
Abstract
Introduction: The majority of consultations for acute respiratory tract infections (RTIs) lead to prescriptions for antibiotics, which have limited clinical benefit. We explored patients' willingness to have blood tests as part of the diagnostic work-up for RTIs, and patient knowledge about antibiotics.
Methods: Patients at 6 family medicine clinics were surveyed. Regression modeling was used to determine independent predictors of willingness to have venous and point-of-care (POC) blood tests, and knowledge of the value of antibiotics for RTIs.
Results: Data were collected from 737 respondents (response rate 83.8%), of whom 65.7% were women, 60.1% were white, and 25.1% were current smokers; patients' mean age was 46.9 years. Sex (female), race (white), and a preference to avoid antibiotics were independent predictors of greater level of antibiotic knowledge. A total of 63.1% were willing to have a venous draw and 79% a POC blood test, to help guide antibiotic decision-making. Non-American Indian/Alaskan Native race, current smoking, and greater knowledge of antibiotics were independent predictors of willingness to have a POC test.
Conclusion: A large majority of patients seemed willing to have POC tests to facilitate antibiotic prescribing decisions for RTIs. Poor knowledge about antibiotics suggests better education regarding antibiotic use might influence patient attitudes towards use of antibiotics for RTIs.
- Antibacterial Agents
- Decision Making
- Family Physicians
- Hematologic Tests
- Patient Preference
- Prescriptions
- Point-of-Care Systems
- Practice-based Research
- Referral and Consultation
- Respiratory Tract Infections
Acute respiratory tract infections (RTIs) are among the most common reasons adults and children present to family medicine clinics.1,2 Patients' consultation decisions are driven by a variety of factors during RTI episodes, including perceived severity of illness, desire for symptomatic relief, and concerns about complications.3⇓–5 Despite evidence that antibiotics confer little benefit for most RTIs, the majority of patients presenting with RTIs are inappropriately prescribed broad-spectrum antibiotics.6⇓⇓–9 Diagnostic uncertainty, patient demand, and perceived patient expectations for antibiotics have been identified as key factors that influence antibiotic prescribing decisions.4,10,11
A variety of strategies have been introduced in attempts to safely reduce antibiotic prescribing. Some have been directed toward patients in order to change their knowledge and beliefs about antibiotics, such as education campaigns from the Centers for Disease Control and Prevention, whereas other initiatives have been directed toward clinicians, such as delayed prescribing, clinical prediction rules to help identify patients at risk of complications, and point-of-care (POC) diagnostic tests to enhance diagnostic certainty.12⇓–14 Despite some success with these strategies, lack of confidence differentiating bacterial infections that may benefit from antibiotics from self-limiting viral RTIs remains an impediment to further reductions in antibiotic prescribing by clinicians.10,11
The recently announced National Action Plan for Combating Antibiotic-Resistant Bacteria has highlighted the need for more POC testing to guide treatment decisions.15 Two main types of POC tests are available in primary care settings to improve diagnostic certainty for RTIs: tests that detect individual pathogens (eg, influenza, group A streptococcus) and tests that quantify the response to infection, such as C-reactive protein (CRP), which is an acute-phase protein synthesized by the liver more quickly during bacterial than viral infections, thus facilitating differentiation of bacterial from viral RTI etiologies.16 Strong evidence shows that POC CRP tests provide physicians with added diagnostic information that can facilitate improved targeting of antibiotics.17⇓–19 Indeed, a systematic review of 13 trials of POC CRP testing in >10,000 adults with suspected RTIs in primary care found a 25% reduction in antibiotic prescribing, with no increase in adverse events, reconsultations, or worsening of patient experience.20 Changes to the culture of antibiotic prescribing and potential introduction of new diagnostic tests requires an understanding of patients' knowledge, views, and attitudes.21,22 While primary care physicians have highlighted a need for improved diagnostic tools to help them guide antibiotic prescribing decisions, no recent attempts have been made to determine patients' willingness to avoid antibiotics for RTIs or their perceptions of these tests in the United States.23,24 The aim of this study, therefore, was to explore patients' knowledge and preferences regarding antibiotics for RTIs and their willingness to have a blood test in order to help guide antibiotic use for RTIs.
Methods
Sampling and Recruitment
Six primary care clinics from the WWAMI Region Practice and Research Network (WPRN), a practice-based research network in the region comprising the 5 states of Washington, Wyoming, Alaska, Montana, and Idaho, participated in this study. The WPRN Coordinating Center at the University of Washington facilitated identification of interested clinics. Participating clinics were located in Washington, Wyoming, and Idaho and included both locations serving rural areas and those serving large metropolitan areas; 2 sites were federally qualified health centers and 3 were hospital-associated clinics.
