
Abstract
Background: Primary care is crucial to the health of individuals and communities, but it faces numerous structural and systemic challenges. Our study assessed the state of primary care in Virginia to prepare for Medicaid expansion. It also provides insight into the frontline of health care prior to an unprecedented global COVID-19 pandemic.
Methods: We surveyed 1622 primary care practices to understand organizational characteristics, scope of care, capacity, and organizational stress.
Results: Practices (484) varied in type, ownership, location, and care for medically underserved and diverse patient populations. Most practices accepted uninsured and Medicaid patients. Practices reported a broad scope of care, including offering behavioral health and medication-assisted therapy for opioid addiction. Over half addressed social needs like transportation and unstable housing. One in three practices experienced a significant stress in 2019, prepandemic, and only 18.8% of practices anticipated a stress in 2020.
Conclusions: Primary care serves as the foundation of our health care system and is an essential service, but it is severely stressed, under-resourced, and overburdened in the best of times. Primary care needs strategic workforce planning, adequate access to resources, and financial investment to sustain its value and innovation.
- COVID-19
- Family Medicine
- Health Policy
- Medicaid
- Medically Underserved Area
- Primary Health Care
- Research Report
- Surveys and Questionnaires
- Virginia
- Workforce
Introduction
Primary care plays a critical role in promoting the health of individuals and communities. The provision of primary care has been shown to decrease mortality, improve health outcomes, promote equity, and more efficiently use limited health care resources.1⇓–3 Patients with a usual source of primary care are healthier and are more likely to receive recommended care. In the United States, more than 35% of health care visits are to primary care clinicians,4 who can address the spectrum of health needs including prevention, chronic disease management, acute care, and behavioral health. Primary care clinicians can serve as an entry point to health care, as well as provide continuous, coordinated, and comprehensive care for patients and populations.5 Given its value and broad reach, high-quality primary care can be an essential force for promoting health equity.
Despite our need for high-quality primary care, we only have a superficial understanding of the state of primary care. Compared with other developed countries, the United States has an inadequate supply of primary care providers.6 Students increasingly chose to pursue more lucrative specialty careers. Primary care is under-resourced, receiving only 5% of health care expenditures, requiring practices to do more with less.4 While licensure data can be used to identify primary care clinicians, it is more difficult to identify primary care practices. As a result, less is known about the distribution and location of primary care practices, practice composition of clinicians and staff, services provided, ownership and organizational structure, and stress and stability. Understanding these factors is essential to ensure primary care design broadly meets the needs of communities.
In January 2019, Virginia became the 33rd state to expand Medicaid coverage. The state anticipated up to 500,000 previously uninsured residents with family incomes less than or equal to 138% of the federal poverty line becoming insured. To determine whether primary care practices could meet the new demand for care, we sought to evaluate the current state, capacity, and stresses of Virginia's primary care practices. Virginia, which is in the 50th percentile nationally for the overall size and makeup of primary care,7,8 may be generalizable to other settings as well for understanding the state of primary care nationally.
Methods
We queried the 2018 Virginia Department of Health Professions (VDHP) licensure data and the 2016 Virginia All Payer Claims (APCD) to identify all active primary care clinicians and their practices in the state.9,10 Between October 2018 and March 2019, we surveyed every identified primary care practice to understand their characteristics, affiliations, scope of care, patient accessibility, and the system pressures and stresses they face. The Virginia Commonwealth University Institutional Review Board deemed this not human subjects research.
Primary Care Practice Identification
We sought to identify all adult primary care practices including family medicine, general internal medicine, preventive medicine, and geriatric practices. Since the overarching goal of our study is to understand primary care practice capacity for Medicaid expansion, we excluded pediatric practices as all children in Virginia were already eligible for Medicaid. We also excluded obstetric and gynecologic practices because we were not able to determine which practices provided primary versus specialty care.
