
Abstract
Direct primary care (DPC) is an emerging practice alternative that (1) eliminates traditional third-party fee-for-service billing and (2) charges patients a periodic fee for primary care services. We describe the DPC model by identifying DPC practices across the United States; distinguish it from other practice arrangements, such as the “concierge” practice; and describe the model's pricing using data compiled from existing DPC practices across the United States. Lower price points and a broad distribution of DPC practices were confirmed, but data about quality are lacking.
- Fees and Charges
- Primary Health Care
- Health Care Costs
- Health Services Accessibility, Patient-Centered Care
Direct primary care (DPC) is a growing model used by family physicians and other primary care specialties aimed at delivering quality care at an affordable price. The model emphasizes ongoing and preventive care services, and third-party fee-for-service payments are abandoned. Instead, a periodic (usually monthly) fee is paid to the DPC physician to better reflect the ongoing patient relationship. The affordability of the monthly fee and the high patient and physician satisfaction have garnered national media attention from many news sources including Time,1 Forbes,2 the New York Times,3 and The Hill.4 This article clarifies terminology in part by analyzing practice self-descriptions, describes Medicare “opt out” and “split” practice data, provides an overview of the periodic fees practices have made publicly available on their websites, and presents other raw practice data in an effort to offer a national snapshot of the growing DPC movement.
DPC Terminology and Background
For the purposes of inclusion in our study, a DPC practice must be a primary care practice that (1) charges a periodic fee for services, (2) does not bill any third parties on a fee-for-service basis, and (3) any per-visit charges are less than the monthly equivalent of the periodic fee.5 This definition represents a comprehensive legal interpretation of 14 state laws passed to clarify DPC “business of insurance” regulatory questions and language from the Affordable Care Act describing mechanisms for DPC practices to participate in the insurance exchanges with “wraparound” insurance products. DPC practices often are compared with other models that charge a periodic fee, most commonly the concierge model. Price differences between the models are usually acknowledged, but price is absent from any legislative or regulatory definition of DPC.
Practices' periodic fees have been described using many terms, including retainer, membership, concierge, hybrid, split, direct pay, and direct primary care. Any group that charges patients on a periodic basis might be described using 1 or more of these adjectives. The terminology continues to evolve, but direct primary care and concierge are the terms that have taken on the greatest meaning. The most well-known concierge practices, such as MDVIP or MD,2 continue to bill third parties in the traditional fee-for-service fashion in addition to the periodic fee, a method many describe as “double dipping.”6 By contrast, DPC practices rely on the periodic fee to finance the practice without any third-party fee-for-service payments. Some practices treat one cohort of patients in the DPC model and another cohort in the traditional third-party fee-for-service model; we refer to these as “split practices.” Medicare regulations prohibit physicians from charging DPC patients for covered primary care services via the DPC model, so many DPC physicians who would like to make their services available to the Medicare population decide to “opt out” of Medicare so that they may privately contract with Medicare patients.
DPC practices claim to reduce overhead by more than 40% by eliminating administrative staff resources associated with third-party billing, resulting in lower price points for patients.7 DPC physicians cite 3 key practice improvements: (1) increased availability and, therefore, access; (2) more time for each patient encounter, leading to improved quality; and (3) lower overhead costs.8 Patients may usually join without regard to their insurance or socioeconomic status since practices often “opt out” of Medicare and do not sign traditional contracts with private insurance companies or Medicaid. For non–primary care services, DPC patients rely on a variety of options, ranging from the usage of high-deductible health insurance plans or “wraparound” insurance plans designed to cover everything except primary care (as specifically authorized by the ACA; discussed below) to traditional employer-sponsored insurance, Medicare, Medicaid, or ACA-exempted “health-sharing” ministries.9 Uninsured patients who need traditionally expensive nonemergent procedures such as a colonoscopy or magnetic resonance imaging often benefit from the DPC physicians' efforts to negotiate lower “cash pay” prices on their behalf, and depending on the DPC practice, some radiologic testing might be included at no additional cost.10
Methods
A thorough literature search demonstrated a paucity of data available to describe the DPC practice model. Studies related to DPC were located using the following search terms in PubMed and Google: direct primary care, retainer medicine, membership medicine, concierge medicine, and boutique medicine. The phrase “direct primary care” yielded only 3 relevant results in PubMed. We conducted a review of information publicly available on DPC practices' websites that met our 3-part definition in an effort to describe the number of practices adopting the model, the terminology advertised (self-description), and their distribution. We gathered information about the size of practices, the providers involved, and costs to provide a broad overview of the current state of DPC in the United States.
