
Abstract
Background: Advanced primary care models emphasize patient-centered care, including self-management support (SMS). This study aimed to promote the translation of SMS into primary care practices and reported on key baseline practice characteristics that may impact SMS implementation.
Methods: Thirty-six practices in Colorado and California participated in the study from December 2013 to March 2017. Practice administrators completed a Practice Information Form describing practice characteristics. Clinicians and staff (n = 716) completed the Practice Culture Assessment and the Patient-Centered Medical Home (PCMH) Monitor. Descriptive statistics were computed to determine practice characteristics related to culture, quality improvement, level of PCMH, and SMS implementation. Field notes and key informant interviews provided contextual details about practices. Iterative qualitative analyses identified important facilitators and barriers and change capabilities around SMS implementation.
Results: In bivariate analyses, rural locations, fewer uncontrolled patients with diabetes, higher Medicaid or uninsured populations, underserved designation, and higher level of “PCMHness” were associated with greater reported implementation of patient SMS (all P < .05) at baseline. In the final multilevel model, specialty (FM vs mixed, P = .0081), rural location (P = .0109), and higher percent Medicaid (P < .0001) were associated with greater SMS. Practices described key facilitators (alignment, motivation, a visible champion, supporting infrastructure, and functional quality improvement and care teams) and barriers (no shared vision, no visible champion, siloed infrastructure, competing programs, turnover, and time constraints) to improving SMS delivery.
Conclusions: Careful attention—and action—on key practice characteristics and context may create more favorable initial conditions for practice change efforts to improve SMS in primary care practices.
- California
- Chronic Disease
- Colorado
- Counseling
- Disease Management
- Information Technology
- Life Style
- Obesity
- Patient Care Team
- Patient-Centered Care
- Primary Health Care
- Quality Improvement
- Self Care
- Type 2 Diabetes Mellitus
Most patients with type 2 diabetes mellitus (T2DM) in the United States receive diabetes care in primary care settings, which are undergoing rapid transformations due to the need to improve quality and decrease costs. The Patient-Centered Medical Home (PCMH) and the Chronic Care Model are complementary clinical intervention frameworks that are commonly used to support better T2DM outcomes in primary care.1⇓⇓⇓⇓⇓–7 Self-management support (SMS) is a core component of both the PCMH and Chronic Care Model, and focuses on providing patients with the necessary tools and resources so that they can better manage their illness, in particular by adopting and implementing healthy behaviors that promote optimal clinical outcomes.6,8⇓–10 SMS for diabetes typically targets improvements in medication adherence, diet, exercise, and other risk-related behaviors, all which are crucial for maintaining good glycemic control and reducing the risks of diabetes-related complications. Despite its recognized importance and success in clinical trials, SMS programs for diabetes continue to demonstrate limited adoptability and sustainability in the real world of primary care.11,12 Primary care clinicians have been unable to comprehensively and consistently address diabetes self-management within an efficient and systematic SMS framework for several interrelated reasons: they are often overwhelmed by competing demands, are poorly trained in assessing and intervening with health behavior change, lack practice systems for implementing change and quality improvement, and receive inadequate reimbursement for time spent in SMS activities.13⇓⇓–16
Few tools are available to assist practices with SMS. Interactive behavior-change technology (IBCT) can facilitate the adoption of crucial SMS interventions in primary care for patients with diabetes and related health risk behaviors.17⇓⇓–20. Compared with traditional, unstructured programs, technological options for delivery have the advantage of increased convenience and accessibility and may provide individualized support and resources necessary for initiating and maintaining healthful lifestyles, especially when they include nonautomated options to address patient preference and permit patient tailoring.19⇓⇓–22 There is strong evidence that Internet-based programs can effectively promote health behaviors to support diabetes self-management,23 such as healthful eating/weight management,24⇓⇓–27 increasing physical activity,28⇓–30 reducing depression symptoms, and smoking cessation.31,32 Multiple randomized trials have been conducted using IBCT programs for diabetes self-management with positive results.33,34
Connection to Health (CTH) is a comprehensive, evidence-based SMS program that supports behavior change through IBCT. The CTH logic model is informed by social-cognitive35⇓–37 and social-ecological38⇓–40 theories and is inclusive of the evidence based principles for implementing SMS in primary care.41 Multiple intervention components work together to promote enhanced, tailored diabetes management, which is linked to positive health outcomes.42⇓⇓–45