Adult patients (≥18 years old) presenting for any reason for a visit to a participating clinic during a 5-day period in November/December 2015 were consecutively enrolled and invited by clinic staff to complete an anonymous survey upon arrival for their office visit. The survey was available in English and Spanish. Completed surveys were deposited into a designated box in the clinic reception area. Front desk staff tracked how many surveys were handed out in order to calculate response rates, and the collection boxes were mailed to the WPRN Coordinating Center at the end of the week. The University of Washington Human Subjects Review Board approved this study.
Survey Instrument
The survey included questions about patient demographics (eg, age, gender, ethnicity, race), overall health status, type of health insurance, smoking status, number of office visits for an RTI within the previous 12 months, number of antibiotic prescriptions for an RTI issued to the patient in the previous 12 months, patient preference for antibiotic treatment for RTI, and willingness to have a POC fingerstick test and venous draw (assessed using a 5-point Likert scale). Patients were asked to indicate the 3 most important reasons that would help them decide to have a POC fingerstick test. The survey also asked patients about the types of respiratory conditions which they believed would be improved by antibiotics (ie, those caused by viruses, bacteria, or viruses and bacteria), which was used as a measure of patients' knowledge of antibiotics.25 Respondents were asked to select a single response for all items except race, type of health insurance, and the 3 most important reasons for deciding to have a POC fingerstick test. (See the Appendix for the survey instrument.)
Data Management
Survey responses were double-entered into a Research Electronic Data Capture database.26 Data sets were cross-referenced to identify discrepancies using the cf command in StataIC 14 (StataCorp LLC, College Station, TX) and were resolved by manually reviewing the relevant surveys. Age was categorized into 3 groups: <40, 40 to 59, and ≥60 years. Given the small number of respondents identifying as Asian and Pacific Islanders, these were combined. Those who selected >1 race option were assigned to a “multiple race” category. Respondents who selected multiple options for health status were assigned to the better health status (eg, if they selected both “good” and “moderate,” their health was categorized as “good”). A “multiple/other type of insurance” category was created for respondents who selected multiple types of health insurance, “other” health insurance, or who did not know their insurance type; however, those who selected both Medicare and Medicaid were combined into 1 category. Subjects who selected “private insurance” and another type of health insurance were assigned to a private insurance category, as secondary insurance is often supplementary. Respondents who selected multiple options to the question about antibiotic knowledge were assigned to a “do not know” category. Patients selecting multiple options regarding their willingness to have blood drawn from their arm or willingness to have a POC fingerstick test were assigned the category closer to neutral (eg, if they selected both “very unwilling” and “somewhat unwilling,” they were assigned to the “somewhat unwilling” category). Responses were then transformed into a binary variable of “somewhat willing or very willing” and “neutral, somewhat unwilling, or very unwilling.”
Data Analysis
Survey response rates were estimated by counting the numbers of surveys issued at each site and the number of nonblank surveys returned. Descriptive statistics were used to describe respondents' characteristics (age, gender, ethnicity, race, insurance status, smoking status, and overall health status) and antibiotic prescriptions used by them in the previous 12 months, preferences for antibiotics, knowledge of antibiotics, willingness to have blood drawn from the arm, willingness to have a fingerstick blood test, and the most important reasons for deciding to have a POC fingerstick test.
We explored associations between potential predictor variables (eg, patient demographics, number of prior visits for an RTI) and the outcome of knowledge of antibiotics using the Pearson χ2 test. We used the same methods to predict the outcome of willingness to have a POC fingerstick test, using knowledge of antibiotics as an additional predictor variable. Backward stepwise logistic modeling was used to identify significant predictors of knowledge of antibiotics and of willingness to have a POC fingerstick test. Demographic characteristics, doctor visits for an RTI, preferences for antibiotics, knowledge of antibiotics, and willingness to have blood drawn from the arm were considered independent predictor variables, and dummy variables were created for categorical variables such as health status or race. Several regression models were used to explore determinants of knowledge of antibiotics and willingness to have a POC fingerstick test. The final adjusted models include predictor variables that were identified after examining the strength and significance of the association between predictor variables and outcomes.
Results
A total of 743 patients returned completed surveys, of which 6 were excluded because they were filled out on behalf of children. The final sample comprised 737 surveys, with an overall response rate of 83.8% (range, 64.7–99.0%). A total of 707 patients (95.7%) completed the survey in English.
