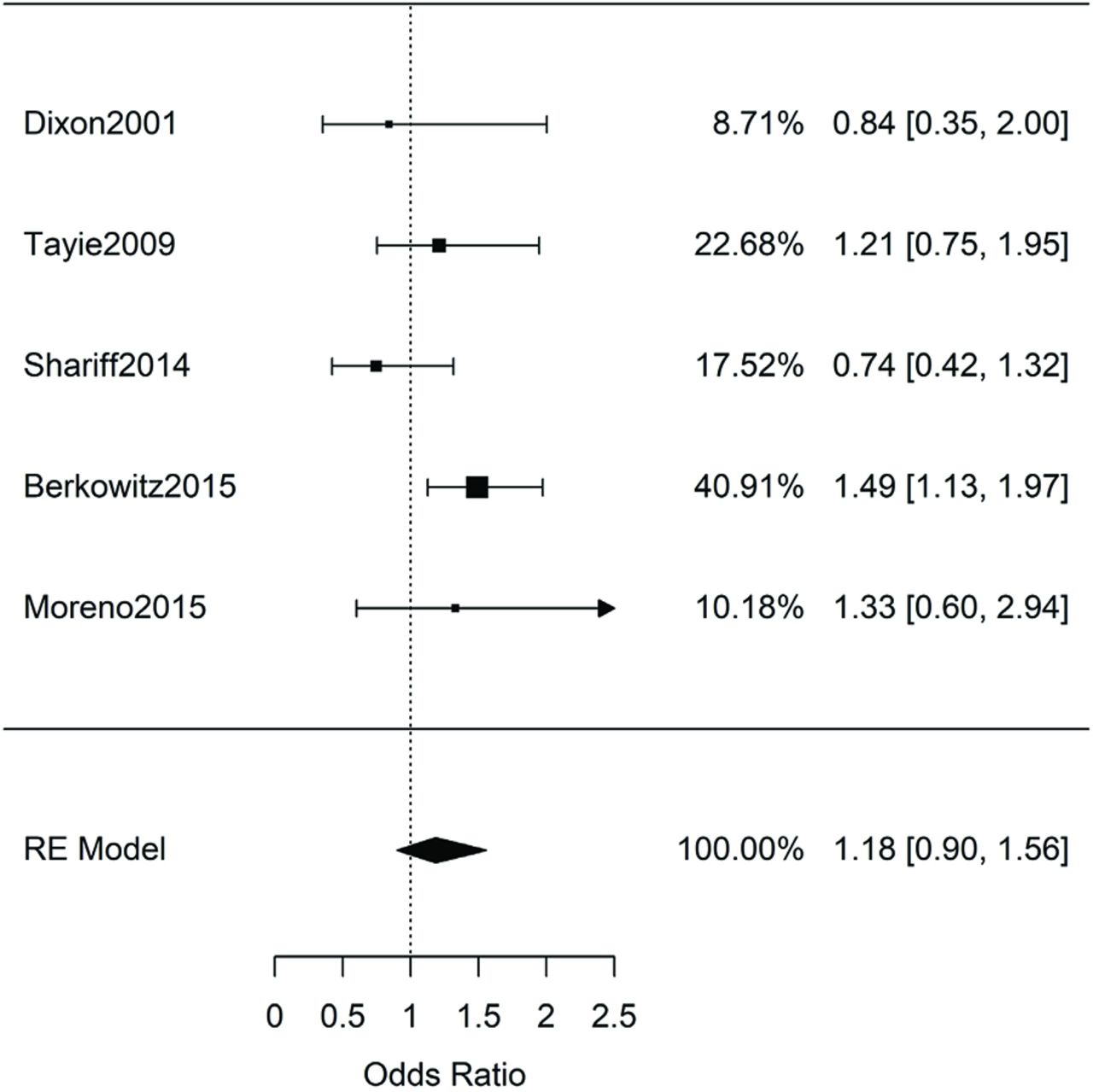
Meta-analysis of adult studies investigating increased odds of elevated low-density lipoprotein (LDL) for food-insecure patients. Synthesis of the 5 studies resulted in a nonsignificant combined odds ratio of 1.18 [95% CI, 0.90-1.56, n = 22,746, Q(df = 4) = 5.5, I2 = 27%].
Twenty-five studies presented data on adults,12,19,49⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓–71 5 presented data on children,72⇓⇓⇓–76 and 2 studies had data on both.64,77 Twenty-six studies presented lab measurements for 1 (or a combination) of LDL, TG, TC, or HDL; 5 studies exclusively used only self-reports of previous diagnoses of dyslipidemia; 1 study used general nonspecific diagnosis of hyperlipidemia from chart review.75 The characteristics of each study are presented in Online Appendix Tables 1–11. These tables divide studies based on child/adult status, dyslipidemia measurements, and choice of effect size (OR, SMD). Each table indicates where in the manuscript the original information was located and whether we calculated the effect sizes ourselves by extracting primary data. We noted manuscripts with overlapping patient data and those for which we could not extract nor calculate effect sizes.
For children, the few identified studies (Online Appendix Tables 9 and 10) did not have sufficient overlap to perform any meta-analysis. In short, the data from some studies suggested associations between FIS and specific dyslipidemia measurements,72 while others did not.64,74,76 One study presented data on both children and adults but was not analyzed due to inability to separate the data from the 2 groups.77
In adults, the available literature data allowed for 8 meta-analyses to explore the association of FIS with dyslipidemia: by 4 lab measurements (LDL, HDL, TC, TG) and with 2 different effect sizes (OR and SMD). As some studies had partially overlapping data (depending on population and/or measurement modality and reporting), the total number of manuscripts and sample size used for each meta-analysis will be discussed in the subsections below.
Results of Individual Studies and Synthesis of Results by Dyslipidemia Measurement
LDL
We first analyzed studies that explored the association between food insecurity and elevated LDL measurements. The 5 studies (n = 22,746) that reported the adjusted ORs were combined for meta-analysis in Figure 1. Synthesis of the results revealed no significant association between FIS and elevated LDL: ORLDL = 1.18 [95% CI, 0.90–1.56, n = 22,746, Q(df = 4) = 5.5, I2 = 27%]. All of these studies adjusted for various covariates such as age, sex, gender, and, in some cases, body mass index (BMI) or adiposity (Online Appendix Table 1). One study was excluded from the meta-analysis above as it involved overlapping National Health and Nutrition Examination Survey data (Online Appendix Table 1).51
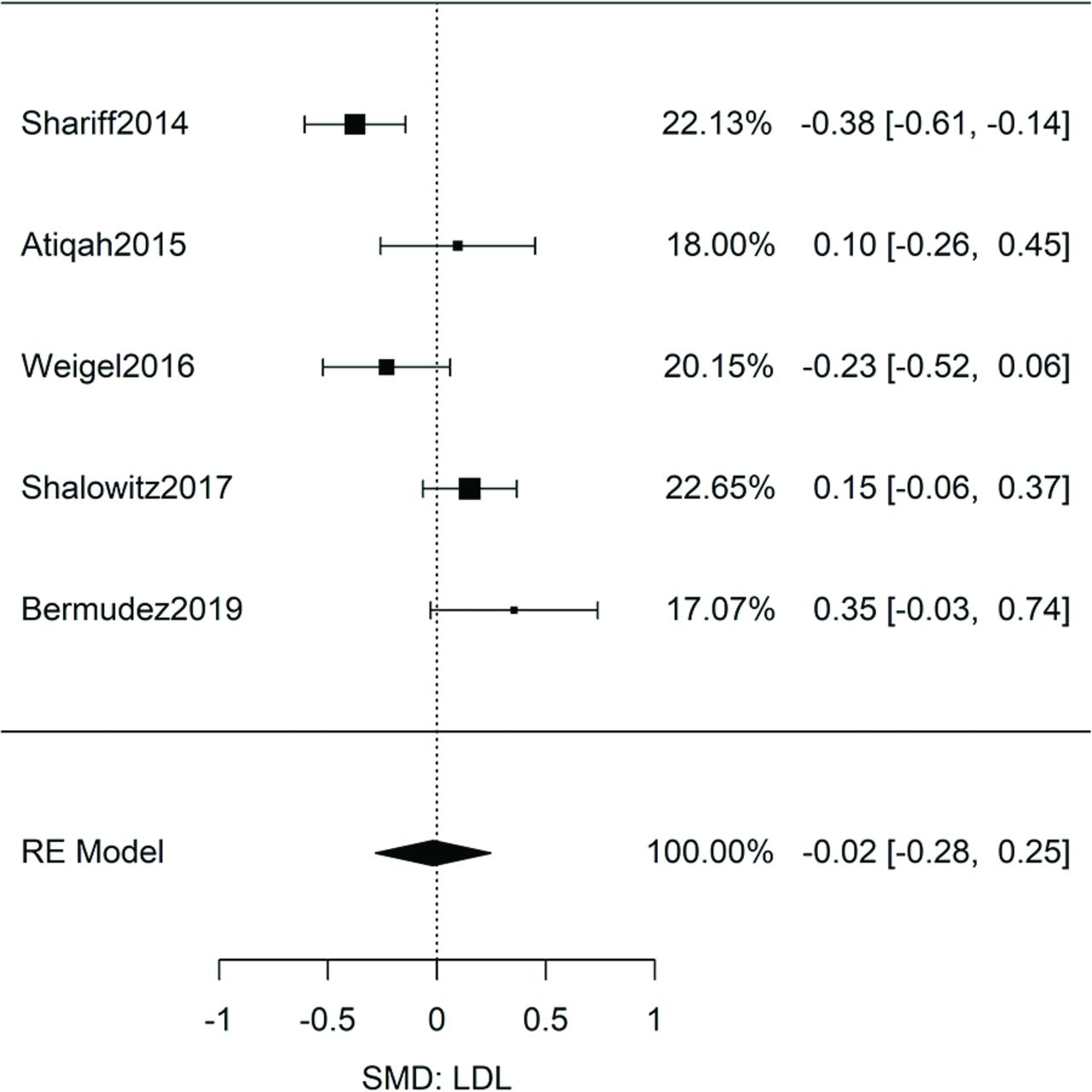
Five additional studies (n = 1,143) reported sufficient data to calculate the SMD in LDL levels between food-insecure and food-secure adults (Online Appendix Table 2). Although these data were not adjusted for covariates, synthesis also resulted in no significant difference in LDL levels between food-secure and food-insecure patients: gLDL = −0.02 [95% CI, −0.28, 0.25, n = 1143, Q(df = 4) = 17, I2 = 76%] (Figure 2). Lastly, the study on veterans with diabetes by Smalls et al also did not show a significant association between LDL and FIS,58 but it was not added to the meta-analysis due to lack of primary data for OR or Hedges g.