The simple availability of effective IBCT tools such as CTH does not assure their successful implementation.15,16,46⇓–48 Primary care practices are experiencing multiple pressures to see a large number of patients, to provide improved care, and to do so with very constrained reimbursement. Practices have few mechanisms to integrate new programs into routine care, which can exert major pressures on practice operations—even small changes can have substantial consequences that limit their effectiveness and sustainability.15,16,46⇓–48 Adoption and implementation of new care programs vary across practices based on practice characteristics, including practice culture and change capacity, practice size, location (rural vs urban), previous change experience, and decision-making style.13,14,46
This study was designed to promote the translation of SMS into primary care practices for patients with T2DM by combining 2 promising lines of research; specifically, testing the effectiveness of CTH for patients with T2DM in diverse primary care practices and evaluating the impact of practice facilitation to enhance uptake and maintenance of the intervention over time. This article reports on the baseline quantitative and qualitative results, which address this specific aim: to identify key practice characteristics (eg, practice size, organization, setting, and level of experience with practice redesign efforts) that affect CTH implementation and outcomes. The 2 other specific aims of this study, which will be reported on in another manuscript, are (1) to conduct a cluster randomized trial to examine the reach, effectiveness, adoption, implementation, and maintenance of CTH for patients with T2DM in primary care practices; and (2) to determine the incremental benefit of brief, targeted practice facilitation on the implementation of CTH in diverse primary care practices.49
Methods and Design
Design
CTH is a 3-arm, cluster-randomized trial to evaluate the reach, effectiveness, adoption, implementation, and maintenance of CTH for patients with T2DM in diverse primary care practices. This report is focused on postrandomization practice and practice member surveys and key informant interviews collected at baseline, before any intervention implementation.
Practice Sample
We recruited 36 primary care practices, 18 each in Colorado and California. Practices were recruited through the Colorado and California practice-based research networks, informational articles in the Colorado Academy of Family Physicians quarterly newsletter, and direct investigator contacts with health systems and individual practices. Inclusion criteria were family medicine or general internal medicine practices with a minimum of 80 patients with T2DM, with all clinicians agreeing to participate. Practices were selected to participate if they met these criteria. We recruited a diverse set of practices of various sizes and organizational structures (such as private, system-owned, and safety-net practices). Detailed information about practice recruitment was published in a previous manuscript.50 Practices participated for 18 months, with participation encompassing December 2013 to March 2017.
Protections
This project was reviewed and approved by the Colorado Multiple Institutional Review Board and the University of California San Francisco Institutional Review Board.
Practice Participants
All practice staff and clinicians were asked to complete the baseline surveys, resulting in 716 completed surveys from all 36 practices. In addition, 3 to 6 staff and clinicians per practice participated in key informant interviews. Interviewees were selected to represent a mixture of roles in the practice (ie, clinical and practice leadership, nursing, front and back office staff, and health educators) to ensure capture of the breadth of experience related to SMS.
Measures
Practice Surveys
Clinicians and staff completed 2 surveys to determine baseline practice characteristics related to culture, quality improvement, PCMH-ness, and SMS implementation:
The SMS subscale of the Practice Monitor provided information about clinician and staffs' routine use of SMS as a component of patient care. Practice members rated their perceptions of SMS activities and practice culture using a Likert scale (strongly disagree to strongly agree) on 28 items. Prior validation and factor analysis yielded 7 reliable subscales used in our analysis; this survey can be found in Appendix A online.
The Practice Culture Assessment (PCA) provided practice-wide information about practice culture related to practice change and improvement.50 The PCA was completed by practice clinicians and staff using a 5-point Likert-type scale (strongly disagree to strongly agree) on 22 items. Before validation and factor analysis yielded 3 reliable subscales used in our analysis: improvement and Change Culture, Work Relationships, and Chaos.51
In addition, practice administrators completed a Practice Information Form, a 16-item form that describes main practice characteristics and descriptions of their patient population.
Survey Data and Statistical Analysis
Surveys were administered from introduction through the first SMS training session. Practice staff and clinicians completed the survey either via article copy or through an email link to Research Electronic Data Capture, which is a secure, web-based application designed to support data capture for research studies.52 Surveys were anonymous, and no individual information was obtained or shared with other staff.