DPC practices were identified through a review of literature, practice listings from databases in the 2 states that require DPC practice registration and publication (Washington11 and Oregon12), and meeting agendas of the Direct Primary Care Coalition13 and Direct Primary Care Summit14 held in June 2014. We included all practices that met the 3-part definition of DPC (identified via the above-described methods) either exclusively as a “pure” DPC practice or as part of a split practice model.
The following data were collected: number of physicians in the practice, number of nonphysician clinicians, lowest periodic (monthly) fee for patients older than age 29, highest periodic (monthly) fee for patients older than age 29, any per-visit fee, any enrollment fee, Medicare opt-out status, whether the practice was split, and the terminology the practice used to advertise (self-describe) its membership model.
An estimation of the total average monthly cost of care was obtained by averaging the monthly low and high costs, assuming patients visited the practice an average of 4 times per year,15 and amortizing the first year's enrollment fee over a 12-month time period via the following formula:

Results
DPC practices tend to fall naturally into 1 of 3 cohorts: (1) small and independent practices with varying levels of network affiliation, (2) split practices that are either independent or often entirely dependent on a network for their DPC patients, or (3) larger practices that tend to employ physicians and grow rapidly by marketing themselves directly to large employers. Many other arrangements certainly exist; of note, one hospital offers an “Affordable Access” DPC program at $30 per month,16 and even some urgent care chains17 are offering DPC options.
Networks may be used by providers for a variety of different purposes, from learning about the model to recruiting/enrolling patients (especially from large employers), sharing group purchasing discounts, and sharing electronic medical records and membership management platforms. Examples of networks are available in the full practice listing in the Appendix. Because of the variety of network options and lack of transparency regarding practice participation in networks, precise data could not be aggregated from this website review.