Meta-analysis of adult studies investigating food insecurity and low-density lipoprotein (LDL) measurement. Hedges' g, standardized mean differences with a small size correction, were calculated from the primary data of the 5 studies. Meta-analysis resulted in a nonsignificant effect: gLDL = -0.02 [95% CI, -0.28, 0.25, n = 1,143, Q(df = 4) = 17, I2 = 76%].
HDL
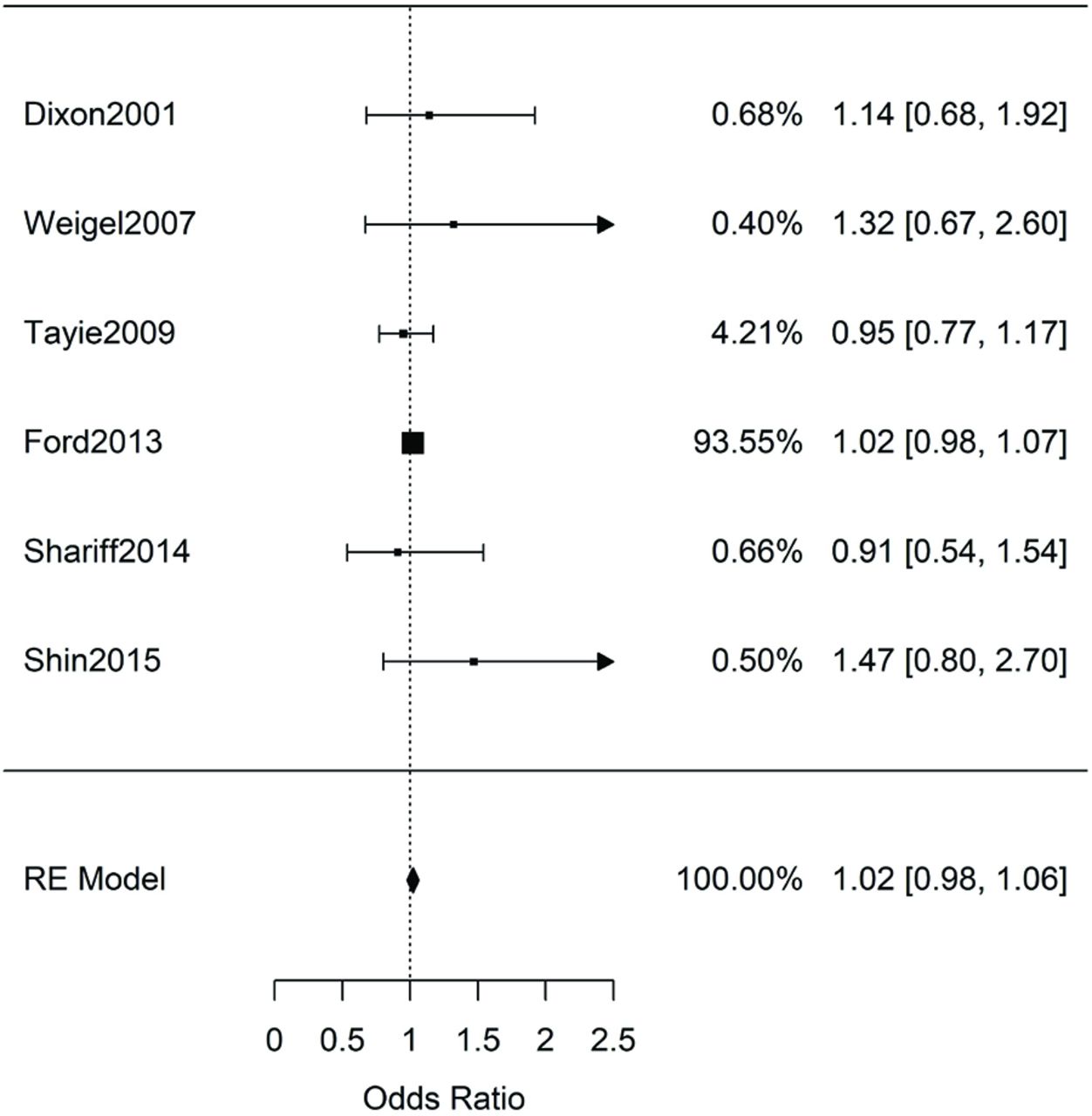
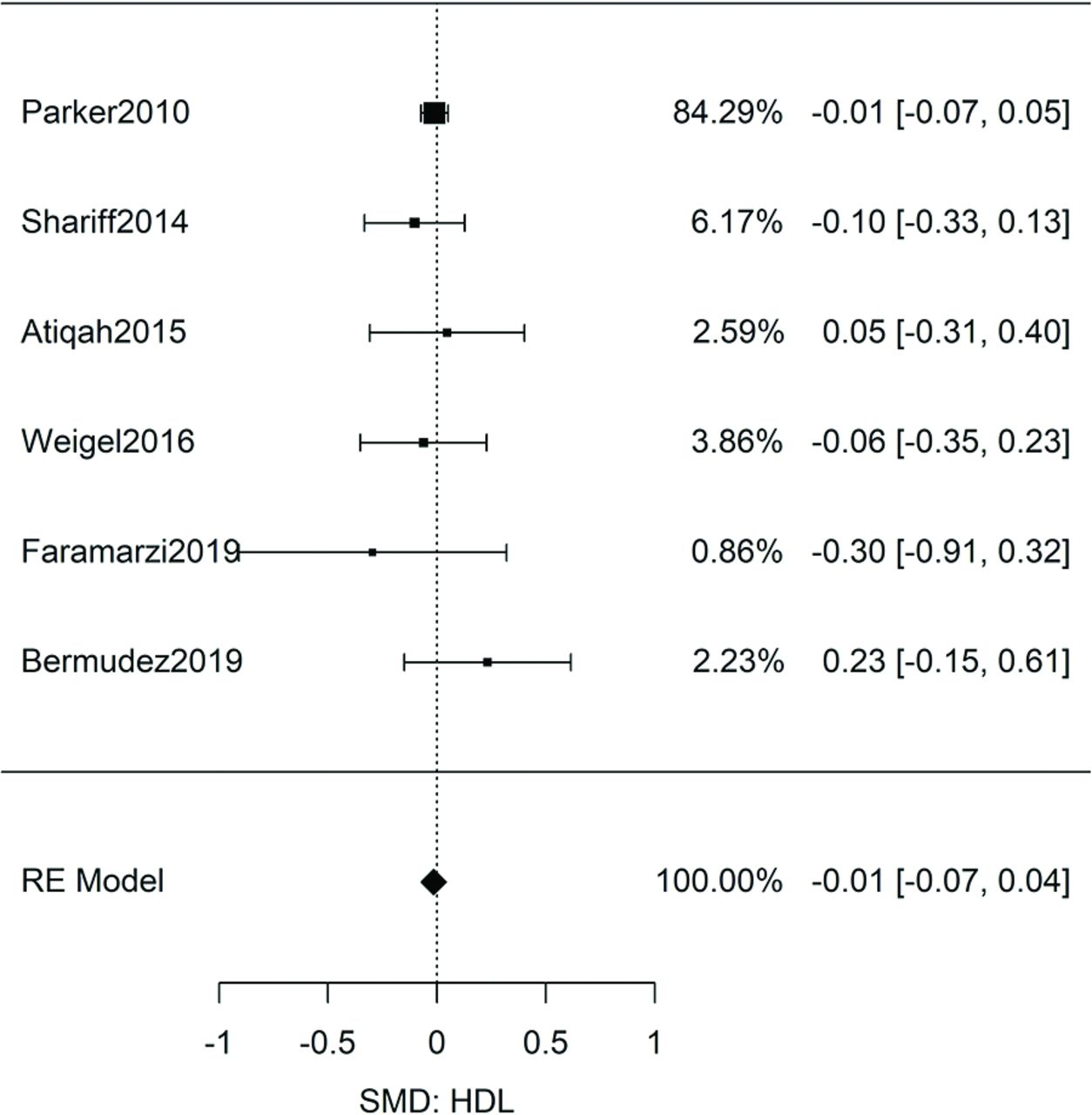
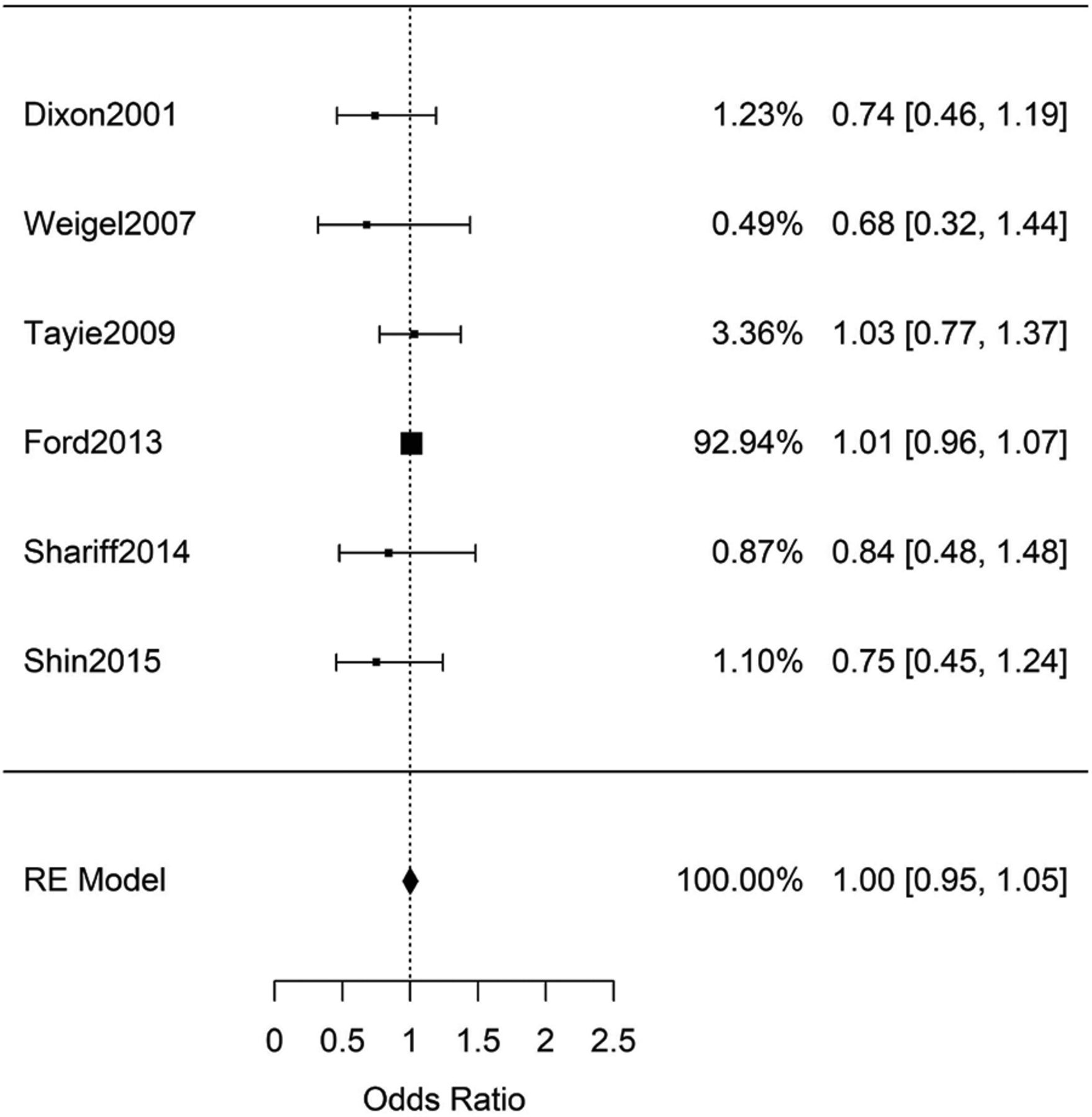
Synthesis by meta-analysis of the 6 nonoverlapping studies (n = 28,557) (Online Appendix Table 3) exploring FIS and low levels of HDL resulted in a nonsignificant result: ORHDL = 1.02 [95% CI, 0.98, 1.06, n = 28,557, Q(df = 5) = 2.7, I2 = 