
Abstract
Using data from 2016 to 2018, we demonstrate a sharp increase in graduating family medicine residents and early-career family physicians who intend to or actually prescribe buprenorphine with no change in mid-to-late-career physicians. Family physicians are responding to the opioid crisis but, growing the family medicine workforce to treat opioid-use disorder will require a larger response from mid-to-late-career physicians.
Deaths attributed to drug overdoses have increased in the United States from 16,651 in 2010 to 70,237 in 2017, with two thirds of these being from opioids.1,2 Despite increasing need, only 35% of those needing treatment for a opioid-use disorder (OUD) received treatment in 2015 to 2017.3 In late 2015, only 31% of family medicine (FM) residencies reported having a recent graduate obtain a buprenorphine waiver in the prior year4 and only 7% of 2013 FM residency graduates were prescribing buprenorphine.5 Given the increased need for treatment of OUD, our objective was to determine the proportion of family physicians (FPs) who prescribe, or intend to prescribe buprenorphine, at various stages in their careers.
We used data from the 2017 and 2018 American Board of Family Medicine (ABFM) Family Medicine Certification Examination registration questionnaires6 and the 2016 through 2018 Family Medicine National Graduate Survey.7 The examination registration questionnaires are completed 3 to 4 months before examination date and are a required component of registration.6 We used data from both residents signing up for their initial certification examination and from FPs seeking to continue their certification, usually a minimum of 7 to 10 years after residency graduation. The graduate survey is administered to ABFM diplomates 3 years after residency training. The following groups were asked whether they prescribed buprenorphine: all respondents to the graduate survey (“early career”) all graduating residents when registering for their initial ABFM certification examination (“certification”), and a 20% sample of practicing FPs (“mid to late career”). Certification candidates were asked about intentions to prescribe, as opposed to actual prescribing. We summarized the proportion in each cohort by year. The American Academy of Family Physicians Institutional Review Board approved this study.
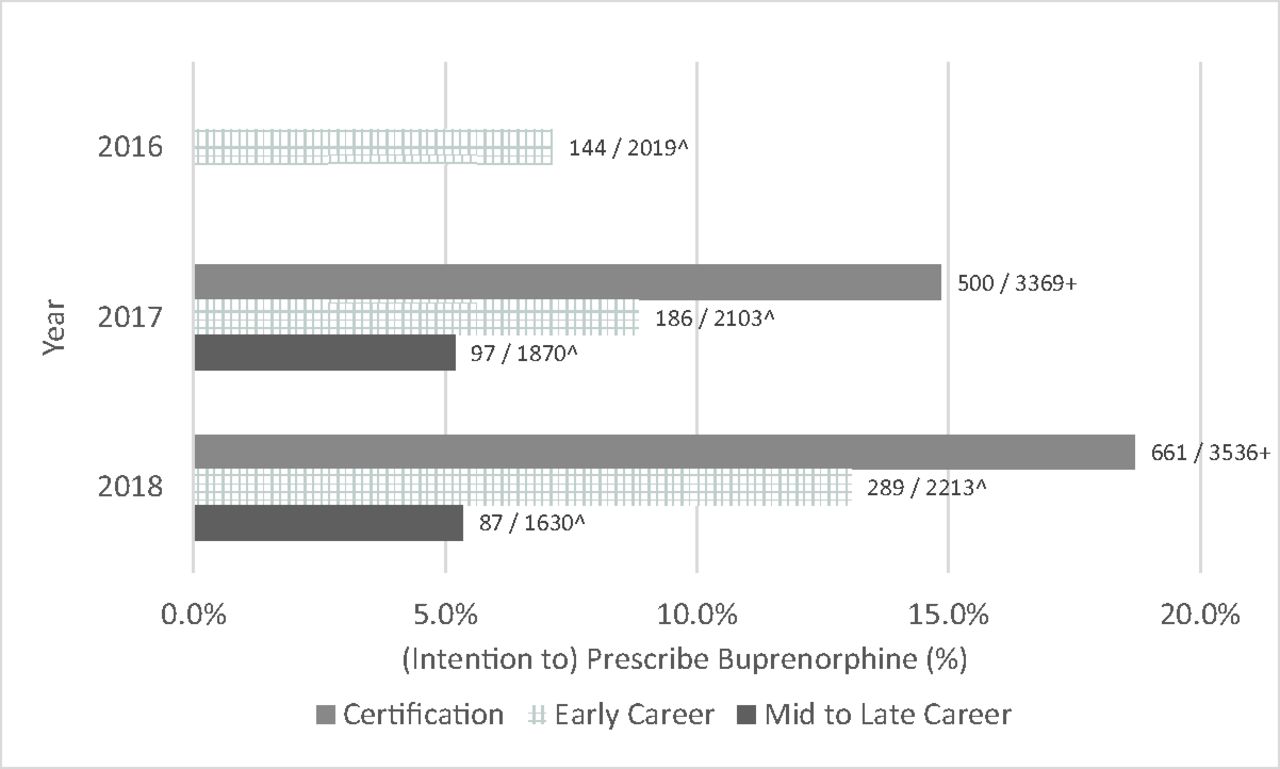
The response rates varied from 67% to 100%. A total of 16,740 FPs data were included: 1630 to 3536 in each cohort (Figure 1). Certification candidates' intentions to prescribe buprenorphine increased from 14.8% to 18.7% from 2017 to 2018. The proportion prescribing buprenorphine increased among early-career FPs from 7.1% to 13.1% from 2016 to 2018, while mid-to-late-career FPs prescribing rates were flat at just over 5%.