To identify primary care practices, we followed a 6-step process. First, we identified primary care clinicians and their practice from the VDHP licensure files by self-designated specialty type and practice name and address.11 Second, we manually reviewed practice names and excluded all those appearing to be specialty practices. For example, a self-designated primary care clinician in a practice with “cardiology care” in its name would be excluded. Third, we queried the APCD and removed clinicians with no claims, assuming they represented retired or nonpracticing clinicians.9 Fourth, we identified all clinicians with 50 or more claims in the APCD that were not in the VDHP licensure file (n = 715) and manually conducted internet searches to determine if they were a primary care clinician and if their practice was in Virginia.
Fifth, from the VDHP and APCD we assembled a comprehensive list of practice names and addresses. As the VDHP data were self-reported, there was some variation in how clinicians listed the same practice. By cross querying listed practice name and listed address and manually reviewing content, the list was refined. For example, we verified whether 2 clinicians that shared the same address but listed their practice name slightly differently actually practiced in the same or different practices using internet queries. Practice name was identified from the VHDP. Since nearly a third of clinicians did not report a practice affiliation, we identified those practice affiliations by internet searches and local connections within our state's practice-based research network, the Virginia Ambulatory Care Outcomes Research Network (ACORN). Clinicians who could not be matched or found through internet queries were excluded from the analyses. Finally, our practice list was further refined based on our survey responses, described below.
Practice Survey
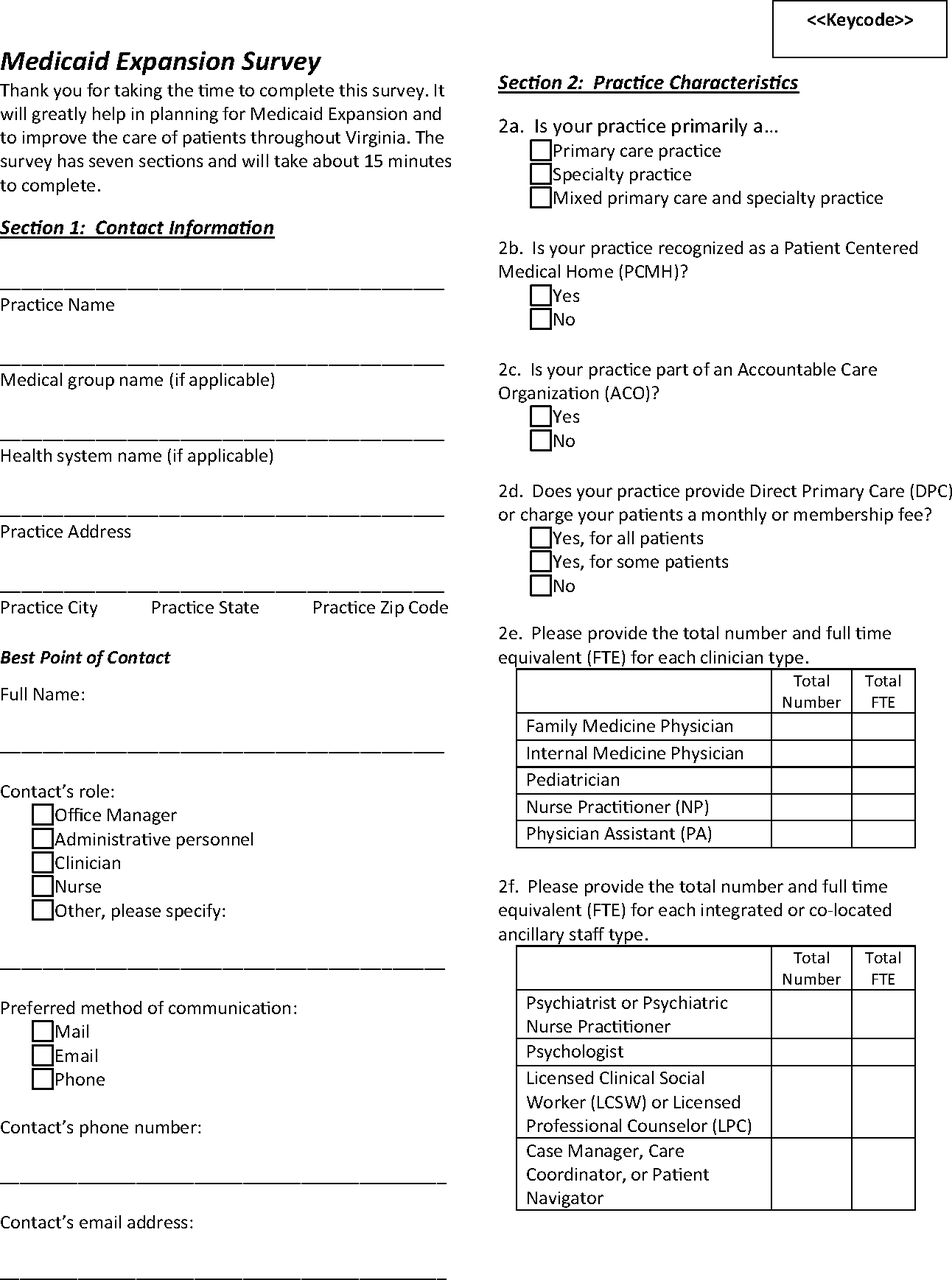
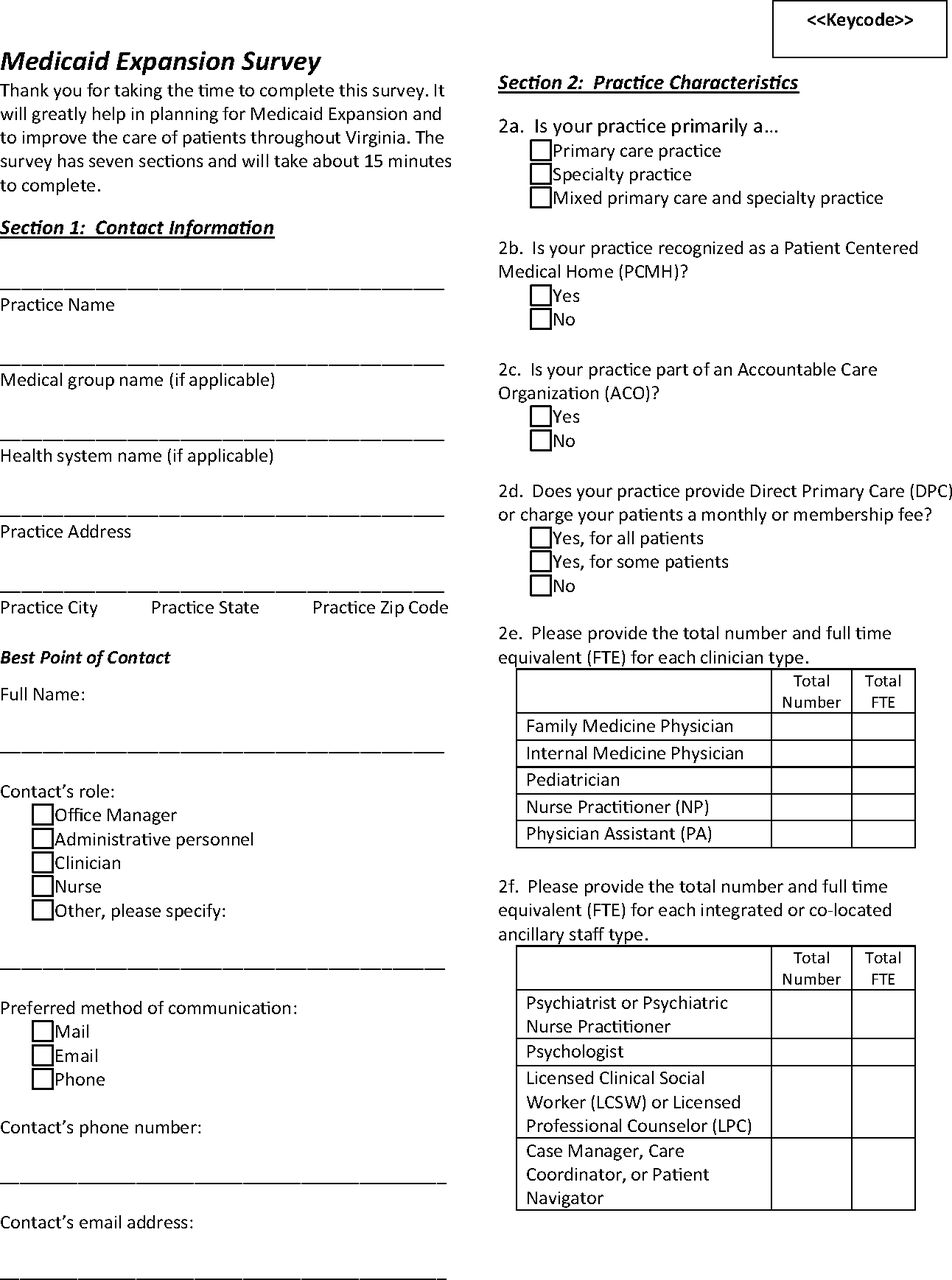
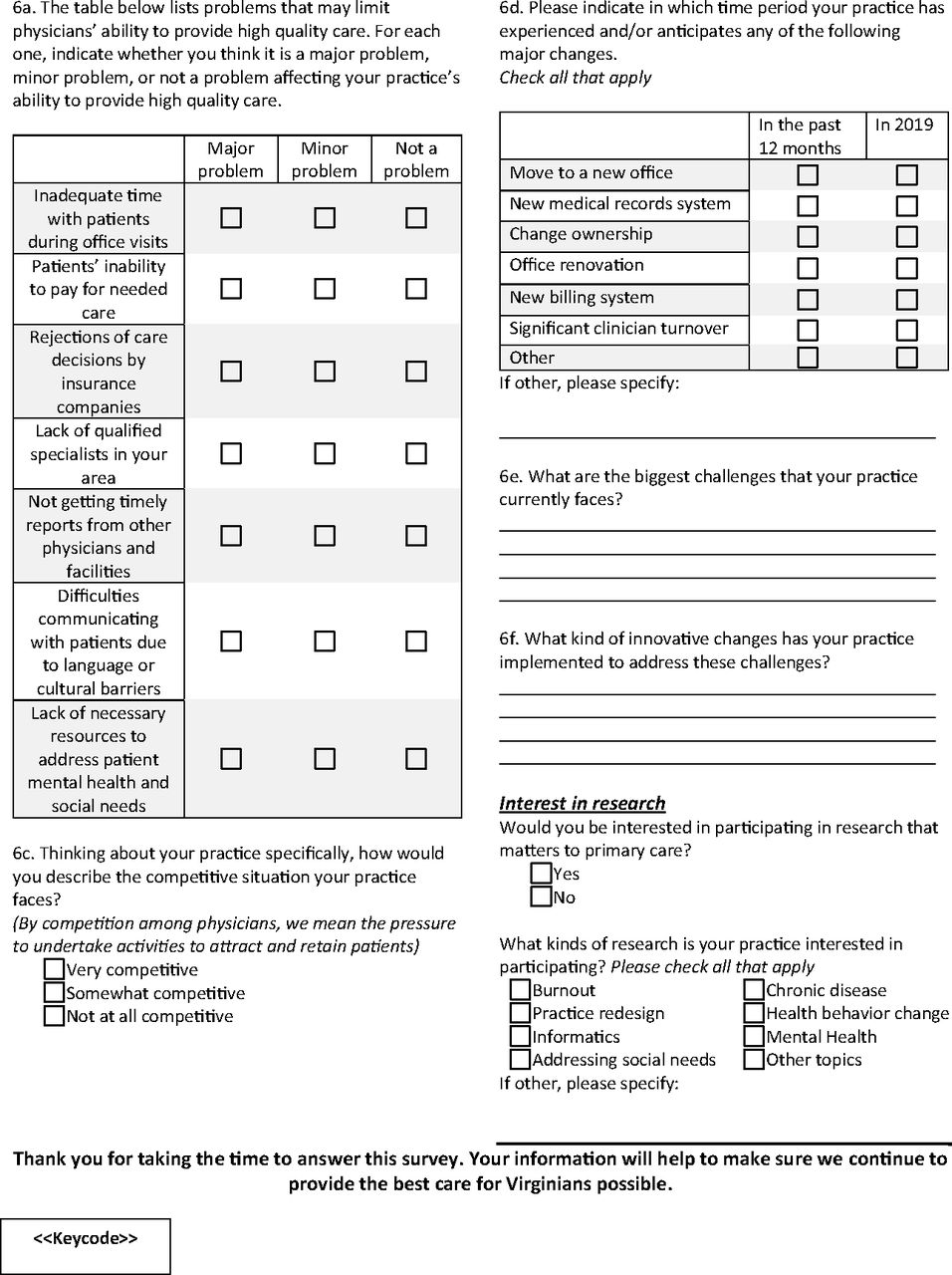
The practice survey questions were drawn from several sources. Questions were selected based on information needs and experiences from the Department of Medical Assistance Services (DMAS) and ACORN. Questions from the annual ACORN practice inventory assessed practice size, affiliations, population served, panel size, patients seen per day, and services offered; questions have been used in ACORN surveys of practices for