0%] (Figure 3). Not only was the synthesized OR close to 1, but the heterogeneity (I2 = 0) was lower than that expected from random chance. Synthesis of the 6 HDL studies (Online Appendix Table 4) with standardized mean data resulted in a nonsignificant difference in HDL levels between food-secure and food-insecure adults: gHDL = −0.01 [95% CI, -0.07, 0.04, n = 7,096, Q(df = 5) = 3.20, I2 = 0%] (Figure 4).
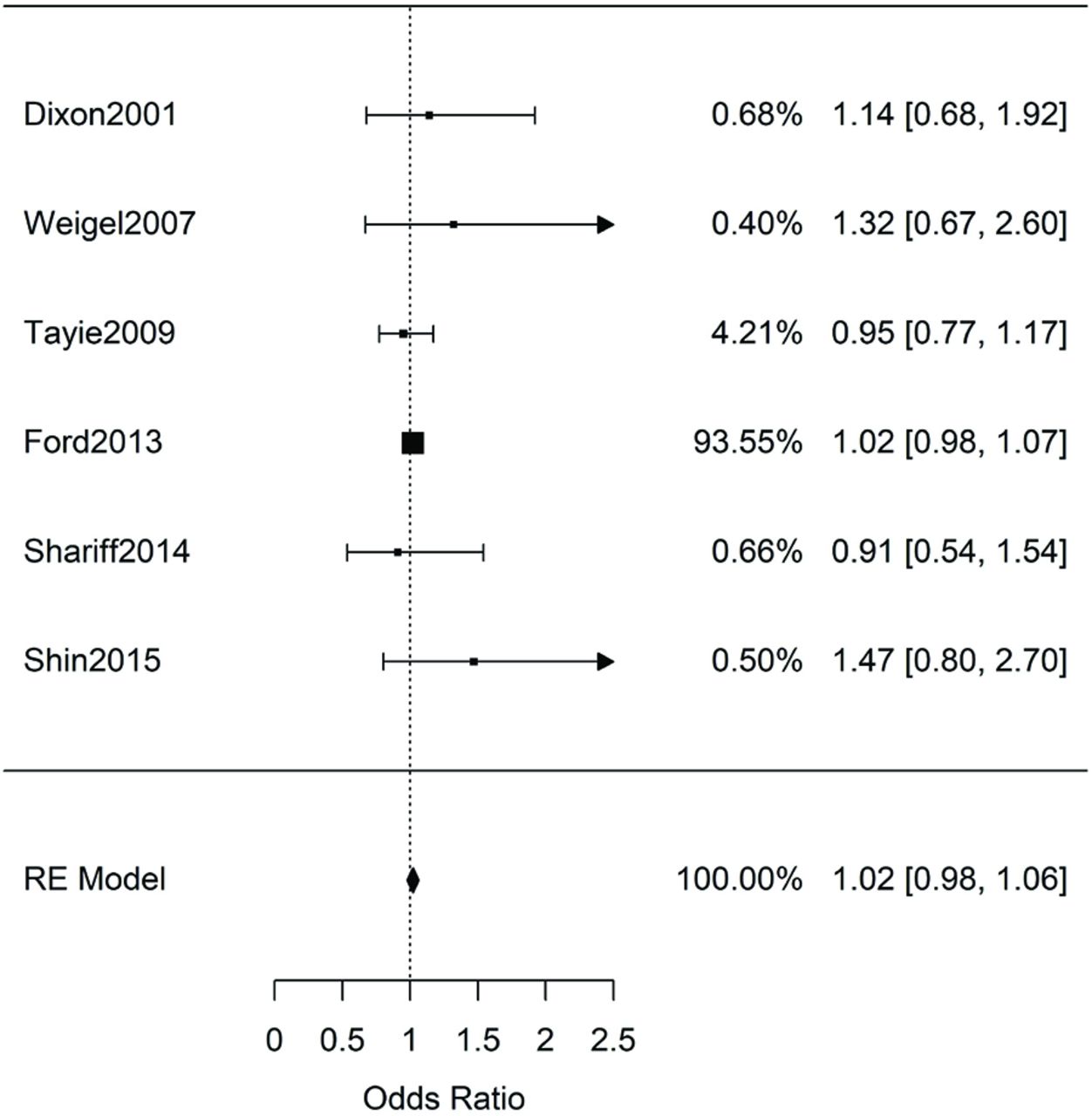
Meta-analysis of adult studies investigating increased odds of low high-density lipoprotein (HDL) for food-insecure patients. Synthesis of the 6 studies resulted in a nonsignificant combined odds ratio of ORHDL = 1.02 [95% CI, 0.98, 1.06, n = 28,557, Q(df = 5) = 2.7, I2 = 0%].