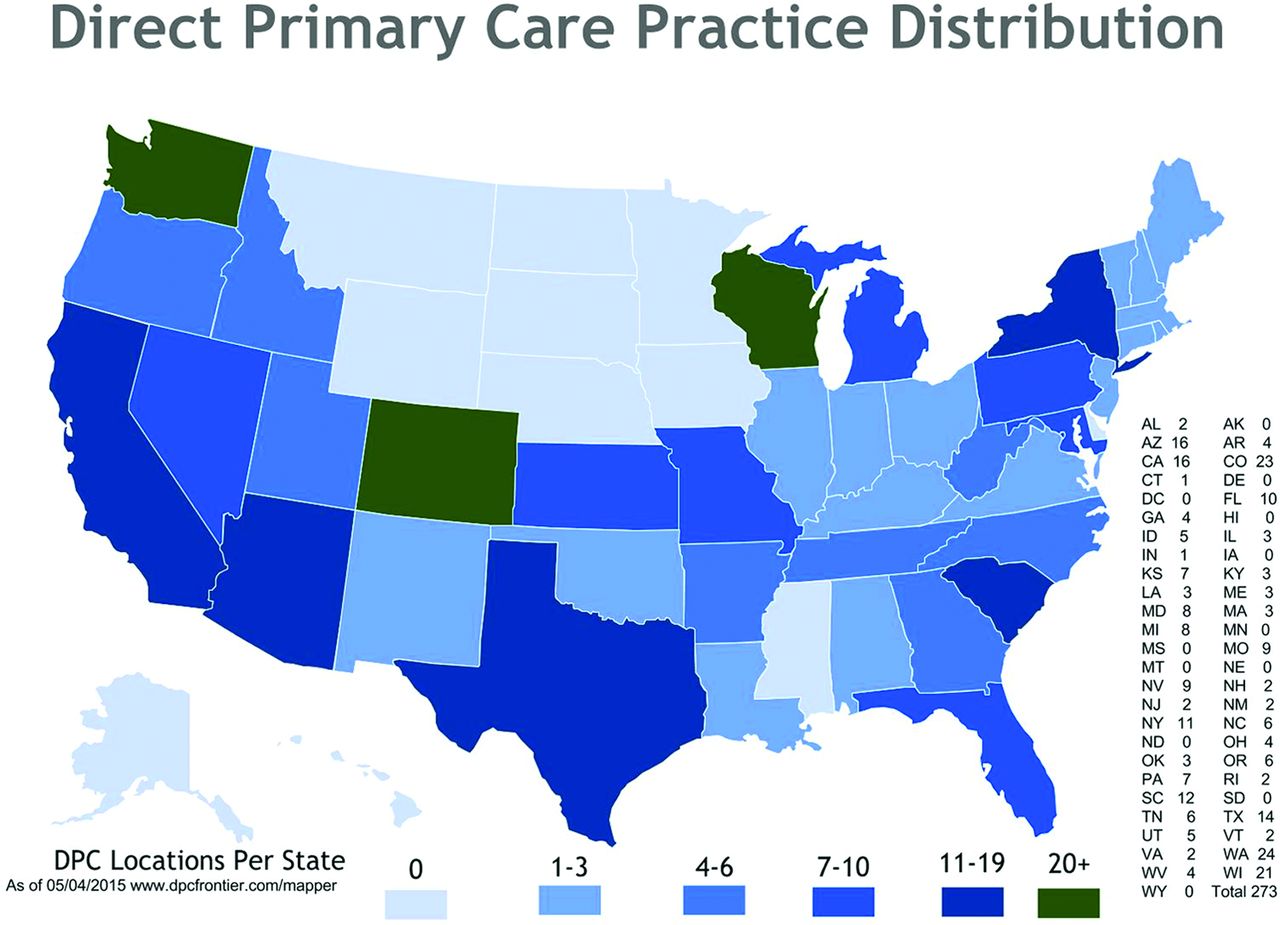
We located 141 practices with 273 locations spanning 39 states (see Figure 3 and the Appendix). Practices with ≤4 providers comprised 93.2% of those included in the study. Of the 141 practices, 87 disclosed enough information for us to determine whether they were “pure” or “split” (73 [83.9%] were pure and 14 [16.1%] were split), and 84 disclosed enough information for us to determine whether they had opted out or were accepting Medicare (65 [77.4%] opted out and 19 [22.6%] accepted Medicare). Of the 65 practices that opted out of Medicare, 1 operated in a split fashion. A practice self-description was recorded for every practice in the study. The following terms were used: DPC by 75 practices (53.2%), concierge by 21 (14.9%), direct by 17 (12.1%), and other by 22 (19.6%).

Direct primary care practice distribution. DPC, direct primary care.
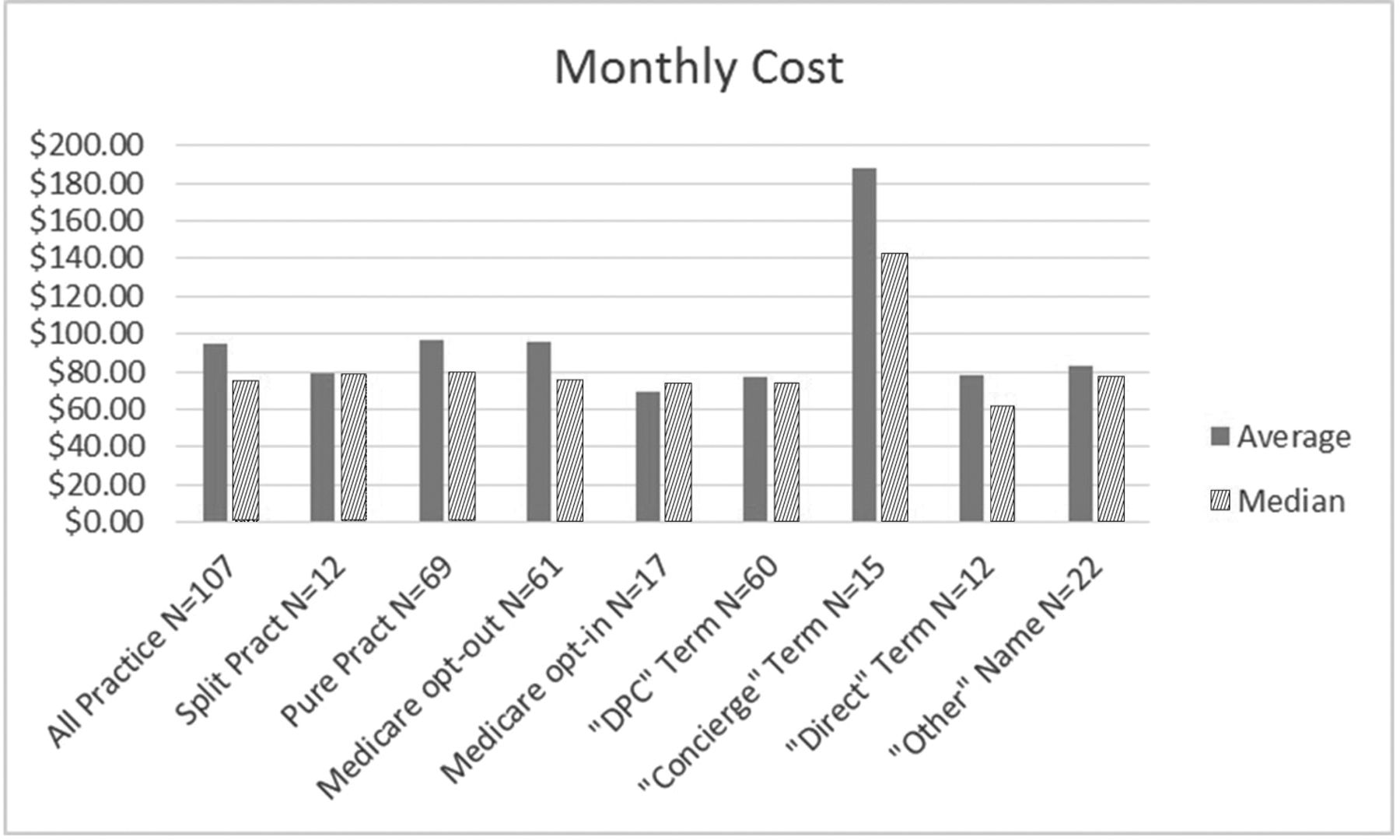
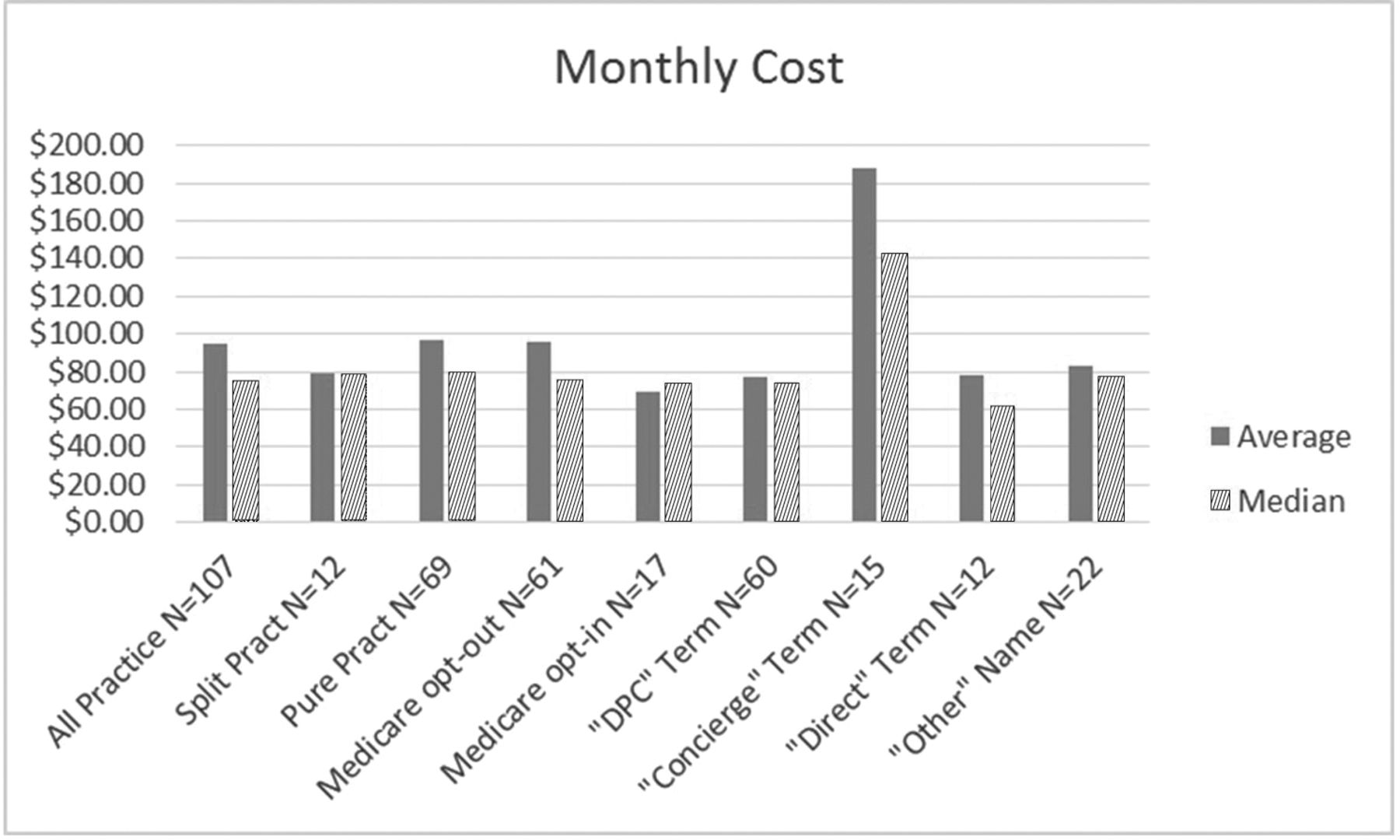
Of the 141 practices identified, 116 (82%) have cost information available online. When these 116 practices are analyzed, the average monthly cost to the patient is $93.26 (median monthly cost, $75.00; range, $26.67 to $562.50 per month). While all the practices included in our study met our definition of DPC, not all the practices used the phrase “direct primary care” to self-describe their practice model. Seventy-five of the studied practices (53%) referred to their model using the phrase “direct primary care.” Practices that used the phrase DPC on average charged a lower fee than practices that used the term concierge to describe their model: $77.38 compared with $182.76, respectively. Of 116 practices with available price information, 28 (24%) charged a per-visit fee, and the average per-visit charge among this group was $15.59 (range, $5 to $35). Thirty-six of these 116 practices charged a one-time initial enrollment fee, and the average enrollment fee among this group was $78.39 (range, $29 to $300). Figures 1 and 2 present monthly cost data.

