
Abstract
Introduction: Our university hospital-based primary care practices transitioned a budding interest in telehealth to a largely telehealth-based approach in the face of the COVID-19 pandemic.
Initial work: Implementation of telehealth began in 2017. Health system barriers, provider and patient reluctance, and inadequate reimbursement prevented widespread adoption at the time. COVID-19 served as the catalyst to accelerate telehealth efforts.
Implementation: COVID-19 resulted in the need for patient care with “social distancing.” In addition, due to the pandemic, the Centers for Medicare and Medicaid Services and other insurers began expanded reimbursement for telehealth. More than 2000 providers received virtual health training in less than 2 weeks. In March 2020, we provided 2376 virtual visits, and in April 5293, which was more than 75 times the number provided in February; 73% of all visits in April were virtual (up from 0.5% in October 2019). As COVID-19 cases receded in May, June, and July, patient demand for virtual visits decreased, but 28% of visits in July were still virtual.
Lessons learned: Several key lessons are important for future efforts regarding clinical implementation: (1) prepare for innovation, (2) cultivate an innovation mindset, (3) standardize (but not too much), (4) technological innovation is necessary but not sufficient, and (5) communicate widely and often.
Introduction
The emergence of COVID-19 combined with subsequent public health measures to reduce social contact have created an increasingly vital role of telehealth.1⇓–3 Telehealth is generally understood to include any visit between patient and provider or provider and provider that is not in-person. This can include video visits, phone visits, and sometimes electronic asynchronous communication such as an e-consult or messaging within an electronic medical record (EMR) or patient portal.1
Although many institutions and their associated practices had baseline telehealth capabilities before the pandemic, COVID-19 necessitated a rapid increase in telehealth capacity and use, specifically to triage and treat patients suspected or infected with COVID-19, to care for patients after leaving the hospital setting, and to continue addressing routine non-COVID-19 care in the outpatient setting.1,4⇓–6 As “social distancing” was presented as the main way to limit spread of the virus and decrease the peak of a potential surge in cases, patients also began to show increasing interest in telehealth services.7 State and local orders for stay-at-home mandates and restrictions on unnecessary in-person medical care in late March accelerated this trend; these orders were gradually relaxed or rescinded from late April through May 2020. Before the pandemic, use was generally low for routine care due to several obstacles. Provider-based obstacles included clinician acceptance of the modality, payment for services, Health Insurance Portability and Accountability Act (HIPAA) compliance with various platforms, available technology, and health system structure,5,8 while patient-level factors included consent processes, ability to use and access the telehealth online portal, and compliance with legal, ethical, and logistic needs of the individual patient population such as parental consent for pediatric patients.2 However, with a rapidly increasing demand for telehealth services, many institutions were able to overcome these obstacles in a matter of days to weeks,2,8 whereas others are still struggling with getting telehealth running and reimbursed effectively.9
This article will address how the University of Colorado Department of Family Medicine (DFM) was able to harness an already increasing interest in telehealth to rapidly and efficiently transition to largely telehealth-based patient care. We share factors we believed were important in successful rapid transition and sustainment of telehealth as well as practical guidance in the form of lessons learned in provision of telehealth in primary care.
The Setting
The University of Colorado Health System is a network of hospitals, clinics, and health care providers throughout Colorado, southern Wyoming, and western Nebraska. It is the largest academic health center in the Rocky Mountain region, and the focal location is at the Anschutz Medical Campus, home to the University of Colorado health professional schools, research laboratories, and the UCHealth University of Colorado hospital. The University of Colorado DFM is associated with UCHealth and employs 145 regular faculty, 75 affiliate faculty, and 65 support staff, as well as 600+ volunteer faculty. There are 5 UCHealth-owned family medicine clinics located in the metro Denver area. Two clinics integrate family medicine and internal medicine faculty, while 1 is a residency clinic. Table 1 describes the clinics in summary.
University of Colorado Department of Family Medicine Clinics
Initial Work on Telehealth Pre-COVID-19
Implementation of telehealth in the UCHealth system began with the introduction of virtual visits in July 2017; however, virtual visits in family medicine would not happen for a couple of years. A key element needed for introduction of telehealth was the availability of a platform to run the telehealth services. The Vidyo platform (Vidyo, Inc., Hackensack, NJ) was selected by the hospital administration in part because it was able to integrate with the electronic record Epic (Epic Systems Corporation, Verona, WI). Therefore, from a practical perspective, there needed to be leadership buy-in to the concept of telehealth at various levels (system, practice, clinician, and staff), resources (ie, funds within the system) to purchase and operate the telehealth system, and the availability of an actual telehealth system to be either purchased or internally developed.