Meta-analysis of adult studies investigating food insecurity and high-density lipoprotein (HDL) levels. Hedges' g, standardized mean differences with a small size correction, were calculated from the primary data of the 6 studies. Meta-analysis resulted in a nonsignificant effect: gHDL = -0.01 [95% CI, -0.07, 0.04, n = 7,096, Q(df = 5) = 3.20, I2 = 0%].
Total Cholesterol
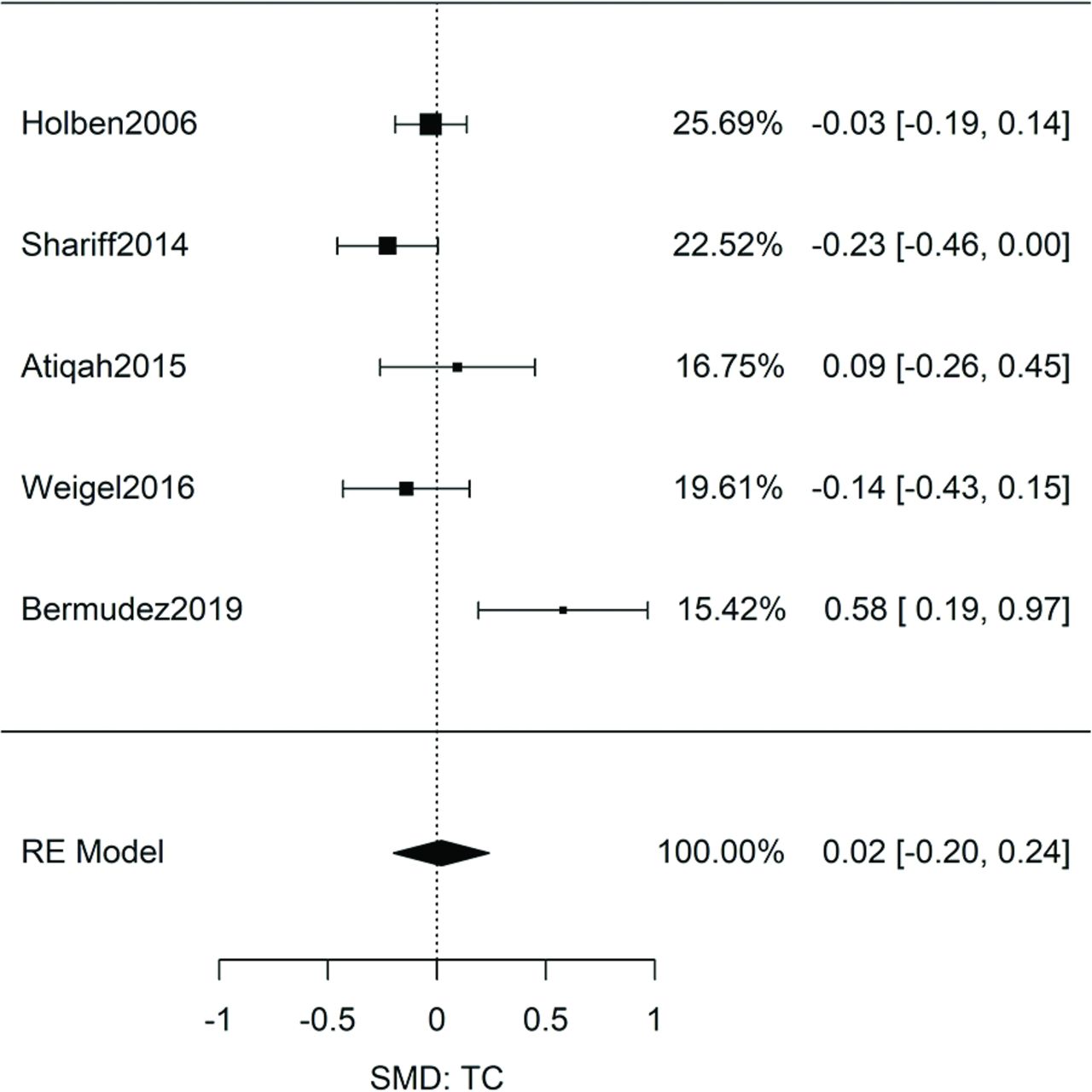
Meta-analysis of 6 studies (n = 28,225) (Online Appendix Table 5) showed similar odds for elevated cholesterol between food-insecure and food-secure patients: ORTC = 1.00 [95% CI, 0.95, 1.05, n = 28,225, Q(df = 5) = 4.3, I2 = 0%]. The results (Figure 5) were homogeneous as evidenced by the calculated I2. The study excluded from this meta-analysis, due to overlapping data, also reported no significant association.61 Analysis of SMDs of 5 studies (Online Appendix Table 6) also showed no significant association in the TC levels between food-insecure and food-secure patients: gTC = 0.02 [95% CI, -0.20, 0.24, n = 1,614, Q(df = 4) = 13, I2 = 70%] (Figure 6).
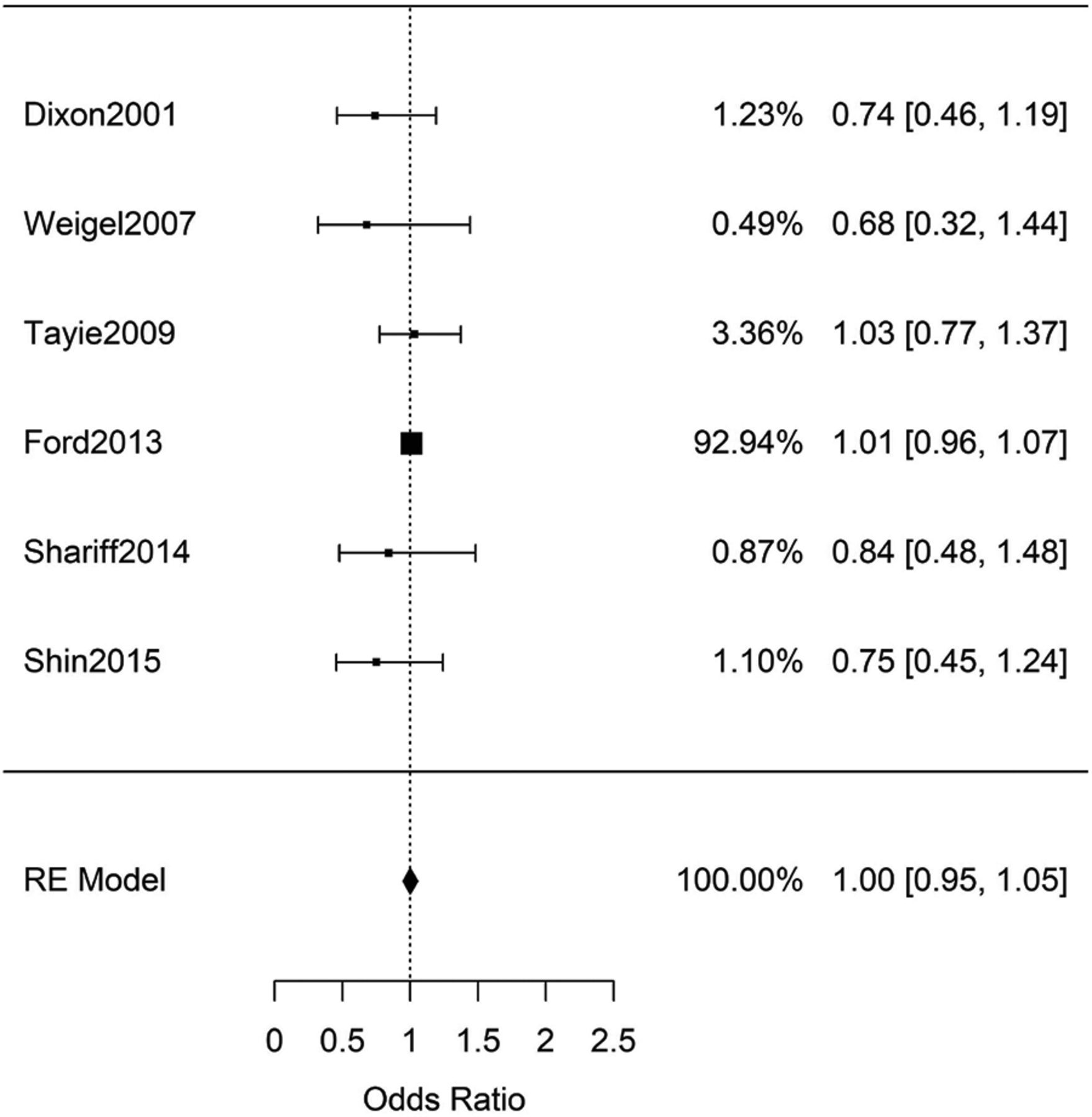
Meta-analysis of adult studies investigating increased odds of elevated total cholesterol for food-insecure patients. Synthesis of the 6 studies resulted in a nonsignificant combined odds ratio of ORTC = 1.00 [95% CI, 0.95, 1.05, n = 28,225, Q(df = 5) = 4.3, I2 = 0%].

