
Abstract
Purpose: To understand patient attitudes, access toward video calling to enhance efficiency of after-hours triage calls.
Methods: We surveyed patients aged 18 to 89 years. Questions included demographics, preferences, access to video calling devices, and perceived advantages and disadvantages of this technology. Answers were entered into Qualtrics database and analyzed using JMP 11 (SAS, Cary, NC).
Results: Two hundred ninety-eight patients agreed to participate. Mean age was 47.9 years; 71.6% were female; and 75.1% had access to video calling device. Device proficiency was inversely related to age and greatest in 18-to-32-years group (χ2 = 71.18, P < .0001). Seventy-one percent of patients enjoyed video communication, directly proportional to education (trend test Z = 2.78, P < .005). Adjusted for both age and education, respondents with college education or above were 3 times more likely to self identify as “good' with video (OR, 3.11; 95% CI, 1.48-6.64); those under age 48 had even higher proficiency (Odds ratio (OR), 13.9; 95% CI, 4.79-59.34). Patients with prior video experience were 3 times more likely to prefer video calling (Relative risk (RR) = 3.46; 95% CI, 1.95-6.11). Patients calling their doctor 5 or more times annually preferred video calling significantly more than calling by telephone (RR, 1.61; 95% CI, 1.31-1.97). Faster contact with the primary care provider (19.8%) was the most perceived advantage. Loss of in-person interaction with doctor (37.1%) was the greatest perceived disadvantage.
Conclusions: Patients seem to have access and interest in video communication for after-hours calls. Further studies are needed to evaluate whether addition of video component to after-hours triage calls will help reduce unnecessary emergency department visits.
Introduction
With the increased popularity and convenience of technology, there have been attempts to incorporate technology into the workplace, specifically the health care sector.1 Telemedicine, through various communication strategies, such as video consultation and phone services, already allows patients the convenience of speaking with their physicians from their preferred environment and removes added and often unnecessary time and travel costs associated with patient encounters.2 However, using video calling for after-hours triage has not been studied extensively but would provide patients with more health care options beyond normal clinic hours than just visiting the emergency department (ED).
Overcrowding in EDs is a concerning global problem and has been identified as a national crisis in some countries due to decreased patient safety and increased mortality, delays in initiation of critical care, and inefficient inpatient flow.3 To improve the continuity of care and decrease the number of unnecessary visits to the ED, thereby removing the burden on ED physicians, triage systems for after hours in the clinic have been implemented.4
Currently, most after-hours triage offer phone services allowing patients to call the clinical staff and speak with an on-site physician or nurse who can direct them on further course of action.5 Such instruction on behalf of the physician may include advising the patient to seek immediate attention at the ED or wait until the next day to meet with their primary care provider (PCP) in person. In some cases, treatment may even be prescribed without seeing the patient's condition first hand.6 A 2009 study done on “tele triage” via telephone showed a decrease in the number of same-day visits to the PCP when phone service was used.4 Furthermore, the researchers concluded that 50% of cases could be handled entirely through phone and suggested that this service may have the potential to reduce patient volume in the ED.4
While phone services are promising, the lack of visual cues may lead to uncertainty in evaluating the patient's condition.7 Therefore, we are interested in the possibility of incorporating video communication into after-hours triage to determine whether this could help prevent unnecessary ED visits, thereby saving patients and hospitals both time and money. Since implementation of technology into the health care setting is still controversial due to its often-perceived effect of increasing distance between patients and physicians and potentially affecting patient/physician privacy, it is necessary to gauge patient interest in tele-triage options. Thus far, a study in the UK surveying patients on their technological expertise and willingness to communicate with their doctors through video calls found that younger patients and those with greater technological experience were more likely to prefer video communication.8 However, no studies have been conducted in the United States regarding public receptiveness toward video calling in after-hours triage. This study investigates the attitudes of patients toward after-hours video calling with their health care provider, along with accessibility and any perceived advantages or disadvantages of video communication. The information gathered is intended to provide a platform for future research involving video communication triage that may help improve patient care.