the past decade and were developed from the VDHP licensure questions, American Board of Family Medicine Graduate Survey, American Association of Medical Colleges (AAMC) Physician Survey of Primary Care, and assessments of the patient-centered medical home.12⇓–14 Questions from the Healthy Michigan Plan's physician survey assessed a practice's clinician capacity, payer mix, practice environments, strategies to provide access to care, intent to see more Medicaid beneficiaries, and barriers to caring for Medicaid beneficiaries.15 Questions were drawn or adapted from additional studies to assess how practices addressed unhealthy behaviors, mental health, and social needs; major changes the practice experienced or anticipated; and the perceived competitiveness of the market.16⇓–18 We considered experienced or anticipated major practice changes and competitiveness of the local market as surrogates for practice stress. See Appendix for the full survey instrument.
Using the identified addresses and e-mails, practice surveys were mailed, faxed, or e-mailed to all primary care practices in Virginia. When possible, invitations were directed to a known senior practice clinician or administrator. The survey included a cover letter from the Virginia secretary of health to explain the purpose and importance of the survey. Practices were reminded up to 6 times to complete the survey, including telephone reminders to nonresponders. In addition, the Virginia Academy of Family Physicians, Virginia Chapter of the American College of Physicians, Medical Society of Virginia, and ACORN e-mailed all their primary care members an electronic survey for completion, asking them to identify a practice lead to complete the survey, referencing that they may have already received and completed a survey, and asking each practice to only complete the survey once. If we received duplicate surveys for a practice, we only included the first survey response in our analysis.
Statistical Analysis
Our unit of analysis was the primary care practice. We provided descriptive summaries such as percentages, counts, and means based on practice survey responses. We geocoded all primary care practices' addresses. A χ2 goodness-of-fit test was used to compare the geographical distribution of practice survey respondents to that of all practices, using ZCTA as the unit of analysis. SAS version 9.4 (Cary, NC) was used for analyses and geocoding.