Meta-analysis of adult studies investigating food insecurity and total cholesterol levels. Hedges' g, standardized mean differences with a small size correction, were calculated from the primary data of the 5 studies. Meta-analysis resulted in a nonsignificant effect: gTC = 0.02 [95% CI, -0.20, 0.24, n = 1,614, Q(df = 4) = 13, I2 = 70%].
Triglycerides
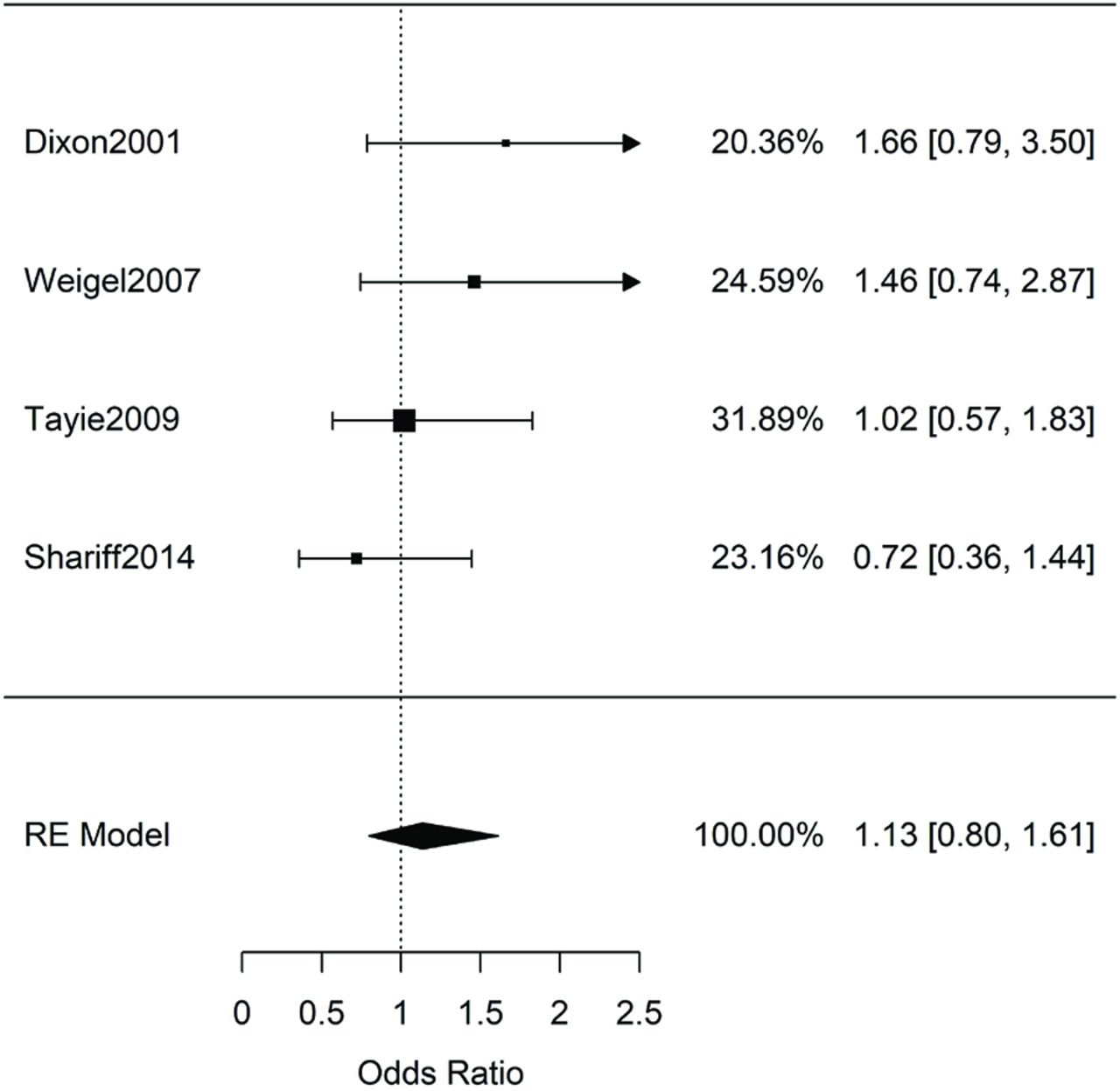
Meta-analysis of 5 studies (Online Appendix Table 7) with adjusted ORs for elevated TG in food-insecure versus food-secure patients yielded ORTG = 1.13 [95% CI, 0.80, 1.61, n = 16,107, Q(df = 3) = 3.29, I2= 10%] (Figure 7). Similarly, analysis of SMDs for 5 studies (Online Appendix Table 8) showed no significant difference between food-secure and food-insecure patients: gTG = 0.02 [95% CI, -0.22, 0.27, n = 958, Q(df = 4) = 10.2, I2 = 61%] (Figure 8).

Meta-analysis of adult studies investigating increased odds of elevated triglycerides for food-insecure patients. Synthesis of the 4 studies resulted in a nonsignificant combined odds ratio of ORTG = 1.13 [95% CI, 0.80, 1.61, n = 16,107, Q(df = 3) = 3.29, I2= 10%].