Methods
The study was reviewed and approved by the institutional review board at Eastern Virginia Medical School before implementation. It is a cross-sectional study where surveys (supplement 1) were administered to a convenience sample of patients aged 18 to 89 years who came for a visit at an academic family medicine clinic in Norfolk, Virginia. Patients had the option to decline the survey. Questions included demographic information, availability, and access to devices that allow video calling. Patients were also asked about perceived advantages and disadvantages related to video calling with their health care provider and if they would prefer video calling in place of telephone communication. Certain questions allowed free responses for any additional details that the patients wanted to provide. Surveys were distributed to patients on check-in. While patients had the option of answering the survey themselves, a research team member was available at the check-in area to assist patients who needed help in completing the survey. Completed surveys were then transcribed by research team members and answers were entered into a Qualtrics database. Data analysis was done using JMP version 11.2.1 (SAS, Cary, NC). Evaluation included descriptive statistics,χ2 for categorical variables with α set at 0.05, relative risk with 95% CIs, odds ratios calculated using logistic regression to adjust for potential confounders involving dichotomous outcomes, and Cochrane Armitage trend tests.
Results
Demographics
Three hundred patients were offered the survey, of whom 298 agreed to participate: 213 (71. 6%) were females and the mean age was 47.9 years (Table 1). One hundred twelve (37.6%) patients had access to a smart phone and 111 (37.5%) to desktop or laptop. Tablets, smart watches, and smart TVs were some of the other devices patients owned that had capability for video calling. When ownership of a smart phone was compared between income levels of less than $25,000 and greater than $25,000, the Pearson's c2 test showed no significant difference, with most individuals in both income categories owning smartphones (χ2 = 2.299; P = .130; relative risk, 1.603; 95% CI, 0.863-2.98).
Demographics of Patients Surveyed at Ghent Family Medicine Clinic
Technology Use, Proficiency, and Enjoyment
One hundred ninety (63.9%) patients had used video calling at home while 66 (22.3%) had used it at work. One hundred thirty-one (44%) patients said they use video communication extremely rarely and 86 (29.1%) use it more than once a week or every day. One hundred sixty-two (54.4%) patients spoke with their doctors or nurses over telephone to discuss medical problems, predominantly for prescription-related questions (72, 24.3%), minor illnesses (66, 22.2%), general medical advice (54, 18.3%), follow-up on chronic conditions (49, 16.6%), skin rashes (15, 5.3%), emergencies (15, 5.3%), mental health issues (14, 4.8%), and others (9, 3.1%). Some of the answers submitted in free text included pediatric health issues, women's health–related issues, and test results.
One hundred forty-nine (50.2%) patients said they were extremely good at using devices that allowed video communication (Figure 1). In general, device proficiency was inversely related to age in a significant manner, with the greatest reported proficiency occurring in the 18-to-32-year age group (χ2 = 71.180, P < .0001). Two hundred eleven (71%) patients surveyed enjoy video communication; in general, people with higher levels of education tended to enjoy video more, as demonstrated by the Cochran Armitage Trend Test (Z = 2.780, P < .005). Adjusted for both age and education, respondents with college education or above were 3 times more likely to self identify as “good' with video (Odds ratio (OR), 3.11; P = .0028; 95% CI, 1.48–6.64); and those under age 48 years had even higher proficiency (OR, 13.9; P < .0001; 95% CI, 4.79–59.34).
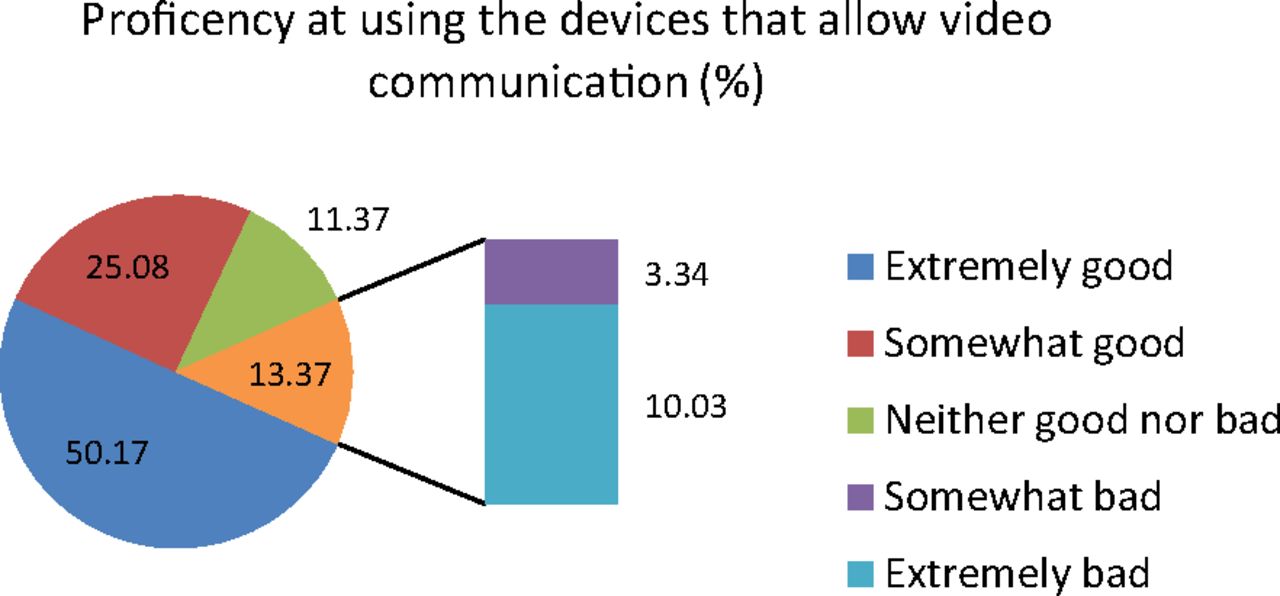
Proficiency in using video communication.