Monthly costs to patients. DPC, direct primary care.
Average monthly price (sorted from low to high) and grouped by practice self-description.
Most DPC practices are young and small and thus lack sufficient quality and cost data to assess outcomes. The larger practices (especially Qliance, Iora Health, and Paladina) are known to have patient panels as large as 40,000 and routinely grow at faster rates by marketing themselves to large employers looking to purchase DPC plans for their employees. Most DPC practices are too small or young to have collected quality outcomes data, but we identified 2 mature practices that have compiled information: Access Health Care and Qliance.18
Access Health Care has been deemed a Cardiovascular Center of Excellence since 2009 by the Consortium for Southeastern Hypertension Control.19 An unpublished study performed by the University of North Carolina School of Medicine and North Carolina State University MBA students demonstrated that the group's DPC patients spend 85% less out of pocket for their total cost of care compared with the same level and amount of care in a traditional setting. Patients receive an average of 35 minutes per visit (compared with 8 minutes in the traditional model).20
Qliance is the first example of a corporate, multisite DPC model.21 Internal data from the group demonstrates that Qliance patients have a >50% reduction in emergency department visits, specialist visits, advance radiologic testing, and surgical procedures than traditional practices.22,23 The only measure of increased utilization is the number of primary care visits, which more than doubled from an average of 2 to an average of 4 per year during the reporting period.23 The logical inference is one that primary care advocates have insisted is true in every health system: As the utilization of low-cost comprehensive primary care increases, the need for high-cost emergency and specialty services decreases.