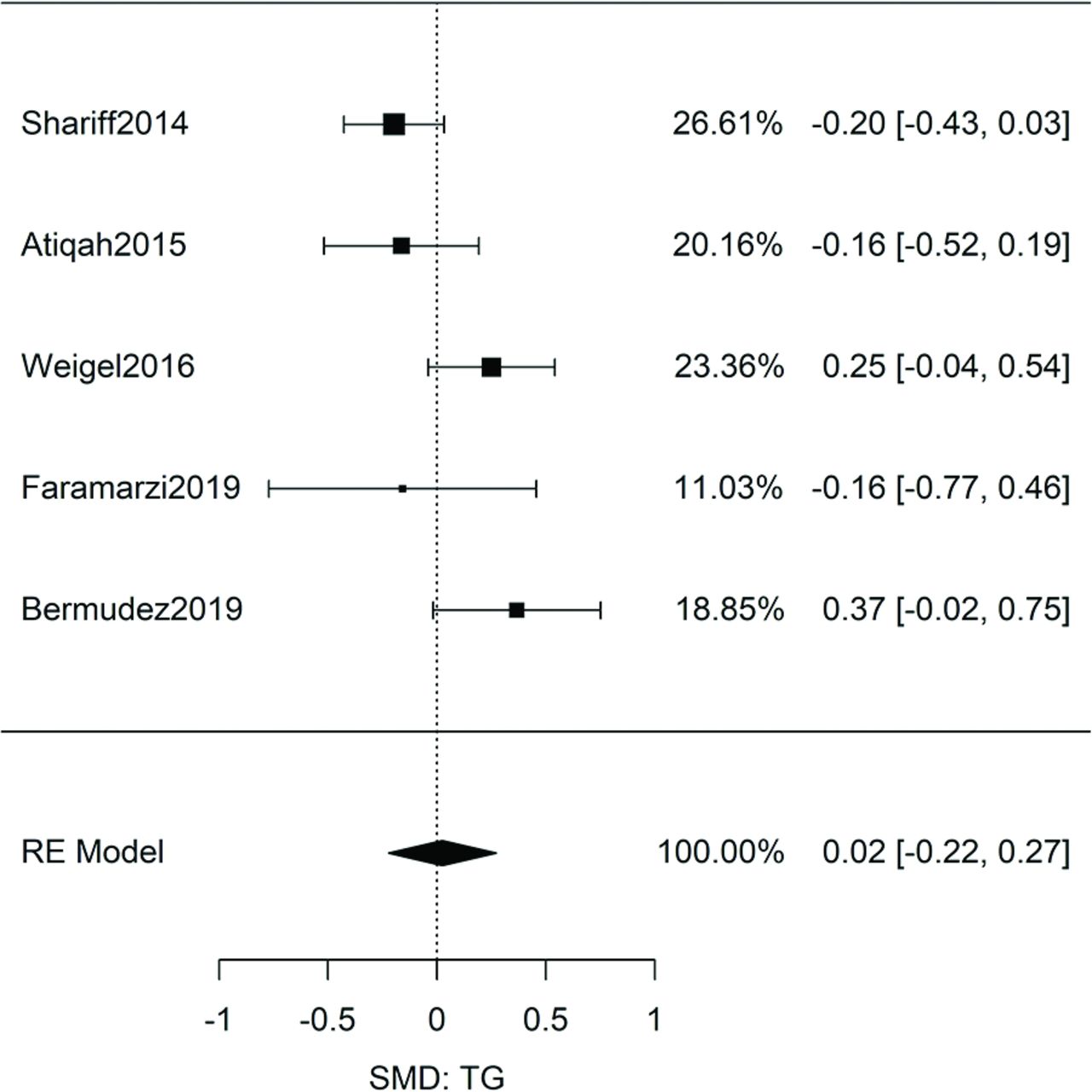
Meta-analysis of adult studies investigating food insecurity and triglycerides levels. Hedges' g, standardized mean differences with a small size correction, were calculated from the primary data of the 5 studies. Meta-analysis resulted in a nonsignificant effect: gTG = 0.02 [95% CI, -0.22, 0.27, n = 958, Q(df = 4) = 10.2, I2 = 61%].
Self-Reports of Dyslipidemia Diagnosis
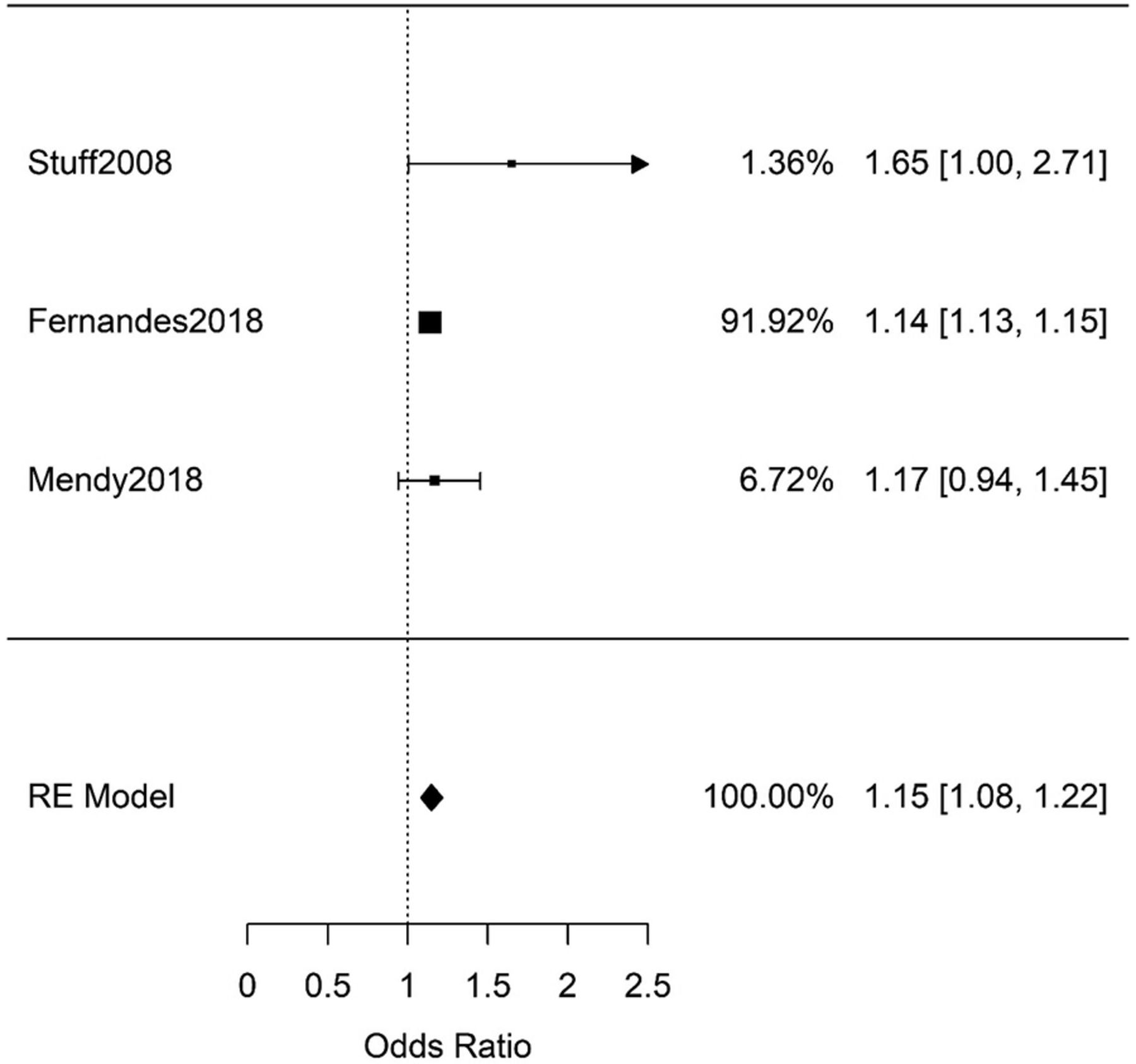
As previous meta-analyses studies have shown conflicting results between lab measurements and self-report of chronic conditions,78 we a priori decided to separate these studies. We identified 5 studies (n = 12,888) that used self-reports of previous/current dyslipidemia diagnosis (Online Appendix Table 11). There was sufficient data to synthesize 3 of the studies; the result showed a significant association: ORself-report = 1.15 [95% CI, 1.08, 1.22, n = 9,212, Q(df = 2)=2.2, I2 = 10%] (see Online Appendix Figure 2).
Risk of Bias within Studies and across Studies
Analysis with the AXIS tool did not identify any study warranted for exclusion. As for publication bias, none of the funnel plot asymmetry tests yielded positive results. However, it should be emphasized that for such a small number of studies the statistical power for these tests is very small.79,80
Subgroup Analyses
Diabetic Patients
One US study specific to the diabetes population reports a significant association between FIS and elevated LDL.53 Another US study, specific to California and Hispanics, does not report an association between FIS and elevated LDL in their diabetic population.52 These were the only 2 studies reporting adjusted ORs for the diabetic population and were considered too few for meta-analysis. We also calculated the association specific to this group by extracting primary data from 2 other US studies (at Hartford and Illinois)56,57; the analysis did not yield a significant association between FIS and elevated LDL.
Female Patients
There were mixed results on whether FIS was associated with higher odds of elevated LDL measurements in women.49,50 The study on US women by Tayie and Zizza49 showed significantly higher adjusted odds of elevated LDL in food-insecure compared with food-secure patients; combining their results from different levels of FIS yielded AOR = 1.51 [95% CI, 1.02, 2.24, n = 2,977] (Online Appendix Table 1). In contrast, the study by Shariff et al on Malaysian women did not show a significant result: AOR = 0.75 [95% CI, 0.42, 1.31, n = 625].50
Three comparable studies (Online Appendix Table 2) were available for meta-analysis after calculating the SMD in LDL levels between the food-secure and food-insecure women50,54,55; synthesis of the results yielded significantly lower LDL levels in food-insecure patients compared with food-secure patients: gLDL_Women = -0.24 [95% CI, -0.45, -0.02, n = 668, Q(df = 2) = 3.1, I2 = 55%]. As this corresponds to unadjusted data, it is difficult to compare with the results from Tayie and Zizza and Shariff et al.49,50
Discussion
In this systematic review and meta-analysis, we found no association between FIS and dyslipidemia. Synthesis of the available literature showed that food-insecure adults did not have significantly elevated nor decreased odds of qualifying for a dyslipidemia diagnosis, whether by elevated LDL, TC, or TG, or a decreased HDL. There are several possible explanations for the nonassociation observed in the synthesis of the current data.