Practice characteristics were collected during the practice recruitment process. Practice characteristic data collected were level of quality improvement experience, level of PCMH implementation, number of clinicians, specialty type, percent of patients with diabetes, percentage of patients with hemoglobin A1c >9, location (rural/urban), type of practice organization, and percentage of Medicaid or uninsured patients.
Survey Data Analysis
Descriptive statistics were computed for baseline practice characteristics and key variables of interest from the practice member surveys. Exploratory factor analysis and item analysis were performed for items the SMS scale from the Practice Monitor survey, because this specific combination of items had not been previously used as a scale. The outcome variable for all subsequent analyses was the patient SMS scale. Independent variables of interest included items from the practice survey, listed above, and scores on the PCA subscales Change Culture, Chaos, and Work Culture. Each independent variable was assessed for possible association with the outcome in bivariate analyses (Pearson correlation coefficient); practice characteristic variables that were associated with the outcome at P < .10 in simple bivariate associations were considered for further analysis; PCA subscales were considered for further analysis regardless of strength of bivariate associations. Next, general linear mixed models (with random intercept for practice) were used to further examine associations between the outcome and each practice-level variable, 1 at a time. Practice-level variables that were significantly associated with the outcome (P < .05) after adjusting for clustering were included in an initial multivariable model, eliminating nonsignificant variables 1 at a time until all P values were less than 0.05. Finally, practice culture variables were added to the models. Because of collinearity, Change Culture and Work Culture were assessed in separate models. All statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC).
Qualitative Data
Baseline qualitative data included (1) structured field notes completed by the facilitator and/or research staff after each substantive contact with the practice (from introduction through the first SMS training session) and (2) semistructured interviews conducted with staff and clinicians in each practice (before or immediately after the first SMS training session). Memo forms providing brief summary notes by the interviewer were also completed after each interview.53 Over 250 documents were included in this analysis.
Qualitative Data Analysis
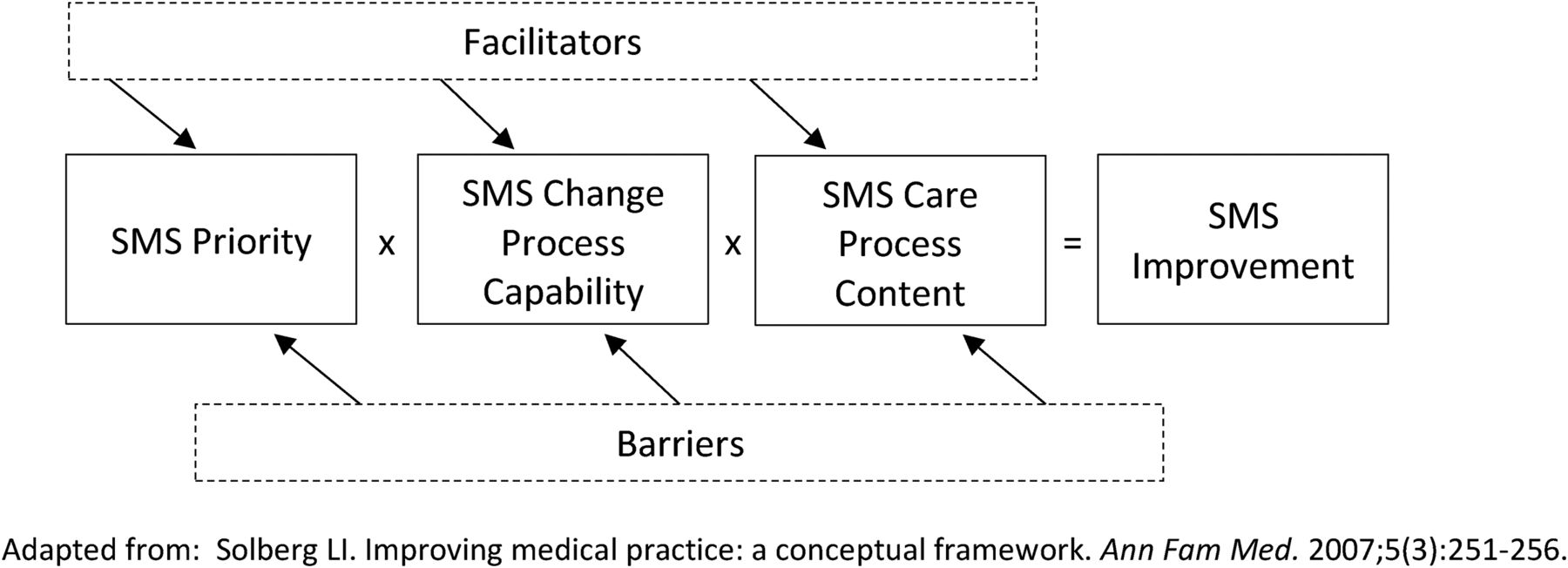
Four qualitative analysts followed an iterative approach to the qualitative analysis, with the investigators going through cycles of reading, summarizing, and rereading the data.54 Beginning with immersion in the data (each analyst reviewed data from a selection of practices in each Colorado and California and in each arm) to read, review, and reread, and then to the development of conceptual categories relevant to the implementation of CTH or SMS. Fourteen provisional conceptual categories emerged, which were then used for template coding to begin segmenting relevant data for further review and analysis. After