Though Qliance initially enrolled individual patients, currently employers (such as Expedia) contract with Qliance to pay membership fees as an employee benefit. Qliance recently enrolled an additional 20,000 patients via a Medicaid managed care contract, where Medicaid simply pays the membership fee on behalf of the patients as part of a shared savings program.23 Another 5,000 patients signed up with Qliance via the insurance exchange. This was made possible by a provision of the Affordable Care Act that permits DPC practices to be offered in a bundled fashion in the insurance exchanges when paired with a wraparound insurance policy.24
The Affordable Care Act contains a provision in Section 10104 stating that the Department of Health and Human Services “shall permit a qualified health plan to provide coverage through a qualified direct primary care medical home plan that meets criteria established by the Secretary…”24; the Department of Health and Human Services later described a direct primary care medical home plan as “an arrangement where a fee is paid by an individual, or on behalf of an individual, directly to a medical home for primary care services, consistent with the program established in Washington.”25 This ACA provision and similar topics are discussed in detail in the article providing a legal and regulatory review of DPC by Eskew.5
Discussion
A medical literature search did not identify a consistent or consensus definition of the DPC model; thus we relied on a detailed legal analysis to articulate the 3-part definition of DPC used for this study. Prior editorial publications often used terminology indiscriminately, contributing to broad misperceptions about the nuances among DPC, concierge, and other periodic fee models. A narrow majority of practices in the study self-describe as DPC. Practices are certainly free to advertise in any manner they chose, but this inconsistency in terminology certainly contributes to confusion on the part of patients and policymakers.