Preference for Video Calling
One hundred sixty-five (55.4%) patients said they would prefer video calling over talking to their health care provider through telephone while 75 (25.4%) would like to use it all the time and 225 (75.6%) would like to use it only sometimes. The Cochran Armitage Trend Test showed a significant association between preference for video and age (Figure 2); specifically, younger individuals tended to prefer video more with the exception that the greatest level of preference was found in the 33-to-47-year age group rather than the 16-to-32-year age group (Z = −3.862, P < .0001). Generally, women tended to prefer video calling with their doctor over discussing via phone compared with men (χ2 = 5.089; P = .024; relative risk, 1.34; 95% CI, 1.01–1.77). No significant differences in preference for video calling with the physician were found between different races or education levels. In addition, patients who had prior experience with video communication were more likely to prefer video calling with their doctors in place of communicating over phone (χ2 = 35.700; P < .0001; relative risk, 3.46; 95% CI, 1.95–6.11). Patients who called their doctor 5 or more times annually preferred video communication significantly more than patients who called less than 5 times annually (χ2 = 21.3; P < .0001; relative risk, 1.61; 95% CI, 1.31–1.97).

Prefer video calling by age quartiles.
Advantages and Disadvantages of Video Calling
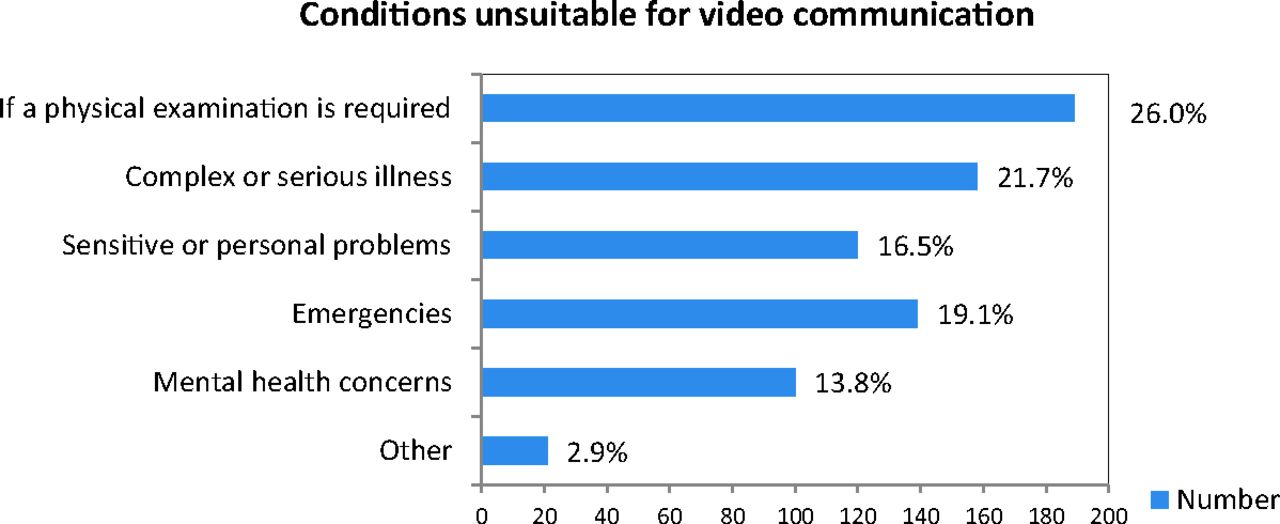
Faster contact with the PCP rather than waiting for an appointment (59, 19.8%) was the most frequent perceived advantage of video calling (Table 2). Other advantages that were submitted by free text included ability for the doctor to see what is going on with patient, ability for the patient to see the doctor's body language, saving time for minor injury and rash evaluation, and allowing family members to be included in the interaction. Table 3 shows that wanting to have a face-to-face in-person interaction with a doctor was the greatest perceived disadvantage (110, 37.1%). Answers that were also offered by patients included feeling self conscious, self perception of not being good with technology, miscommunication and possibility of causing more harm, concerns about quality of video call, worry about appearance, visual impairment, and ability to get distracted by things in the background. Illness requiring a detailed physical examination (77, 26%) were not preferred for video communication (Figure 3).