Results
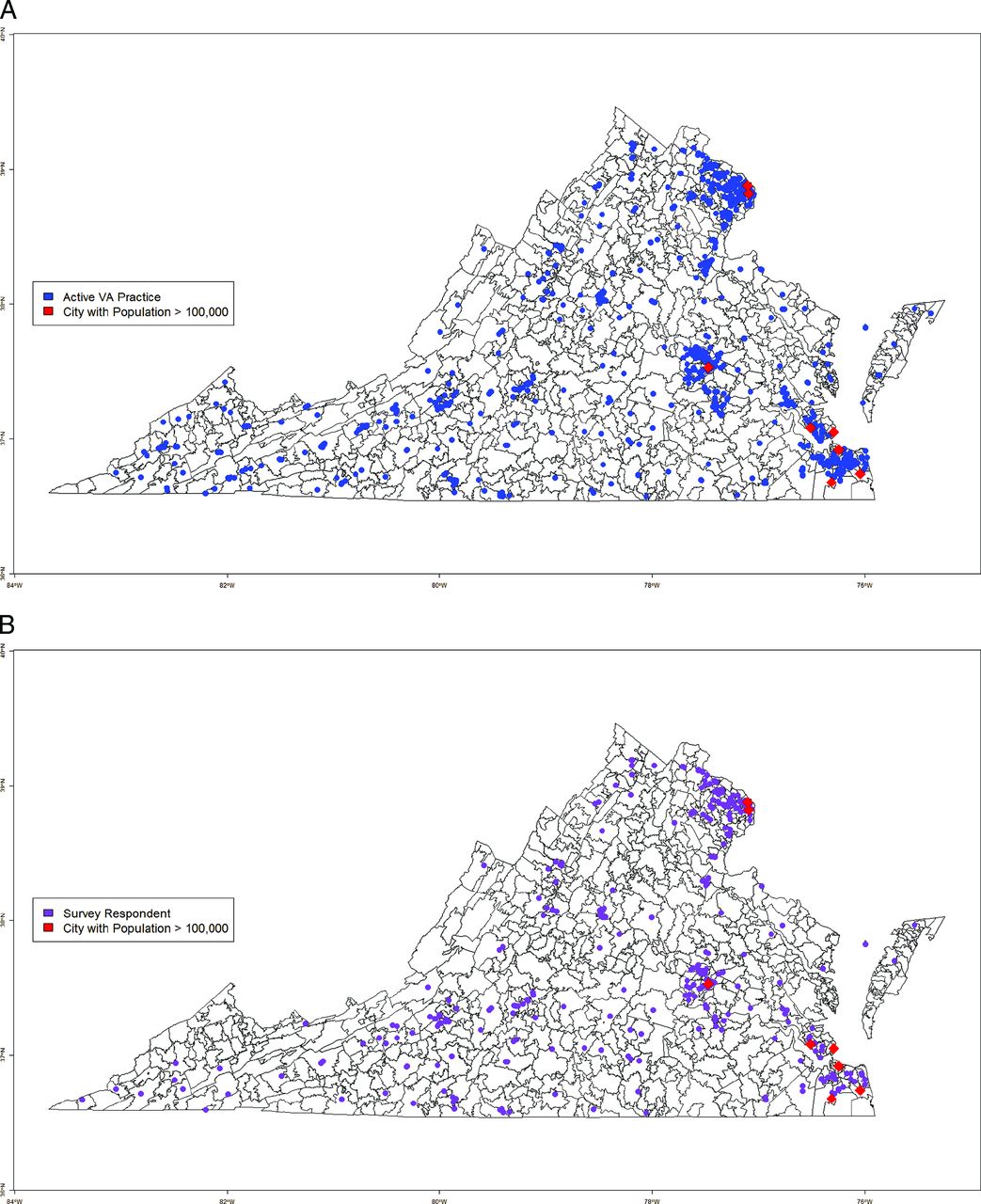
Overall, 484 practices of 1622 completed the survey (29.8% response rate). Survey respondents were representative of primary care practices serving adults throughout Virginia. The geographical distribution of respondents was similar to that of all primary care clinicians (Figure 1), which was supported by a goodness-of-fit test (χ2 test-statistic = 0.4, df = 228, P value = 0.999).

A. Primary care practice distribution in Virginia (n = 1622). B. Primary care practice survey response distribution in Virginia (n = 484).
Practices varied in type, ownership, location, and certifications (see Table 1). Practices were primarily clinician owned (53.4%), followed by health system owned (25.1%). A majority were either part of a medical group (39.7%) or health system (27.9%). Over a third had patient-centered medical home recognition (34.3%) and half were part of an accountable care organization (50.2%). Practices on average had 4.5 clinicians and 1.7 care team member full time equivalents (FTEs). Care team members included behavioral health care providers, social workers, and case managers.