First, counterbalancing, opposing effects may be operating across the general population due to 2 major subsets of patients: 1 ingesting fewer calories11⇓–13 and another consuming a poor-quality diet with normal or increased calories.14,15 Given its complexity, FIS may translate into differences in diet and calorie intake, effects that may vary significantly across different cultures, locations, and individuals. As these studies did not measure the calories or nutritional quality of the food ingested, it is currently not possible to assess the impact of these factors. Furthermore, there were very few studies outside of the USA, and few studies presenting data on socioeconomic, racial, or ethnic subgroups. Therefore, it remains possible that associations between FIS and lipid profiles might be detected in future studies focusing on specific subpopulations of patients.
Second, it is possible that the strengths (ie, effect sizes) of the intermediate associations (ie, FIS to diet quality, and diet quality to dyslipidemia) are small and do not lead to an appreciable effect size overall. The upper limits of the 95th confidence intervals from the meta-analyses provide convincing evidence that the overall effect size is most likely small. For example, the unadjusted effect size for TC was (g = 0.02 [95% CI, -0.20, 0.24]); and an effect size of 0.24 is small, especially when compared with other FIS associations.31,81,82 Similarly, upper limits from the covariate-adjusted ORs (ie, ORTC = 1.00 [95% CI, 0.95, 1.05]) suggest weak effects as well.
Finally, it is important to acknowledge that the effect of FIS on serum lipids may be time dependent and thus may not have been captured in the currently available cross-sectional studies because the patients studied had not experienced FIS for a long enough duration to produce measurable changes in serum lipid levels. Furthermore, our review identified few studies that focused (or performed subpopulation analysis) on elderly populations, which may have demonstrated a larger response. Admittedly, our results may reflect a complex interplay of all of the processes described above.
Unlike dyslipidemia studies that used lab measurements, self-reports of previous diagnosis were significantly associated with FIS. This finding is similar to what has been previously reported by Beltrán et al for FIS and self-reported diabetes and hypertension.78,83 It is currently unclear why food-insecure patients are more likely to report such chronic diagnoses, although 1 possibility is a complex interaction between FIS, anxiety/depression,31 and the odds of self-reporting poor health.84
With respect to its clinical implications, our data do not indicate an association between FIS and dyslipidemia and thus do not support routine lipid screening of food-insecure individuals. However, as more FIS-dyslipidemia studies focusing on different countries, races, ethnicities, or socioeconomic groups emerge, such assessments may subsequently be determined to be warranted.
This study has several important limitations. First, the combined cross-sectional studies do not yield information on either causality or temporal relationships between FIS and lipid measurements. Second, our subgroup analyses were greatly limited by the availability of demographic-specific data on FIS and dyslipidemia. Not only were the studies limited to a few countries, there was very little data to explore by meta-analysis how the association occurs in children, across genders, across races/ethnicities, and for seniors. Third, the small number of studies do not allow satisfactory exploration of publication bias. Although no funnel asymmetry test was significant, it is important to note that the statistical power of these tests is small for the number of studies reviewed.