Medical conditions unsuitable for discussion over video communication.
Advantages of Video Calling
Concerns Toward Video Calling
Discussion
“After-hours care” refers to care for medical problems arising between 5 pm and 8 am, and on weekends and holidays, that could be appropriately managed by the patient's primary care physician/team.9 Several primary care teams have an “after-hours telephone line” where patients can call for concerns that are not life threatening. The call is directed to an on-call nurse or physician who either provides advice over phone, refers the patient to the ED, or recommends follow-up with PCP when clinic reopens.
By removing accessibility barriers and providing a convenient option for patients, current telephone triage services during after-hours primary care may help to reduce the burden on ED resources, address immediate health concerns, and target a greater range of patients in rural areas who may not be able to access an ED in a timely manner.10 In addition, such a service maintains continuity of care for patients during after hours, in contrast to Urgent Care facilities, which despite convenience, require patients to meet with a provider who does not know their medical history. However, the severity of the illness is often difficult to interpret due to poor patient description of symptoms over telephone; patients are anxious and have difficulty explaining their condition and subsequently get referred to the ED or Urgent Care for further evaluation.
We believe that the addition of a video component to after-hours telephone calls would improve the quality of advice provided and hence would avoid unnecessary referrals to the ED. Our aim is to assess patient interest in and concerns regarding video calling for enhancement of after-hours triage to ultimately reduce burden on the ED by minimizing unnecessary referrals. With the current emphasis on social distancing due to the COVID-19 pandemic, avoiding visits to the ED as much as possible would benefit both patients and providers by limiting exposure.
Our study was conducted in an academic family medicine clinic in Norfolk, Virginia; the second most populated city in the state with the largest naval base in the world, serving a diverse range of socioeconomic, demographic, and geographic locales. The population of Norfolk, Virginia is 41.2% African American with a median household income of $47,137, while our study had 63.7% African American participants and 56% participants had annual household income less than $50,000. Our research found that income levels did not seem to be a barrier for access to video communication, since both patients below and above the federal poverty level generally owned smart phones; this contrasts with the study by Johnston et al, which showed a socioeconomic gap in access to technology and provides promising evidence that incorporation of technology into the health care setting will not create an economic bias in delivery of care.8 While most patients had familiarity with video communication, younger people were more likely to have greater proficiency than older individuals, which is consistent with prior literature.11 Reasons for reduced proficiency in the elderly include a deterioration in cognitive, motor, and sensory capabilities such as decreased color perception and peripheral vision, nearsightedness, diminished hearing—especially of higher-pitch sounds, impaired fine motor skills and coordination, along with compromised memory and attention.12 Other potential explanations for reduced expertise of technology in older adults include lack of integration of technology into work and personal lives along with decreased self confidence regarding technology use.13,14 This may be a concern because elderly patients tend to regularly visit the PCP more.15 However, as technology becomes more heavily integrated into the business and personal aspects of people's lives at increasingly earlier ages, it is likely that future generations of patients will be comfortable using technology even into old age. Overall, most patients claimed to use video calling infrequently so the fact that this service is not popularly utilized may have a greater impact on its successful implementation into clinical practice than level of proficiency. “Video call triage” in the context of our study as opposed to the broader term telemedicine is possible based on the widespread availability and use of smartphones, even in low-income populations. Telemedicine in the modern sense often requires more intensive resources and investment. What we have observed is that “video call triage” as a subcategory of telemedicine may be feasible with existing resources and technology.