Characteristics of Adult Primary Care Practices in Virginia (n = 484)
Populations Served
Practices reported caring for diverse patient populations that generally reflected the commonwealth's demographics (Table 1).21 Practices reported caring for a slightly greater proportion of racial/ethnic minority patients than the proportion that reside in Virginia, estimating their practice population to be 64.4% White, 24.5% Black, 8.3% Asian or Pacific Islander, 2.8% Native American or Alaska Native, and 11.1% Hispanic/Latino. An average of 41.4% of practices reported having at least 1 clinician who can deliver care in a language other than English.
Practices also reported caring for high proportions of medically underserved populations (Table 1). Practices reported a payer mix of 10.2% uninsured, 11.9% Medicaid, 29.4% Medicare, and 48.2% commercial or private insurance. Fully 89.7% of practices reported accepting new uninsured patients, and 87.9% were accepting new Medicaid patients. A high proportion of practices were located in more historically underserved rural communities (53.0%), while only 12.1% of Virginians live in a rural community.22
Access to Care and Scope of Practice
Practices reported multiple strategies to improve access to care (Table 2). Strategies to improve access to care include 89.7% of practices providing same-day appointments, 42.2% evening and weekend access, and 67.4% 24-hour phone access. Furthermore, practices made accessing ancillary services easy, with 70.7% of practices having onsite laboratory and 30.4% onsite radiology services. At the time of the survey (ie, prepandemic), 21.1% offered telehealth services and 11.0% offered group visits.
Primary Care Efforts to Ensure Access to and Comprehensiveness of Care
Practices reported a broad scope of care beyond the usual primary care domains of acute, chronic, and preventive care (Table 2). Most practices reported some degree of behavioral health including mental health screening (83.7%), patient handoff to mental health clinicians (52.3%), and even colocated mental health clinicians (18.2%). Many practices also address substance abuse disorders, with 80.6% of practices providing smoking cessation counseling, 65.9% alcohol misuse treatment, 23.1% opioid misuse treatment, and 23.1% medication-assisted therapy for opioids. Many practices even reported efforts to help patients address social needs such as helping patients with out-of-pocket medical expenses (81.3%), food insecurity (52.2%), transportation (59.5%), unstable housing (52.2%), and unemployment (38.9%).
Practice Stress
One in 3 practices reported experiencing a significant stress or change in the prior year (see Table 3). Stresses reported by practices included clinician turnover (13.2%), a major office renovation (11.4%), adopting a new electronic health record (8.9%) or billing system (6.6%), moving to a new location (6.0%), and changing practice ownership (2.7%). Some practices reported experiencing 2 stresses (8.9%), though few reported 3 or more stressors (0.3%). Complicating these stressors, 72.7% of practices reported that their practice environment was somewhat or very competitive.
Recent and Anticipated Stresses Experienced by Primary Care Practices
Discussion
At the time of our survey (fall 2018 to spring 2019), primary care practices in Virginia were well poised to address the needs of new patients in the runup to Medicaid expansion. Practices had several services and strategies to ensure access to care as well as to address a broad range of traditional health care, health behavior, mental health, and even social needs for Virginians. Practices were distributed throughout the commonwealth, with a high proportion in rural communities that likely otherwise have limited access to health care. Practices also reported caring for higher proportions of racial/ethnic minority populations, patients with Medicare and Medicaid, and non-English-speaking patients. Most practices reported a willingness to care for new Medicaid beneficiaries and even the uninsured. This collectively demonstrates primary care's essential role in caring for socially and economically marginalized and medically underserved people.19
During the COVID-19 pandemic, which disrupted our entire health care delivery system, exacerbated mental health and social needs, and disproportionately harmed and killed the most vulnerable people,20⇓–22 primary care was even more necessary and showed its ability to rapidly adapt. To continue to care for patients, primary care practices ramped up existing telehealth systems, implemented new infrastructure, redefined care team member roles, and learned a new way of practicing medicine.23 A longitudinal, national, primary care survey, administered since the start of the pandemic, further documented how primary care increased support for mental health (65% of respondents), increased support for substance abuse (22% of respondents), and waived copays and reduced fees (20%).24 We will also be repeating our survey every 2 years to update these findings and document emergent changes and challenges to primary care practices in Virginia in the wake of the pandemic.