Selection of geographic location seems to be fairly flexible. Practices are located in both urban and rural settings across 39 states. The exact locations of DPC practices that met our definition are continuously updated online in the DPC Mapper.26 Earlier studies demonstrated that each state's regulatory environment is different, and this may play a role in why some states have more DPC practices than others.27 Physicians wishing to start a DPC practice may need to spend time understanding the legal and regulatory requirements at both the state and federal levels that will affect the practice.5
We found the public perception of the term concierge as having higher prices holds true. Self-described DPC practices charged a lower average monthly fee ($77.38) than DPC practices that self-described as concierge ($182.76). Concierge practices such as MDVIP and MD2 have listed average periodic (monthly) fees of $137.50 and $2083.33, respectively; these periodic fees are billed in addition to standard fee-for-service office visit and procedural charges that would be encountered in any traditional medical practice.28
The third-party fee-for-service payment system compensates physicians on a per-unit basis. Physicians billing for a small number of units at high prices (common in specialties that perform expensive procedures) may find that the overhead cost associated with processing each claim is acceptable. In an outpatient-focused practice where procedures are less frequent and/or less expensive, DPC physicians have found that the overhead associated with collecting fees on a per-unit basis is too high to be worth the effort. The administrative efficiencies gained by abandoning third-party fee-for-service overhead are often cited as one of the chief reasons that DPC is offered at minimal cost to the patient. We anticipated that the presumed lower overhead costs in “pure” DPC practices would result in lower periodic fees when “pure” practices were compared with “split” practices that should continue to carry a higher overhead burden, but there was no significant difference in periodic fees between the 2 groups.
Limitations in calculating the monthly costs include (1) complicated price structures (some practices offer family discounts, employer discounts, and other pricing options that could not be easily incorporated into this formula); (2) a lack of price transparency on many practice websites; and (3) scope of practice variance (items covered by the membership fee vary widely). Some practices provide some medications, laboratory testing, and radiologic testing without additional costs. The second most expensive DPC practice included in our website review includes hospitalist (inpatient) services without an additional physician fee.29
Future studies should focus on obtaining data supporting the quality claims made by DPC physicians and patients. DPC practices typically advertise open and continuous patient access to the physician and, according to preliminary, proprietary, and unpublished practice-level data, may be associated with better health outcomes with fewer hospitalizations, fewer emergency department visits, fewer specialist visits, and less radiologic testing. Proponents of DPC practices regularly refer to these benefits, but if the model is to be more widely adopted, more data about DPC practices are needed to document potential improvements. DPC practices should be described using accurate and consistent terminology to minimize confusion, and continued efforts at price transparency at all levels are recommended.
Appendix
Listing of DPC Practices
121MD
Access Direct Care
Access Health care (Albenberg)
Access Health care (Forrest)**
Access MD
Access Medical Home
Access Medicine
Akin Family Medical Care
Alliance Concierge Care
Alonso, Lynn, MD
AMG Medical Group*
Anchor Medical Clinic
Appleton Clinics
Assurance Healthcare & Counseling Center
AtlasMD**
Austin Osteopathic Family Medicine
Balance Health
Baskin Clinic
Belleview Medical Partners
Birdwell Ferris Clinic
Bluegrass Family Wellness
Bluesky Direct
Bridge City Family Medicine
Broderick, Dawn, MD
Brooks Family Care
Care Only
Carlson, Rhonda, MD
Ciampi Family Practice
Compass Health care
Consolaré Personal Physician Services
Crescent Medical
Criscenzo, Donna, MD
Cunningham, Alicia, MD
Davinci Medical DPC
DC Clinic Northwest Arkansas
Diamond Luxury Health Care
Direct Access Family Care
Direct Doctors Inc.