Other important aspects to the setup of telehealth are also important. One key aspect for virtual visits to function was built on foundational elements related to scheduling. UCHealth implemented system-level, patient-facing support services to improve patient satisfaction, access, and delivery of care starting during the summer of 2015. This centralized service expansion included appointment scheduling for in-person visits, nursing triage, portal-based self-service scheduling, and referral authorization, all housed within a centralized patient contact center. At the end of 2019, the contact center was fielding 1.7 million calls and processing 1 million referrals annually.10 Planning for central support of virtual visits began in 2017, but phone center and portal-based scheduling of virtual visits occurred in March and April of 2020, with COVID-19 serving as the catalyst to accelerate efforts.
Coordinated implementation within the DFM began in 2019 with a limited number of medical and behavioral health providers at 1 clinic conducting video visits starting in January. All clinics engaged with the UCHealth virtual health project team to train local staff to be superusers of the Vidyo platform and to procure computers (laptops, workstations on wheels) and peripheral devices (eg, webcams, speakers) that would be used for in-clinic virtual visits.
In July 2019, the family medicine department clinical leadership made expanding virtual visits a departmental priority, setting 3 primary goals: (1) virtual visits will comprise 5% of DFM clinic visits by July 2020, (2) clinic activities would be organized to intentionally learn from each other, and (3) standardized virtual visit processes would be used in all clinics when possible. A virtual visit leader was selected from a competitive application process and formed a working group of local clinic virtual visit champions supported by a department administrator. Starting in October 2019, the virtual visit lead and local champions were provided with protected administrative time to devote to their local and cross-clinic work.
The virtual visit lead and administrator met with their own individual clinics to set local interim goals around clinician and staff engagement, technical support, and patient communication. The virtual visit champions also met as a group each month to share best practices, troubleshoot barriers, and prioritize requests of external leaders and workgroups. Issues discussed included billing and compliance, technology bug fixes, UCHealth website support, scheduling, and staffing workflows. In December 2019, 1 of the virtual visit champions piloted the UCHealth’s first remote, fully virtual primary care session—a feat that seemed amazingly fast at the time. With growing experience, the champions developed an onboarding and training packet in January 2020 that could equip clinicians with the information to begin conduct and bill for virtual visits in under 15 minutes. The training materials were largely in the form of screenshots and documents showing providers how to access telehealth through Epic; training was delivered via live one-on-one and small group presentations. Medical assistants at each practice received additional training to support clinicians in real time with any technology issues.
The focused efforts translated to a growing tally of virtual visits performed in the family medicine clinics each month, and by the end of February, more than half (54%) of the medical providers were conducting virtual visits (see Figure 1). Although the clinics had yet to engage residents or behavioral health providers in virtual visits or leverage centralized call center support, the practices entered March in the enviable position of being “relatively ready” for the pandemic-driven need to move to almost completely virtual.

Cumulative proportion of providers completing virtual visits over time. Abbreviations: BH, behavioral health; GME, family medicine residents in graduate medical education programs.
Implementation during COVID-19 That Facilitated Rapid Transition
The biggest contributors to the expansion of virtual visits were the COVID-19 pandemic, providers and staff contracting COVID-19 in the workplace, and the resulting needs for patient care in the face of “social distancing” to reduce the spread of the coronavirus. Equally important in relation to this need was the Centers for Medicare and Medicaid Services decision to reimburse telehealth more fully and for more people. Medicaid initially agreed that phone visits were reimbursed similarly to video visits and in-person visits. Medicare would later allow for this parity as well. In addition, HIPAA compliance rules for video visits were temporarily relaxed to accommodate more rapid transition to virtual care. This has particularly impacted the platforms available for virtual visits and questions about confidentiality of phone visits as well as the use of privacy-compliant dialers for staff and providers. These conditions made for a special circumstance to make virtual visits important.