Of concern, primary care in Virginia, and likely nationally, is overburdened, under-resourced, and stressed. We found that 1 in 3 practices reported a major change, like new ownership or changing electronic medical records. These changes represent major disruptions that can be expected to strain care delivery and the personal lives of clinicians and staff. Even without these major changes, prior research suggests that primary care suffers from excessive workloads and a high volume of clerical and bureaucratic tasks, documentation mandates, authorizations and preapprovals, and other regulations and mandates.25,26 As a result, the norm is for clinicians to work during evenings and weekends to meet these demands.26⇓–28 Further, an aging primary care workforce and frequent staff turnover risk creating discontinuities in the institutional knowledge, capacity, and culture of practices. In fact, in our study, 20% of the primary care clinicians that we identified were over age 65 years and only 12% were below the age of 40 years.
Not surprisingly, national studies indicate that between a quarter and two thirds of primary care clinicians report being burned out.29⇓–31 Rates vary depending on years in practice, gender, and practice and health system leadership. The COVID-19 pandemic and possibly Medicaid expansion in Virginia likely added to this strain and burnout. Nationally, nearly 30% of those physicians who died from COVID-19 were primary care.32 During the pandemic, 2 of 3 practices reported that they were experiencing stress at an all-time high.24 As a result, 57% of clinicians in that survey reported a health decline from stress, a fifth of practices reported having clinicians retiring early, nearly half of practices reported furloughing or laying off staff, and 19% of practices reported a risk of permanently closing.
Our study has 2 key limitations. First, we had a response rate of 30% for our practice survey. Respondents do seem to be representative of primary care in Virginia with respect to geography, practice type, and patient population, but we cannot assess representativeness in terms of scope of practice or stresses experienced. While we would prefer a higher response rate, we are not aware of any similarly comprehensive statewide survey of primary care. Second, practices self-reported their perception on scope of practice, accessibility, and populations served. Practices may overestimate their scope of practice and service to medically underserved populations. We were able to compare the proportion of practices with Medicare and Medicaid claims with survey responses, and they were generally consistent.
Conclusion
Primary care is diverse and widespread throughout Virginia. It serves as the foundation of our health care system and is an essential service and public good. Virginia practices are present in every community, have many strategies to enhance access to care, including a wide scope of practice that is necessary to address the root causes for poor health, and are poised to meet the needs of medically underserved people. Despite its necessity and value, primary care reported being severely stressed. Stress is primary care's resting state and is expectantly worse due to the COVID-19 pandemic. The strengths, weaknesses, and points of strain in practices identified here can hopefully be used to inform strategies for reinvesting in primary care. We hope that other states and regions can benefit from doing similar assessments, combining local knowledge with existing data sources. Such an assessment is critical to ensure that primary care can adequately care for our communities.
Acknowledgments
Other substantial contributions: The authors thank the following students for assisting with data cleaning and formatting, internet searches, mailings, project coordination, and transcript coding: Karina Armenta, David Branson, Tatiana Brown, Kyandra Rivera DeJesus, Jake Giovia, Suha Hafeez, Sarah Owais, Hannah Rak, and Malaika Sohail. We would also like to thank the Virginia Academy of Family Physicians, the Medical Society of Virginia, the Virginia Center for Health Innovation, and the Virginia Department of Health for helping to promote the survey.
Appendix




Notes
This article was externally peer reviewed.
Funding: Funding for this study was provided by the Department of Medical Assistance Services and the National Center for Advancing Translational Sciences (UL1TR002649). The opinions expressed in this manuscript are those of the authors and do not necessarily reflect those of the funders.
Conflict of interest: The authors of this manuscript have no conflicts of interest to disclose, beyond being primary care clinicians and researchers.
Disclaimer: Dr. Krist is a member of the US Preventive Services Task Force (USPSTF). The findings and conclusions in this document do not necessarily represent the views of the USPSTF. No statement in this manuscript should be construed as an official position of the USPSTF.
To see this article online, please go to: http://jabfm.org/content/34/6/1189.full.
- Received for publication February 2, 2021.
- Revision received June 7, 2021.
- Accepted for publication July 21, 2021.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}