a review of coded data to assure conceptual inter-rater reliability, the analysts divided the data and coded it using the qualitative software program ATLAS.ti (version 7, Scientific Software Development, GmbH). The analysts continued to meet and discuss the data over a series of twice-monthly meetings over 6 months. Reading, refining, discussing, and summarizing continued until key themes emerged and clarity by practice for each theme was evident. The coded data were then summarized into a matrix, with key practice characteristics organized into the Solberg framework for practice improvement (see Figure 1). Finally, the analysts developed practice characteristic constructs as forces that potentially propel or repel the implementation of SMS in these practices.

Framework for self-management support (SMS) practice improvement. Adapted from: Solberg LI. Improving medical practice: a conceptual framework. Ann Fam Med 2007;5:251–256.
Results
Practice Survey Results
A total of 716 clinicians and staff enrolled in CTH completed baseline surveys (73% response rate). Practice characteristics are shown in Table 1. The majority of the practices enrolled in CTH were Federally Qualified Health Centers, and as such, the percentage of patients with Medicaid or uninsured is higher than in the general population.
Baseline Practice Characteristics from 36 Primary Care Practices in Colorado and Northern California; Data Collected from 12/2013 to 9/2015
Overall scores on practice member surveys for patient SMS activities and practice culture are shown in Table 2. Patient SMS Cronbach's α = 0.92. The overall score for patient self-management was 65.7 out of 100, and individual SMS items showed slightly higher implementation of specific SMS activities, such as systems implemented for identifying patients with needs for SMS, use of shared care plans, SMS tools provided to patients and families, and the presence of a care manager or staff member to assist with SMS activities.
Baseline Practice Member Surveys from 36 Primary Care Practices in Colorado and Northern California; Data Collected from 12/2013 to 9/2015
Simple bivariate associations for variables that met initial screening criteria are shown in Table 3. After adjusting for clustering, the following variables were associated with a greater reported implementation of patient SMS (all P < .05; please see Table 2 for specific SMS items): rural location, higher percent Medicaid or uninsured populations, underserved designation, presence of a care manager, and a higher level of “PCMHness” (see Table 2). In the multivariable model with SMS implementation as the outcome and all practice level variables from the previous step included initially as independent variables, presence of a care manager (P = .0019), level of “PCMHness” (P = .0027), and underserved designation (P = .0272) were retained at P < .05. Because of high collinearity between PCA subscales Change Culture and Work Culture, these were included in separate models. After adjusting for significant practice level variables, higher scores on the Change Culture (P < .0001) and Work Culture (P = .0030) subscales were associated with greater SMS. Higher scores on the Chaos (P = .0020) subscale was associated with lower scores on SMS implementation.