Conclusions
Currently, the available published data do not support an association between FIS and dyslipidemia. This literature, however, would be further strengthened by prospective and more higher-quality retrospective cohort studies; studies targeting important populations such as children, women, minorities, seniors, and patients with diabetes; investigations of populations beyond those of the USA, Malaysia, and Iran; and studies incorporating covariates such as calorie intake or diet quality as well as BMI.
Acknowledgments
The authors thank Whitney Orji for useful discussions of the manuscript.
APPENDIX
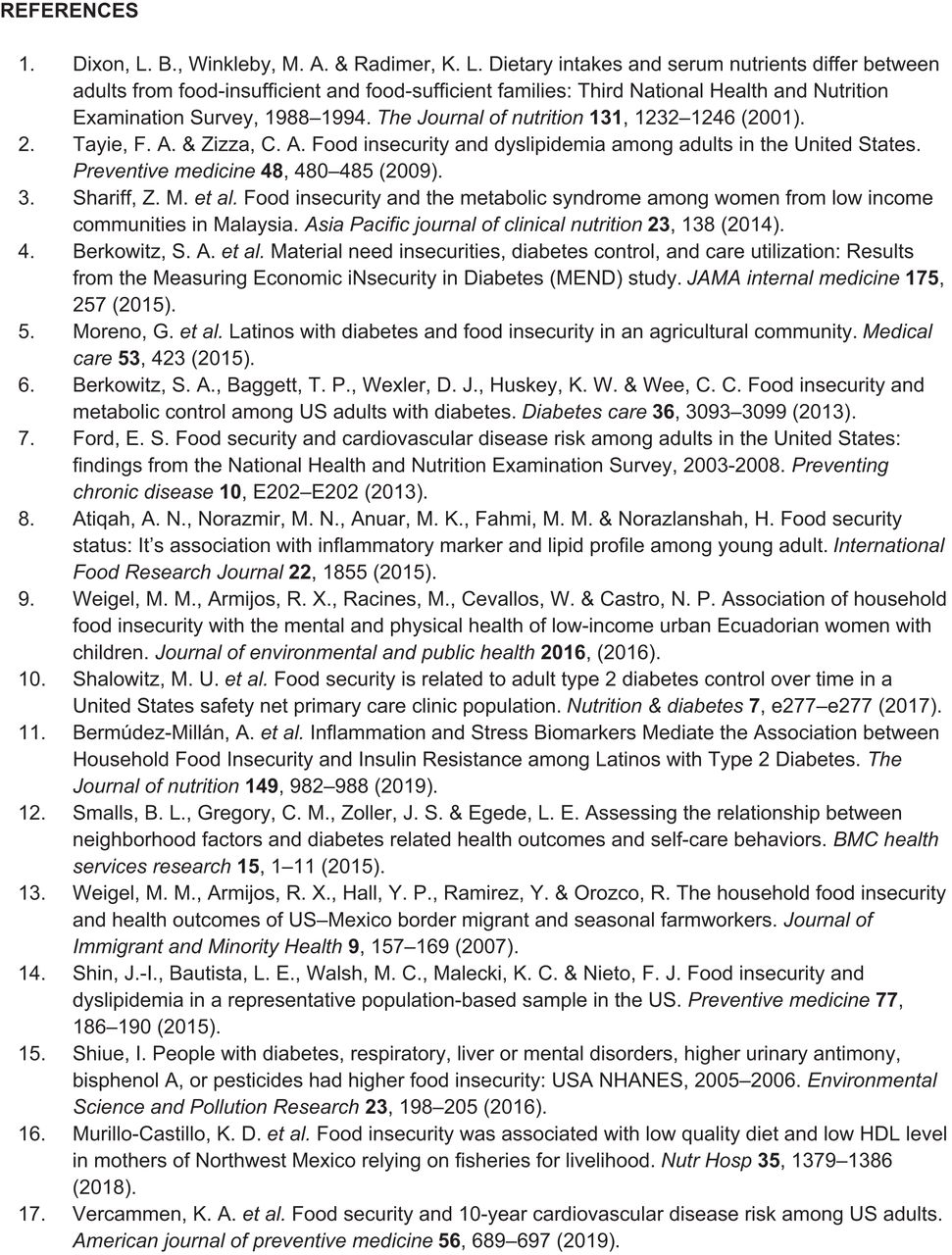
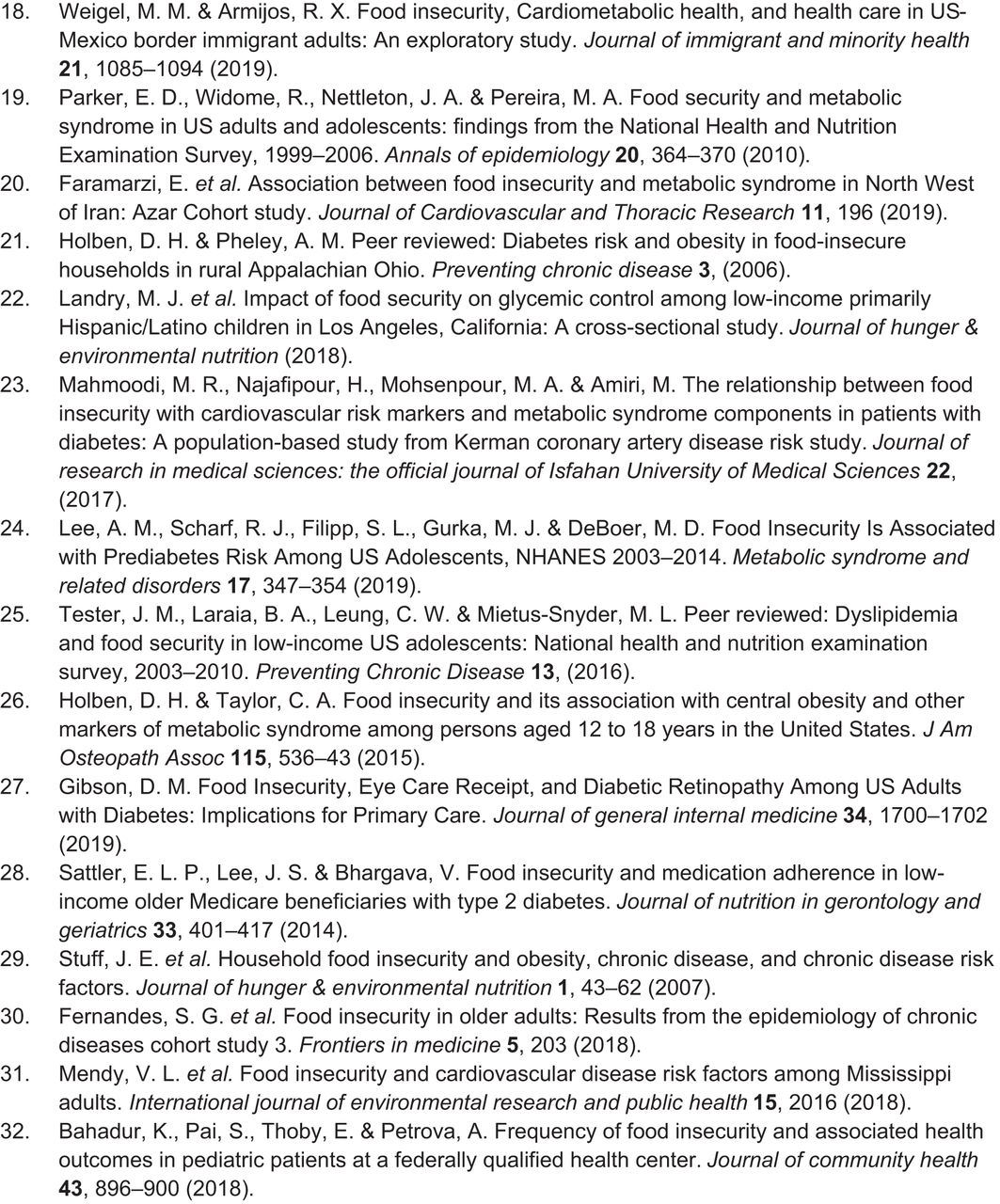
Note: References cited below are those of the 32 studies that were the basis of this systematic review and meta-analysis. Please note that the numbering of these studies in the references for the appendix does not correspond to their numbering in the references for the main manuscript.
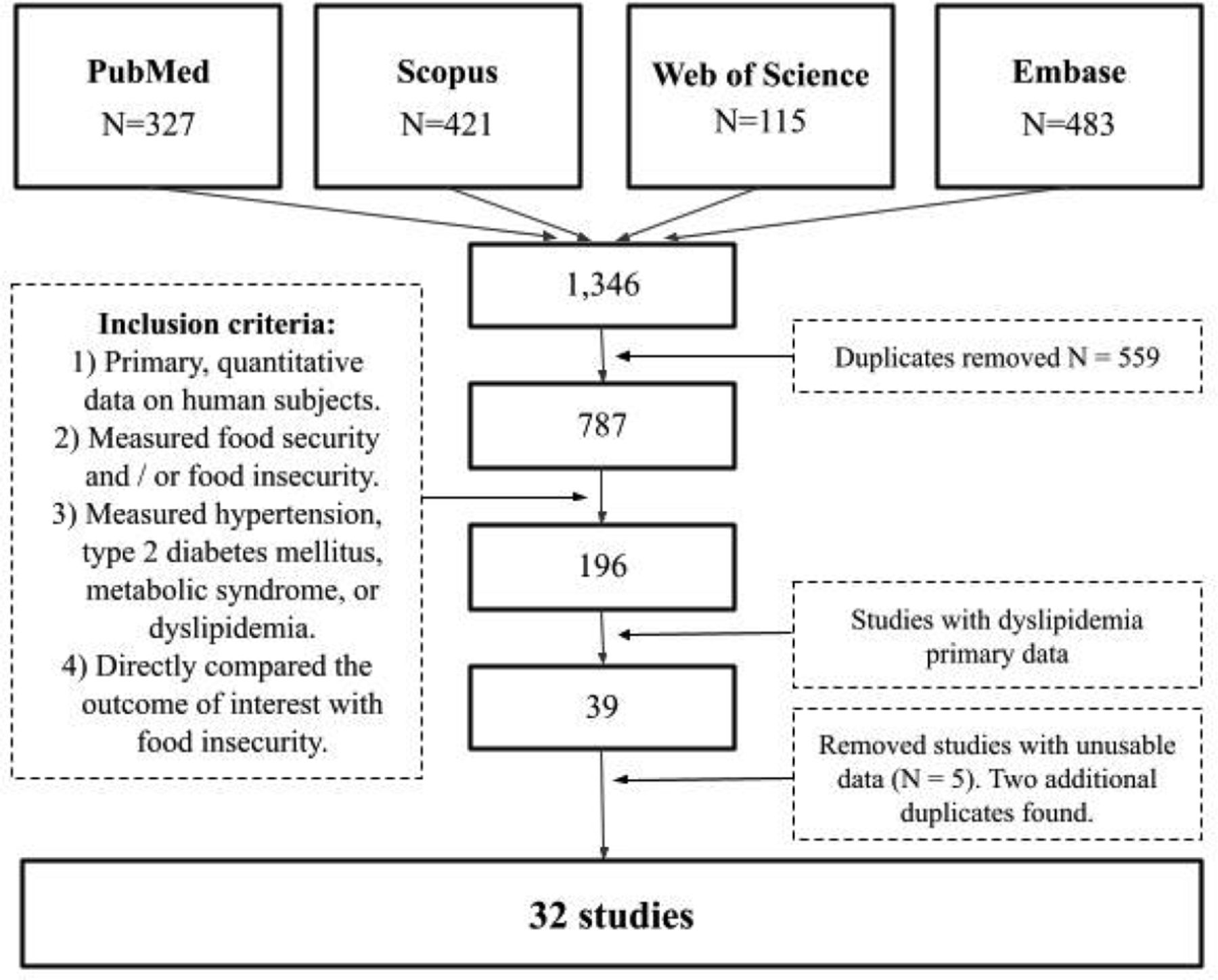
Flow chart displaying the study selection process.

Meta-analysis of adult studies (n = 9,212) investigating increased odds of self-reported dyslipidemia for food insecure patients. Synthesis of the three studies resulted in a significant combined odds ratio of 1.15 [95%CI: 1.08–1.22, n = 9212, Q (df = 2) = 2.2, I2 = 10%].
Adult studies (n = 22,746) with sufficient data to retrieve or calculate the odds ratio for food insecurity and elevated LDL
Adult studies (n = 1,143) with sufficient data to retrieve or calculate the standardized mean difference (Hedges'g) in LDL levels between food secure and food insecure patients
Adult studies (n = 28,557) with sufficient data to retrieve or calculate the odds ratio for food insecurity and decreased HDL
Adult studies (n = 7,096) with sufficient data to retrieve or calculate the standardized mean difference (Hedges'g) in HDL levels between food secure and food insecure patients
Adult studies (n = 28,225) with sufficient data to retrieve or calculate the odds ratio for food insecurity and elevated total cholesterol
Adult studies (n = 1,614) with sufficient data to retrieve or calculate the standardized mean difference (Hedges'g) in total cholesterol levels between food secure and food insecure patients
Adult studies (n = 16,107) with sufficient data to retrieve or calculate the odds ratio for food insecurity and elevated triglycerides
Adult studies (n = 958) with sufficient data to retrieve or calculate the standardized mean difference (Hedges'g) in triglyceride levels between food secure and food insecure patients
Pediatric studies with sufficient data to retrieve or calculate the standardized mean difference (Hedges'g) in lipid levels between food secure and food insecure patients
Pediatric studies with sufficient data to retrieve or calculate the odds ratio for dyslipidemias between food secure and food insecure patients. There were not sufficient data to synthesize for a specific dyslipidemia (i.e. high LDL, or low HDL)
Adult studies with self-reported or chart review methodology

Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: The authors have no conflicting or competing interests to declare.
To see this article online, please go to: http://jabfm.org/content/35/4/656.full.
- Received for publication October 17, 2021.
- Revision received December 29, 2021.
- Accepted for publication January 5, 2022.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}