Direct MD Austin
Direct Patient Services
Direct Primary Care of Austin
Direct Primary Care Carolinas
Direct Primary Care Clinics
DirectcareMD (Heritage FM)
Direct Medical Care
The Doc Shoppe
Dr. Rob Lamberts, LLC
Epiphany Health
Evolve Medical Clinics
Exceptional Health Care
Faith Family Clinic
Family Health Center Direct
Fields, Robert, MD
Flat Rock Health
Forest Direct Primary Care
Free Market Physician
Freedom Family Practice
Functional Family Medicine
Furlow, John, MD
Gold Direct Care
Good MD
GracePointe Health Care
Green Medicine
Guardian Family Care
Hannon & Maltz
Health Access Rhode Island**
A Heartbeat Away Clinic
Henjum, Philip, MD
Hendler, Jared, MD
Highland Urgent Care & Family Medicine
Icon Pediatrics
Independent MD
Innova Medical Care
Insight Primary Care
Institute for Medical Wellness
Integrative Family Medicine Asheville
Iora Health*
Island Direct Care
Ivers, Greta, MD, MPH
Izbiki Family Medicine
Kaysville Clinic Family Med
The Knope Clinic
Lacamas Medical Group
Landsdale, Thomas, MD
Live Active Primary Care
Lutz, Kevin, MD
Marable (Sublime) Health care
Megunticook Family Medicine
MDStat Urgent Care
Medical Access USA
Medlion**
Melioria Family Medicine
Morningstar Family Health Center
MyDoc Personal Physician Service
NeuCare Family Medicine
Nextera Health Care
Northwest Direct Care
Nostalgia Family Medicine
Oasis Family Medicine
One Focus Medical
Osteopathic Center Family Medicine
Our Lady of Hope Clinic
Pacific Direct Care
Paladina Health*
Palmetto Proactive Health care*
Patient Centered Physicians Group
PeaceHealth Medical Group
PeakMed Primary Care
Personal Family Physicians
Prairie Health & Wellness
Premier Personal Health Care
PrimaraCare**
Primary Care One
Priority Health Family Medicine
Priority Physicians
ProPartnersMD Direct
Qliance*
R Health Connect
Revolutionary Health Services
Rio Picos Family Practice
River Rock Medical Clinic
Roark Family Health
Rockville Concierge Doctors
Roth Medical Clinic
Salud Optima Direct
Samuel, Richard, MD
Sanctuary Medical Care & Cons
Scotland Family Medicine
Seattle Medical Associates
Seattle Premier Health
Snoqualmie Ridge Medical Clinic
Solstice Health
SparkMD
Treasure Valley Family Med
Unorthodoc
Vantage Physicians
The Village Doctor
Washington Park Direct Care
Yapha Physician Services
Wells Medical Clinic
Zenith Direct Care
*Large (>5 providers)
**Network total = 141.
A white article by Dave Chase,31 written for the California Health Care Foundation, highlighted Iora Health, MedLion, Paladina Health, and White Glove Health. Similar helpful white articles have been published by Jarrett Flood32 for the Louisiana Lawmakers and by Daniel McCorry33 for the Heritage Foundation. Iora Health mainly operates employer-focused DPC practices often providing services for union groups using physicians paired with health coaches. MedLion is another type of DPC network, with >40 practices across the United States, that claims its “largest client is a 100,000 member association, and its smallest has 3 part-time employees.”34 Paladina Health is a DPC practice operated by the DaVita Corporation with at least 37 clinics across 8 states, and they also are focused on marketing DPC services directly to employers. White Glove Health is an entity focusing on house calls performed by nurse practitioners and does not offer the full scope of primary care services; therefore it did not meet our definition of DPC. Brian Forrest, of Access Health Care, also has a network known as Access Health Care Direct, and AtlasMD sells a comprehensive software solution to DPC practices that includes many features often found in a network.
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: none declared.
- Received for publication December 9, 2014.
- Revision received May 5, 2015.
- Accepted for publication May 11, 2015.
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- A Narrative Review of Slow Medicine Outcomes
- Direct Primary Care: Applying Theory to Potential Changes in Delivery and Outcomes
- "A Paradox Persists When the Paradigm Is Wrong": Pisacano Scholars' Reflections from the Inaugural Starfield Summit
- Real Life Is Full of Choices
- New Tools and Approaches for Family Physicians