The virtual visit champions were asked to rapidly develop strategies to transition clinics to telehealth, which happened between March 1 and 20, 2020. The first step was to understand the needs of the clinics, providers, and staff. All providers and staff in all primary care clinics received a readiness survey between March 9 and 17, 2020. The 356 survey respondents detailed a striking risk to staff and providers to both their personal health and virtual work success. Based on the responses, 23% of respondents were determined to be at high risk of COVID-19 health complications; 32% of staff (43/133) did not have computers able to access the EMR remotely, and 28% (37/133) reported being unable to provide any virtual patient care outside of the clinic.
Based on those survey results, the DFM provided early advocacy for health system staff members to be paid for remote work. Medical directors and clinical managers met in dyads on a daily basis to coordinate implementation of virtual care and remote work. The DFM provided School of Medicine computing equipment to staff, learners (behavioral health staff, residents), and providers. Department-level information technology staff was also available to support these groups as they used the hardware remotely.
New system-wide communications and operations structures were quickly developed or expanded. Extensive system-wide support, training, and technical assistance was available for all care team members to prepare for remote work. This support included help installing software on phones, technology to support secure calling from personal phones, tip sheets to help patients connect with video visits, and remote faxing workflows.
Streamlined communication and information dissemination was rapidly organized. Ambulatory leaders increased the frequency of operations meetings from monthly to daily to provide updates on information regarding COVID-19 disease spread, changes in recommendations about personal protective equipment, staffing shortages, changes in policies, and other emergency issues. This communication was coupled with daily summary e-mails to all leadership teams in family medicine and general internal medicine.
A virtual command center opened to provide high-level leadership and disseminate policies and procedures around virtual and remote work. Resource provisioning was addressed, redeploying staff, equipment, and other support from underused sections of the system to high-demand hospital units, newly established testing sites, and other critical operation activities. The virtual health command center also facilitated training and implementation of the virtual platform and addressed health system policy issues.
In addition to existing efforts to train providers before COVID-19, a rapid escalation and redeployment of training resources resulted in more than 2000 providers system-wide receiving virtual health training in less than 2 weeks. This training included hourly live training sessions that were supported by Project Echo, Epic medical record system trainers, and clinical informaticists. The informatics team members both within and outside of the DFM were deployed to create tip sheets, video resources, and additional electronic tools to support compliance instructions, billing and coding issues, EHR templates, reports, scheduling interfaces, device tools, and workflows.
On March 18, 2020, the hospital required the outpatient clinics to radically reduce in-person visits. Preceding that decision, it became known that the first residents and staff contracted and spread COVID-19 at the residency program clinic. Residents would not return to the clinic until the end of May. Local policies were updated for resident billing, and only later did the American Board of Family Medicine and Accreditation Council for Graduate Medical Education agree to accept these visits to meet continuity visit requirements for residency training completion and professional board certification.
The central call center scheduling of virtual visits began on March 18, 2020. Policies were developed to guide schedulers to safe scheduling practices, and this facilitated a significant increase in virtual visits. By April 9, patients were given the ability to schedule their own virtual visits with primary care through their online health portal. In summary, all of these identified elements contributed to a willing and ready system environment for the rapid adoption and upscaling of primary care telehealth.
The Rapid Increase in Telehealth Visits
We accessed clinic and provider telehealth data using Epic and an analytics visualization service, Power BI (Microsoft Corp., Redmond, WA). The purpose of using Power BI telehealth reporting was to track and trend volume of telehealth visits visually over time. Power BI directly interfaced with Epic to analyze scheduled and completed telehealth visits. Visits could be further visualized by time and date of visit, payer type, online versus phone scheduling, and scheduling trends over time by provider and clinic.