Respondent Characteristics
Respondents had a mean age of 46.9 years (range, 18–93 years), and most (65.7%) were female. The most frequent race and ethnicities selected were white (60.1%), Hispanic/Latino (14.0%), and black or African American (10.7%) (Table 1). Among respondents, 74% considered their health to be moderate, good, or excellent. Approximately half (51.9%) reported they were nonsmokers, whereas 25.1% were current smokers. Fifty percent reported having Medicare and/or Medicaid insurance, 25.3% had only private health insurance, and 10.4% had no health insurance. The majority of respondents (66.1%) indicated they had no doctor visits for RTI in the previous 12 months; 14.6% had 1 visit and 19.3% had ≥2 visits (Table 2). A total of 36% reported they had not been prescribed antibiotics for an RTI in the past 12 months, 35.5% indicated they had been given antibiotics once, and 28.5%, twice or more.
Characteristics of Respondents
Experience with Respiratory Tract Infections, Preference for and Knowledge about Antibiotics, and Willingness to Have Blood Tests
Preference for and Knowledge of Antibiotics for Treating RTIs
The majority of respondents (87.3%) stated they preferred to avoid taking antibiotics unless their doctor believed the drugs would help their cough or cold. Responses to the question relating to patient knowledge about the etiology of RTIs for which antibiotics may be effective showed that only 37.9% understood that antibiotics offer most benefit for bacterial infections, whereas 9.6% believed antibiotics to be effective for viral infections, 25.1% selected the option viral and bacterial infections, and 27.4% did not know (Table 2).
Respondents who correctly agreed with the statement, “I understand that antibiotics are best for treating coughs and colds that are caused by bacteria,” were more likely to be younger, white, female, and non-Hispanic and to prefer to avoid taking antibiotics (Table 3). Regression modeling showed that age group, race, ethnicity, preference for antibiotics, and type of health insurance were independent predictors of knowledge of antibiotics (Table 4). White respondents were significantly more likely to have correct knowledge of antibiotics than those of any other race, and women were 2 times more likely than men to have correct knowledge of antibiotics. In addition, those who preferred not to take antibiotics were 3 times more likely to have correct knowledge of antibiotics than those who preferred to take antibiotics.
Associations between Demographics, Health Status and Attitudes, and Willingness to Have Fingerstick Blood Test and Antibiotic Knowledge
Crude and Adjusted Odds Ratios of Willingness to Have a Fingerstick Test and Antibiotic Knowledge
Willingness to Have Blood Tests to Guide Antibiotic Use for RTIs
Nearly two thirds (63.1%) of respondents were somewhat or very willing to have blood drawn from their arm, and 79.0% were somewhat or very willing to have a POC fingerstick test to determine whether they needed to take antibiotics for an RTI (Table 2).
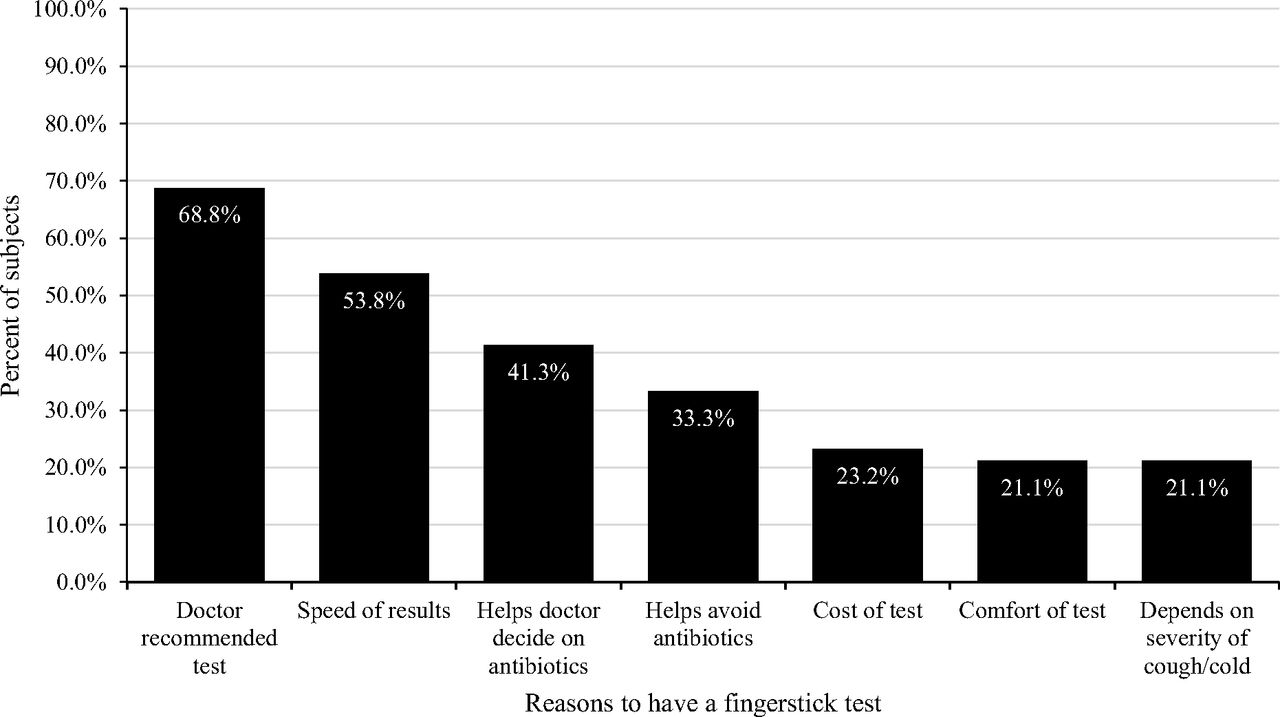
A total of 664 respondents gave 1757 reasons why they would be willing to have a fingerstick test (respondents were allowed to select up to 3 reasons). The 3 most frequently cited reasons were if their doctor recommended the test (68.8% of responses), speed of the results (53.8%), and if it helped the doctor decide whether antibiotics were needed (41.3%) (Figure 1).

Most frequent reasons cited by respondents for deciding to have a fingerstick test to help guide antibiotic use.