In general, most patients enjoyed video communication, and this correlated with higher education levels. A little over half of patients claimed discussing medical problems over phone and nearly the same percentage of individuals said they would prefer discussing such concerns over video instead; this preference was more likely in younger individuals as well as women, patients with prior video calling experience, and those who enjoyed video communication. The finding concerning women is in agreement with prior literature showing that women are more likely to use various media, such as Internet and video calling, to connect with others compared with men.16
While advantages of video calling centered on faster contact, patients still expressed concerns about wanting in-person interaction with their health care provider and possibilities of miscommunication or poor video quality. While these concerns are valid, video triage is still one of the few options allowing patients to seek immediate cost-effective care after normal clinic hours when the only other courses of action include making an expensive visit to the ED or Urgent Care center or attempting to schedule an in-office appointment which, depending on availability, may delay care and further compromise the patient's health. Although miscommunication and connection issues are potential drawbacks of video calling, after-hours triage can be advertised to patients for only conditions that are most suitable for this medium, particularly conditions whose diagnosis can be achieved by obtaining an accurate history and review of systems alone. The common cold, flu, viral gasteroenteritis, and musculoskeleton pain are just a few such examples.17 Despite the visual component of video communication, the majority of patients deemed serious illnesses and those requiring a physical examination as unsuitable for discussion over video.18 Such illnesses would be better worked up in a facility with greater resources such as the ED; however, video-call triage beforehand may still give patients a better sense of how concerning symptoms are and what the appropriate next step is.
Smart-phone use and privacy issues have been reviewed and discussed in various settings, with particular concern for HIPAA compliance in securing protected health information.19,20 In a 2016 study, only about 5% of residents in training at that time “often” or “routinely” used Health Insurance Portability and Accountability Act (HIPAA)–compliant smart-phone applications for patient interactions.21 While popular video-communication media such as WhatsApp are encrypted, many are not HIPAA compliant. In addition, many professional communication applications marketed as “telehealth,” such as Doximity and DocsInk are aimed for communication between health care providers and allow only physician-initiated contact with patients, rather than the other way around. Such applications would inhibit patients from contacting physicians when they have health concerns after normal clinic hours. However, a few video-conferencing sites such as Doxy.me and TheraNest as well as several electronic medical record systems provide HIPAA-compliant patient portals for communication either free or for a small monthly fee. A comparative list of the capabilities and costs of available resources has been provided by some state medical associations.22 Family physicians and other providers looking to implement this capability should review. In addition, given the current concerns and inherent risks of face-to-face interactions due to the COVID-19 pandemic, the US Department of Health and Human Services has relaxed to an extent the HIPAA restrictions to facilitate the use of telehealth.23
The results of this study, which showed patient interest in video calling, encourage further follow-up studies testing the effects of implementing video communication into clinical practice, beginning with after-hours triage, on frequency of visits to the ED. Limitations of the study included lack of clarity regarding the concept of after-hours triage, which could have underestimated patients' willingness to use video communication. While some participants did not approve of video consultation in place of in-person appointment, these patients may be more receptive to video during after-hours clinic, when the only other options include going to the ED or waiting until the next available appointment during clinic hours, both of which are more costly or time consuming. Although the data obtained from this study were from a convenience sample at a single practice, we offered each patient at the clinic the opportunity to complete the survey so the results should be representative of the overall population of our practice.
Results of this study generally showed that patients are economically and technologically capable of video calling. However, further multicenter studies looking into patient and physician comfort and concerns with this service during after-hours would help decide whether to implement video calling into the after-hours triage system. It would also help evaluate whether implementing a video component to after-hours triage would reduce unnecessary referrals to the ED.
Acknowledgments
The initial work was done when Dr. Sankaran was a Resident at Ghent Family Medicine Residency Program, Eastern Virginia Medical School.
Appendix
Video Consultation Survey
We are seeking patients to participate in a survey for a research project. This survey is to understand the interest and access patients may have to video consultation on common medical issues with their physician (or primary care provider) by smartphone, computer or other means. We estimate this survey will take less than 10 minutes and may be done while you are waiting.
This survey is anonymous. It is not linked to you as person. Questions deal with ways to discuss medical concerns without making an office visit. This survey may help you by telling us how best to offer this service. There should be little to no risk from answering these questions. Information provided will be reported by groups, not by each person. Any comments you make will be described by themes. If quotes are used, they will not include personal information. You may stop the survey at any time.