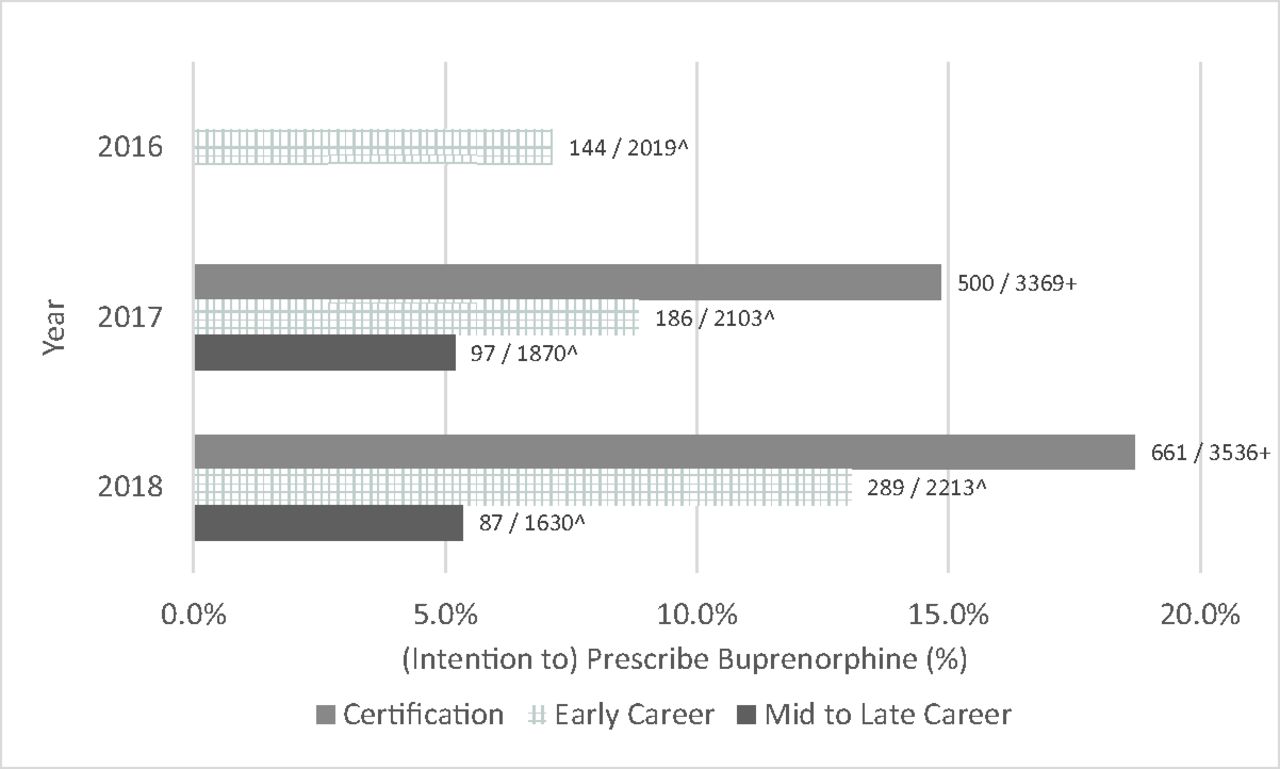
Family physician Buprenorphine prescribing and intention to prescribe, 2016–2018 (n = 16,740). + Family Physicians at residency graduation (Certification) were asked about intention to prescribe. ∧Family physicians 3 Years out of residency (Early Career) and practicing Family physicians at least 7–10 years out of residency (Mid to Late Career) were asked about whether they prescribed Buprenorphine. Numbers at end of each bar signify the actual number prescribing or intending to prescribe over the denominator in each cohort.
We found large increases in both intention and actual prescribing of buprenorphine by early-career FPs, but flat rates among mid-to-late-career FPs. Our results suggest that residency programs are likely responding to the opioid crisis by preparing FPs to treat OUD. This is supported by past work that found only 10% of 2013 FM residency graduates were prepared to prescribe buprenorphine (the 2016 early career FPs in this study) with preparation being the largest predictor of prescribing.4 The increasing intentions of graduating residents likely reflects curricular shifts, 30% of residencies had an addiction medicine curriculum in 2015,4 toward training FPs to treat OUD, and hopefully substance-use disorder as well. With training rooted in the biopsychosocial model, and a large presence in rural areas, FPs are essential to treating the opioid epidemic and all residencies should produce graduates who can treat OUD. Additional support for later career FPs to add OUD treatment to their practice are needed as early-career FPs will not be sufficient to meet patient demand. Figure 1.
Notes
This article was externally peer reviewed.
Funding: LEP and ZJM were supported by the Federal Office of Rural Health Policy (FORHP), Health Resources and Services Administration (HRSA), U.S. Department of Health and Human Services (HHS) under cooperative agreement # U1CRH30041. The information, conclusions and opinions expressed in this paper are those of the authors and no endorsement by FORHP, HRSA, HHS, or the University of Kentucky is intended or should be inferred.
Conflict of interest: LEP, ZJM, and ARE are employees of the American Board of Family Medicine.
See Related Article on Page 4.
To see this article online, please go to: http://jabfm.org/content/33/1/7.full.
- Received for publication June 26, 2019.
- Revision received August 27, 2019.
- Accepted for publication August 28, 2019.





{kind=link}