Willingness to have a fingerstick test to help guide antibiotic use was significantly associated with respondents who were white, considered themselves to be in good health, and were covered by private health insurance. Willingness was also significantly associated with correct knowledge of antibiotics, preference to avoid antibiotics, and willingness to have blood drawn from their arm (Table 3). By contrast, respondents who were unwilling or neutral about having a fingerstick test were more likely to identify as American Indian/Alaskan Native, to have multiple/other health insurance, and to not have visited their doctor for a cough or cold in the past year.
Regression modeling (Table 4) showed that race, smoking status (current smoker), knowledge of antibiotics (higher level of knowledge), and willingness to have blood drawn from the arm were independent predictors of willingness to have a fingerstick test. Those who identified as American Indian/Alaskan Native only were significantly less willing to have a fingerstick test than those who identified as white only.
Discussion
Key Findings
Our results provide new information about patients' preferences and knowledge about antibiotics and their willingness to consider having blood tests to support antibiotic prescribing decisions for RTIs. Nearly 9 of 10 patients (87.3%) in family medicine clinics stated they preferred to avoid taking antibiotics for RTIs, yet two thirds (64%) of those who had visited a doctor for an RTI in the past year had received antibiotics. Patient knowledge about the value of antibiotics for RTIs was somewhat limited: two-thirds did not understand that antibiotics are most effective against bacterial etiologies.
While 63.1% of patients were willing to have a venous blood draw, a significantly higher proportion (79.0%) were willing to have a POC fingerstick test to help guide antibiotic use, suggesting that these types of tests may be acceptable to patients. Patients indicated recommendation by a doctor, speed of results, and the ability of the test to help doctors' decision making were key factors guiding their potential willingness to have such tests. Our results also suggest important disparities related to gender, race, ethnicity, and age in terms of both knowledge about antibiotics for RTIs and willingness to consider blood tests for this condition, which may reflect underlying levels of education, access to care, and prior health care experiences.
Strengths and Limitations
This survey provides new information on patients' knowledge of antibiotics and preferences for treatment for RTIs, and to our knowledge it is the first survey to also provide information about US patients' willingness to consider blood tests in order to inform physicians' decisions regarding prescribing antibiotics for RTIs. Our sample was obtained from several different clinics, shows a very high response rate, and represents several ethnic and racial groups. The favorable responses toward blood tests suggests that introducing POC tests such as CRP into family medicine might be acceptable to patients. Our findings highlight persisting gaps in patient understanding regarding appropriate antibiotic use, despite antibiotic stewardship campaigns such as Get Smart About Antibiotics, targeted toward public education. Yet, paradoxically, the majority of patients in our sample wanted to avoid antibiotics for RTIs, implying that the overarching message of these campaigns may be permeating, but the underpinning rationale may need to be reframed in order to be better understood, and may need to be made more widely accessible.