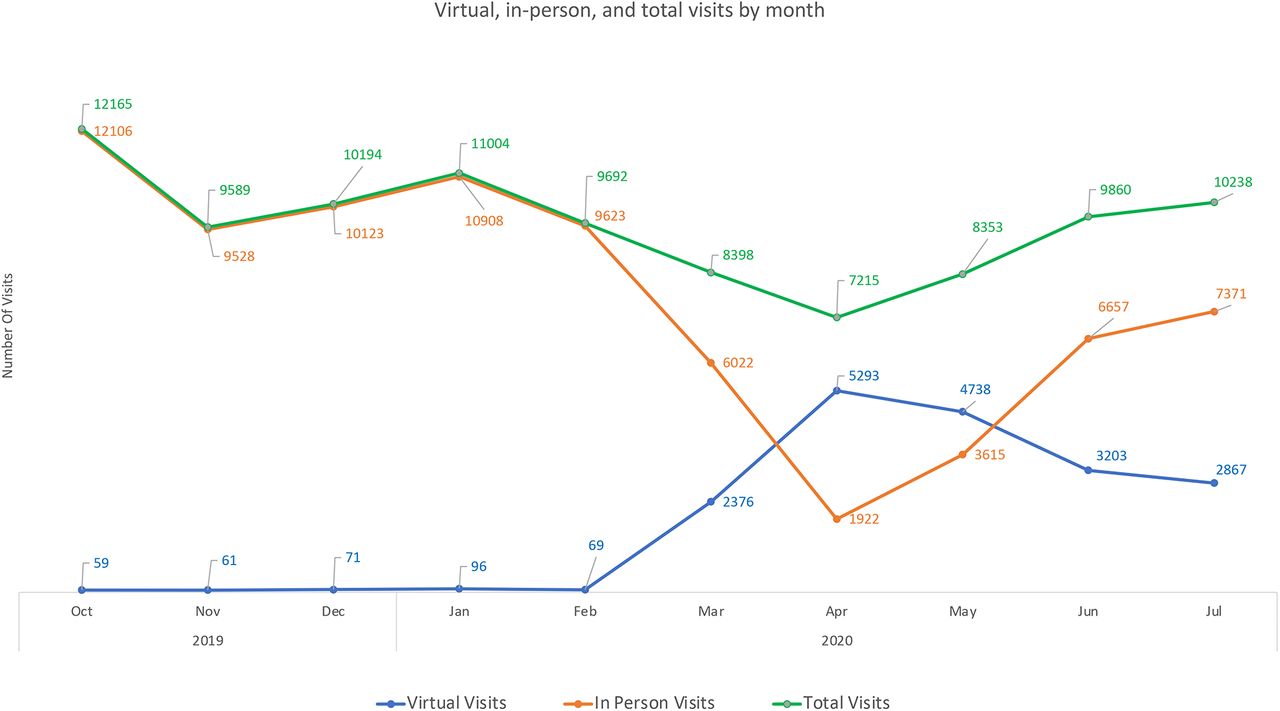
Figure 2 displays in-person and virtual visit totals in the 5 family medicine clinics. In February we had 69 virtual visits, in March we provided 2367, and in April 5292—more than 75 times the February rate. Seventy-three percent of all visits in April were virtual (up from 0.5% in October, 2019). In-person visits began to rebound starting in May, and by July, 28% of visits were virtual. The return to more in-person visits followed a slowdown in COVID-19 cases seen in Colorado, relaxing of the state’s lockdown restrictions, and growing patient demand for in-person visits.

Virtual, in-person, and total visits by month.
Lessons Learned to Apply to Other Telehealth Opportunities in Practice
For others interested in rapid transition of telehealth and other health care innovations in practice, we offer these recommendations.
(1) Prepare for innovation. The preliminary work setting up telehealth greatly facilitated our ability to ramp up telehealth services in a matter of days. On the Rogers Diffusion of Innovations scale,11 consider being an innovator or at least an early adopter. Context (or the circumstances around us) change rapidly, and being prepared means having traveled down the path a bit already. How can your practice be ready for change? What is coming next that is worth investigating now?
(2) Cultivate an innovation mindset. Doing the work to be practically ready for innovation does not necessarily mean that clinical teams are ready or willing to change. University of Colorado family medicine clinics have consciously developed a collective identity as places where innovation happens. People working in these settings are used to continually thinking about, planning, and implementing change.12 Being practiced at trying new things and learning from prior failures made it possible to move quickly. Even if the telehealth system had been in place, but everyone panicked and could not make the mental shift quickly, or argued about change, things would not have worked so well.
(3) Standardize, but not too much. Having a standard technology platform enabled us to rapidly transition to telehealth. However, barriers emerged as virtual care expanded. Patients, providers, and staff experienced technical failures, poor Internet bandwidth, and other end-user challenges. We initially struggled to replicate the full level of team-based care we typically offer, including fully integrated behavioral health and clinical pharmacy services, in-visit documentation support for providers by medical assistants, language translation services, and clinical teaching for residents and a variety of students (medical, nursing, psychology, etc.). We were able to overcome many of these challenges by encouraging practices to innovate locally, including tinkering with the existing technology or experimenting with other platforms. Rapidly communicating, collating, and integrating these variations into our collective approach helped to integrate innovations throughout our system.