Baseline Practice and Practice Member Variables Associated with Greater Self-Management Support Activities, from 36 Primary Care Practices in Colorado and Northern California; Data Collected from 12/2013 to 9/2015
Qualitative Results
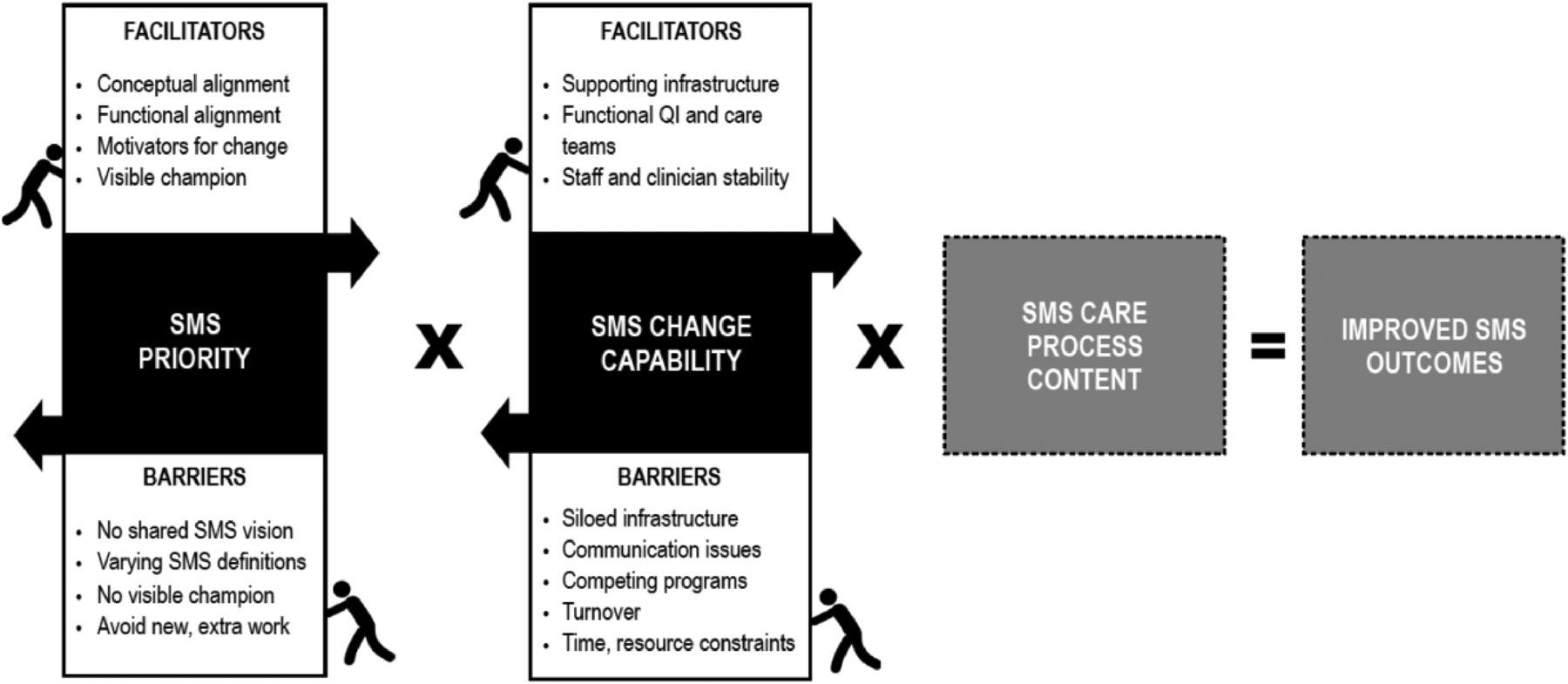
Across all 36 practices, 119 baseline key informant interviews were completed (42 providers; 77 staff or administrators) and 53 field notes were filed covering the baseline period. Delivering SMS likely requires multiple people in a clinic having active and integrated roles in delivering key components of SMS to patients. Leif Solberg's work on practice improvement provided an organizing framework to describe initial conditions that could potentially promote or hinder the changes needed to effectively deliver SMS for patients with diabetes (Figure 2). The baseline analysis focused on Priority and Change Process Capability to elaborate details in the “black box” of these areas. It also provided a conceptual framework to organize analytic conceptual constructs over time. From the analysis of baseline data, practice priorities were identified and change process capabilities that could affect SMS implementation in these 36 practices (Figure 2).

Facilitators and barriers for self-management support (SMS) implementation.