Our study has several potential limitations. First, while we believe our sampling strategy included a representative sample of patients attending family medicine clinics in the United States, we acknowledge that the practices selected (most of which are family medicine residency training sites) are not typical of all primary care settings in the United States where patients present with RTIs (eg, urgent care and pharmacy-based clinics). Second, a preference to avoid antibiotics for RTIs could have been confounded by the fact that most of our sample had not presented for an RTI in the previous 12 months. Furthermore, we did not capture patients' reasons for presenting to the clinic at the time of the survey. Patients who have RTIs only infrequently and those presenting for a non–RTI-related medical reason may respond differently to those who are symptomatic with regard to willingness to have tests and treatment preferences. Third, because we did not collect the demographic characteristics of those patients who declined to complete/submit a survey, we are unable to determine how similar our respondents are to the total population registered with the participating clinics, and indeed against the broader US population. Finally, we did not ask patients to indicate their prior experiences with POC fingerstick tests or venous blood draws, which may influence their willingness to have these blood tests.
Comparison with the Existing Literature
Most patients who completed our survey did not adequately understand when antibiotics are indicated for RTIs, findings that are similar to those of studies of public knowledge captured a decade ago.25 The apparent desire of patients to avoid antibiotics seems contrary to studies of primary care clinicians' perceptions of continued high levels of patient demand as a major driver of inappropriate prescribing of antibiotics for RTIs.27 The diagnostic uncertainty that clinicians face in primary care when caring for patients with acute cough also suggests an appetite for additional diagnostic tools to help improve decision making.10 Our findings suggest that patients too would be keen on additional such testing.10 This echoes a multicountry study from Europe in which the majority of patients noted they would happy to have a POC test when they consulted with a physician for acute cough; their major reason was to give their clinician more information to make better decisions about their treatment.28
Implications for Clinicians, Policymakers, and Researchers
While a fairly substantial body of evidence exists on the effectiveness of CRP POC tests to safely reduce antibiotic use for RTIs in primary care—this test is now recommended in several European countries—to our knowledge no trials of this test have occurred in US primary care settings.20 Currently, none of the various POC tests for CRP are approved for use in the United States. Evidence is weaker for the effectiveness of other inflammatory markers (eg, procalcitonin or white cell counts) to guide antibiotic use in adults in primary care.16 One reason for a lack of studies of these tests in the United States could be a misperception that patients in the United States may be less willing than patients in other countries to accept such testing. Our findings suggest the opposite; the vast majority of adult patients prefer to avoid taking antibiotics for RTIs, and most would accept POC testing to guide decision making. For family physicians, our results suggest that the majority of adult patients prefer to avoid taking antibiotics for RTIs and that patients are strongly guided by what their family physician recommends in terms of the need for additional testing for RTIs. For policymakers, our findings of strong patient interest in blood tests to guide decisions around antibiotic prescribing supports the National Action Plan for Combating Antibiotic-Resistant Bacteria in primary care and ongoing initiatives such as Choosing Wisely, which have highlighted several RTIs for which antibiotics are overused.15,29 Our findings also underscore patients' need for transparency regarding the rationale behind physicians' antibiotic prescribing decisions. Specifically, the provision of clearer information to patient populations who pressure physicians to prescribe antibiotics (eg, patients without a relationship with their physician or who frequently medicalize self-limiting illnesses), as well as underserved populations and those with lower levels of education, may strengthen frontline efforts at antibiotic stewardship.22 For researchers, the results of this and other recent studies support the need for research to determine the role and effectiveness of office diagnostic tests in US primary care settings to safely reduce antibiotic use.22,23,30
Acknowledgments
The authors acknowledge the support of Dr. Rex Force and of the clinic staff and patients who participated in this study.
Appendix

Notes
This article was externally peer reviewed.
Funding: This project was funded by an unrestricted grant from Alere. The WPRN is supported by the National Center for Advancing Translational Sciences (NCATS) of the National Institutes of Health (NIH) under award UL1TR000423.
Conflict of interest: MT has received funding from the National Science Foundation to develop point-of-care tests for group A streptococcus and chlamydia trachomatis, and has acted as a consultant to Roche Molecular Diagnostics. No other conflicts of interest have been reported.
Disclaimer: The content is solely the responsibility of the authors and does not necessarily represent the official views of the funders of this study nor of the National Institutes of Health.
To see this article online, please go to: http://jabfm.org/content/30/5/645.full.
- Received for publication February 28, 2017.
- Revision received May 1, 2017.
- Accepted for publication May 2, 2017.





{kind=link}