(4) Technological innovation is necessary but not sufficient. One important factor in our success was the creation of teams that integrated people with diverse expertise, including technological and administrative expertise as well as direct lived experience of the conditions and context within the individual practices on the ground. Working closely with the centralized scheduling system proved to be critical in making rapid system-wide implementation. Previous practice transformation work created clinic practice champions already “on point” to help within each clinic, facilitating communication and rapid decision making. Although the telehealth platform existed prior to COVID-19, if the implementation structure of the people to do the work had not, change would not have gone as well or as quickly.
(5) Communicate widely and often. Although some structures for communication were in place, the pace and involvement ramped up to meet the need for information. Monthly meetings were converted to daily in some cases. These meetings created a platform to exchange up-to-date information, make sense of the experiences of diverse stakeholders, and provide feedback that facilitated problem solving and rapid iteration. This in turn built trust and thus willingness of staff to make rapid transitions. We prefer to err on the side of overcommunicating in situations of uncertainty necessitating more rapid decision making.
Although our experience occurred within the context of an academic medical center integrated into a large health care delivery system, much of it can be translated to smaller independent settings. Indeed, although large health system-owned practices are known for having more resources, they are also less likely to be nimble.13,14 Large practices within systems often function like tankers, requiring a long time and great distances to turn, without the means to correct course rapidly; small independent practices are more like speed boats, able to change course and maneuver around obstacles quickly. We argue that while some resources are needed to invest in a telehealth system, the proportional costs for independent small practices are much less. In addition, the innovation mindset and ability to institute changes in teams may be easier in smaller practices than in very large practices within health systems.15 Our experience would suggest that these factors are critically important in responding to change.
The Future
As of this writing, we still find ourselves in the COVID-19 public health emergency. Soon, we will find out if exemptions for telehealth billing will continue to allow primary care virtual visits to be reimbursed comparably to in-person visits; lifting these exemptions will likely erode much of the implementation progress to date. However, patient response to telehealth is newly emerging. Regardless of their concerns of contracting COVID-19, many patients report being highly satisfied with telehealth for certain types of visits and conditions. Access to care seems to be improved for certain populations.16 However, other patients have not been able to accommodate to telehealth, and many vulnerable groups may be left behind.17⇓–19
How can access and care be improved for these patients? If telehealth continues, how will teams function in a world blended with in-person and telehealth options? Where will telehealth be physically conducted by each of the team members? These and many more questions will need to be answered in the future. In an innovative commentary, Jenny Gray in “A Fast Start That Fizzles” offers specific recommendations for strategies to make new innovations “stick.”20 Intentional efforts will need to be made to create the policy and organizational changes to best accommodate changes that have resulted from COVID-19, including telehealth. Outlined in the Gray article are ways to map out intentional decisions including who to involve and how to understand the motivation and perspectives of diverse stakeholders. Beyond efforts in individual practices and health systems, there is opportunity to understand and apply learning about effective implementation as a discipline of family medicine. Implementation science may be helpful for the field of primary care in providing both a lens and specific methods to assist in adoption and sustainment of new innovations.21 Many insights will emerge in the coming year to produce new solutions to accommodating these changes and finding out which ones “stick.” Let us all pay attention and keep track of what we learn in support of primary care as a vital source of care in the United States.
Notes
This article was externally peer reviewed.
Funding: None.
Conflict of interest: None.
To see this article online, please go to: http://jabfm.org/content/34/Supplement/S196.full.
- Received for publication August 6, 2020.
- Accepted for publication September 9, 2020.
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Intimate Partner Violence and Telemedicine Usage and Satisfaction Early in the COVID-19 Pandemic
- Care Redesign to Support Telemedicine Implementation During the COVID-19 Pandemic: Federally Qualified Health Center Personnel Experiences
- Telehealth's future in Australian primary health care: a qualitative study exploring lessons learnt from the COVID-19 pandemic
- Telehealth's future in Australian primary health care: a qualitative study exploring lessons learnt from the COVID-19 pandemic
- Points of Concordance, Points of Discordance: A Qualitative Examination of Telemedicine Implementation
- Practice Adjustments Made by Family Physicians During the COVID-19 Pandemic
- Primary Care in the COVID-19 Pandemic: Essential, and Inspiring