I agree to participate in the survey
I do not want to participate in this survey
Q1. What is your gender?
Male
Female
Q2. What is your age to the nearest year?
__________________________________________
Q3. What is your race?
African American or Black
Caucasian or white
Asian
Other
Q4. Are you Hispanic or Latino?
Yes
No
Q5. What is the highest grade or year of school you completed?
Never attended school or only attended kindergarten
Grades 1 through 8 (elementary)
Grades 9 through 11 (some high school)
Grade 12 or GED (high school graduate)
College 1 year to 3 years (some college or technical school)
College 4 years or more (college graduate)
Q6. What is your annual household income from all sources (mark only 1):
Less than $25,000
Less than $35,000
Less than $50,000
Less than $75,000
$75,000 or more
Prefer not to say
Q7. Please select each type of device below that you OWN that may allow video communication (Example: FaceTime, Skype, Whatsapp etc.)
Desktop computer
Laptop
Tablet
Smart phone
Smart watch
Other
Q8 If you answered “other” to above question, please describe below
__________________________________________
__________________________________________
Q9. Please select below each type of device that you otherwise have easy access to (work/friend's device/public library etc.) that allow video communication (Example: FaceTime, Skype, WhatsApp, etc.) and that you would consider using for personal interaction with your primary care provider.
Desktop computer
Laptop computer
Tablet (e.g., iPad, Galaxy, SurfacePro)
Smart phone
Smart watch
Other
Q10. If you answered other to above question, please describe below.
__________________________________________
__________________________________________
Q11. How good are you at using the devices that allow video communication?
Extremely good
Somewhat good
Neither good nor bad
Somewhat bad
Extremely bad
Q12. Have you ever used a device to video call someone?
Yes
No
Q13. If you answered yes to above question, where have you previously used video communication (mark all that apply)?
Home
Work
Friend's device
Public library
Q14. If you answered yes to question 12, where would you PREFER to use video communication for personal medical questions?
Home
Work
Friend's device
Public library
Q15. Do you enjoy video communication?
Yes
No
Q16. How often do you use video communication?
Extremely rare
Less than once a week
About once a week
More than once a week
Everyday
Q17. How many times have you called your doctor's office in the last year by telephone?
less than 5 times
5 to10 times
More than 10 times
Almost every month
Q18. Do you call your doctor/nurse/physician assistant/medical assistant to discuss medical problems over telephone?
Yes
No
Q19. If you answered “yes” to above question, what kind of medical problems have you discussed over telephone?
Minor illness
General medical advice
Skin rashes
Follow up for chronic conditions
Prescription questions or renewals
Mental-health issues
Emergencies
Others
Q20. If you answered “other” to the last question what other kind of medical problems not already listed have you discussed over the telephone (please briefly describe)?
__________________________________________
Q21. Would you prefer video calling to talking to your doctor over telephone?
Yes
No
Q22. If you answered yes, how often would you prefer to use video communication over telephone?
All the time
Sometimes
Q23. If you answered “yes” to preferring video calls to telephone calls, what do you think are the advantages of using video communication instead of telephone (mark all that apply)?
Would save time in general
Would save travel time
Would save travel cost
Could stay home when feeling ill
Faster contact with primary care provider than waiting for an appointment
Wouldn't need to take off from work
Other
Q24. If you answered other to the above question, please specify.
__________________________________________
__________________________________________
Q25. What specific concerns would you have for using video communication?
I prefer face to face interaction with my primary care provider
I don't know how to use the devices or technology
Video calling is less personal
Video calling is not private enough
Video calling may not allow proper diagnosis
Other
Q26. If you answered “other” to the above question, please specify.
__________________________________________
__________________________________________
Q27. What medical conditions do you think are not suitable for discussion over video communication?
If a physical examination is required
Complex or serious illness
Sensitive or personal problems
Emergencies
Mental health concerns
Other
Q28. If you answered “other” to the above question, please specify.
__________________________________________
__________________________________________
Thank you for participating!!!
Notes
This article was externally peer reviewed.
Conflict of interest: RDB has received honoraria for board review lectures with the American College of Preventive Medicine. JS and SM have no conflicts of interest.
Funding: None.
To see this article online, please go to: http://jabfm.org/content/33/5/765.full.
- Received for publication October 9, 2019.
- Revision received April 24, 2020.
- Accepted for publication April 26, 2020.





{kind=link}
{kind=link}
{kind=link}