Priority: Alignment Around SMS Transformation
At baseline, across all 36 practices, there were clinical leaders, staff, and clinicians who expressed SMS transformation as an important priority; however, other practice staff and clinicians expressed simultaneous concerns and reservations about practice changes for SMS. Propelling and repelling factors pushing for SMS transformation are described in Table 4.
Priority Alignment Around Self-Management Support (SMS) Transformation
Change Process Capability to Implement SMS Changes
The details of change process capability varied widely across the 36 practices; however, there were consistent concepts that emerged about characteristics that propel implementation—supporting infrastructure, functional teams, and practice stability—and those that repel implementation—siloed infrastructure, communication issues, turnover, competing programs, and time/resource constraints. Propelling and repelling factors for change process capabilities are described in Table 5.
Change Process Capability to Implement Self-Management Support (SMS) Changes
Discussion
The purpose of this article was to report on baseline practice characteristics and context from surveys and qualitative interviews that reflect previous implementation of SMS activities before participation in this study. SMS is a critical element of care for people with diabetes and other chronic conditions, and the current findings may assist primary care practices and researchers with identifying key practice characteristics that are necessary to provide SMS for patients with T2DM.
At baseline, the practices reporting higher levels of SMS reported significantly higher levels of a positive work culture, the presence of a care manager, higher levels of “PCMHness,” and lower levels of practice Chaos. These characteristics are known to cluster and are often seen together, as have been reported in other studies.48,53 For example, the Enhancing Practice, Improving Care study found that practice facilitation using a continuous quality improvement approach was effective at improving measures of diabetes care.51 Likewise, Shetty et al55 examined the components of organizational support for SMS in primary care practices. These researchers found 8 essential elements of organizational support, including ongoing quality improvement, staff training and education, and integration of SMS into primary care.
Results from the qualitative data also support the findings from the practice surveys regarding level of “PCMH-ness” and the importance of the presence of a care manager. SMS implementation facilitators included several key components of the PCMH,1 including functional quality-improvement teams; coordinated care with the presence of supporting infrastructure such as care managers, patient health educators, or Certified Diabetes Educators; and practice leadership who saw alignment with SMS and their PCMH activities.
Leif Solberg's quality improvement framework suggests that multiple factors combine to produce improved quality. SMS is not business as usual. Results from this study suggest that SMS may require substantial redesign of workflows, responsibilities, and staffing along with careful coordination and communication across multiple roles in a practice for a sustained period. There are factors that seem to align with and promote SMS redesign (eg, conceptual and functional alignment, functional teams, and supporting infrastructure); yet, there may be specific repelling factors (eg, no visible champions, lack of consistent vision, different understandings of SMS, and siloed work) that are particularly at odds with implementing sustained and functional SMS. Addressing and minimizing the repelling forces and maximizing and building on the propelling forces across the entire practice may help to unify the practice vision and point staff and clinicians in the same direction.
These findings may be useful for health systems, practices, researchers, and others to consider in identifying practice's readiness for SMS implementation. Lehman et al55 assessed organizational readiness for change in health care and found similar results, particularly for the importance of a positive work culture to be “ready” to implement technology and organizational changes. As such, it may be useful for practices and health care organizations to assess their work culture before embarking on implementing SMS as foundational work may need to be conducted to ensure success.
Limitations
This project was only implemented in primary care practices in Colorado and California and may not be representative of primary care in other states. In addition, federally qualified health centers were overrepresented in our sample. Because this is a limited sample, other important factors may exist, but we did not observe them in our data. This report does not consider the relative influence on the observed characteristics on important, downstream practice and patient outcomes.
Conclusion
Fully implemented SMS requires robust and active participation across clinical roles in primary care practices. The results from this study add to our understanding that careful attention—and action—on work culture and transformation readiness may create more favorable initial conditions for practice change efforts to improve SMS in primary care practices. Practices, health systems, and reseachers may need to take these key practice characteristics into account when considering implementation of SMS targeted for patients with T2DM.
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: none declared.
See Related Article on Page 341.
To see this article online, please go to: http://jabfm.org/content/32/3/329.full.
- Received for publication April 23, 2018.
- Revision received December 21, 2018.
- Accepted for publication December 21, 2018.





{kind=link}
{kind=link}