
Abstract
Background: Intimate partner violence (IPV) victims frequently seek medical treatment, though rarely for IPV. Recommendations for health care providers (HCPs) include IPV screening, counseling, and safety referral. The objective of this study was to report women's experiences discussing IPV with HCPs.
Methods: This study used structured interviews with women reporting IPV discussions with their HCP; descriptive analyses and bivariate and multivariate analyses were performed, and association with patient demographics and substance abuse was reviewed. We included women from family court; a community-based, inner-city primary care practice; and a tertiary care-based, outpatient psychiatric practice.
Results: A total of 142 women participated: 44 from family court (31%), 62 from a primary care practice (43.7%), and 36 from a psychiatric practice (25.4%). Fifty-one percent (n = 72) of patients reported that HCPs knew of their IPV. Of those, 85% (n = 61) told a primary care provider. Regarding IPV attitudes, 85% (n = 61) found their HCP open, and 74% (n = 53) found their HCP knowledgeable. Regarding approaches, 71% (n = 51) believed their HCP advocated leaving the relationship. Whereas 31% (n = 22) received safety information, only 8% (n = 6) received safety information and perceived their HCP as not advocating leaving the abusive relationship.
Conclusions: Half of participants disclosed IPV to their HCPs, and most perceived their provider advocated them leaving the relationship. Only 31% reported that HCPs provided safety planning despite increased risks associated with leaving. We suggest HCPs improve safety planning with patients who disclose IPV.
Intimate partner violence (IPV) is a major public health concern affecting approximately 24% of US women at some point in their lifetimes.1 Experiencing IPV is associated with negative mental and physical health outcomes and increased use of health care services.2⇓–4 Ample research demonstrates significant financial costs to both the patient and the health care system.5 Primary care estimates of IPV prevalence range from 4.9% to 29% and up to nearly 50% in inner-city practices.4⇓⇓⇓⇓⇓⇓⇓⇓–13 Approximately one third of women injured during their most recent physical assault received medical treatment, providing an opportunity for health care providers (HCPs) such as physicians, nurses, physician assistants, and nurse practitioners to intervene.14 However, most outpatient visits by women experiencing IPV are for non–injury-related complaints, and most affected women do not spontaneously disclose their IPV, thus highlighting the need for comprehensive measures to identify IPV.15,16 IPV has been found to be underdocumented in clinical settings.16 Interviews with HCPs17 and transcripts of patient–physician encounters18 have demonstrated that HCPs often have difficulty asking about IPV as well as addressing IPV when it is disclosed. These findings have generated numerous training tools and interventions to help HCPs better address IPV, but no study has demonstrated sustained improvements in addressing IPV in clinical practice.19⇓–21 Sims et al15 reported no increase in questioning about IPV after an educational intervention for trauma residents, suggesting that education alone may not increase IPV detection without profession-wide guidelines. In addition, documenting IPV by using standard diagnostic codes may warrant caution given concerns for safety and confidentiality.22 In response to the accumulated evidence, the Institute of Medicine (IOM) of the National Academies and the Department of Health and Human Services have recommended culturally sensitive and supportive screening as well as counseling for current or past IPV for all women and adolescent girls.23
Nearly 20 years of research about IPV identification and HCP communication may have affected community practice standards. Recommendations have been based on both preferences and outcomes reported by IPV survivors and include referral to IPV specialists, safety planning, and providing nonjudgmental support regardless of the woman's decision to stay or leave the relationship.24⇓⇓⇓⇓–29 However, there is little knowledge outside of controlled educational interventions about the extent to which current medical practitioners follow expert recommendations, such as those issued by the IOM.
There is a paucity of literature about women's comfort with discussing experiences of IPV with health care providers as well as the degree of confidence women have in their providers' advice. McCauley et al30 found that women frequently cited fear of HCP response as a barrier to disclosure. A qualitative study of IPV survivors identified 5 dimensions of provider behaviors that facilitated patient trust: open communication, professional competency, accessible practice style, caring, and emotional equality.31 Another qualitative study of IPV survivors in emergency, primary care, and obstetric/gynecologic settings concluded that patient satisfaction was related to provider acknowledgment of the abuse, respect, and relevant referrals,32 and a quantitative experimental evaluation of a system change intervention to improve emergency department responses to IPV showed that those who were screened for IPV in an emergency department had higher patient satisfaction than those who were not.33 Studies of women's preferences regarding mandatory reporting indicate that abused women prefer to be given options about what actions to take, rather than being advised directly to leave an abusive partner.34,35 Although studies have addressed patient preferences, the degree of patient comfort with and confidence in HCPs' IPV knowledge and advice after such clinical discussions have not been reported. HCPs may not be knowledgeable about the risks of leaving the abusive relationship without a safety plan in place36 or the complexity of women's decisions about leaving or staying and therefore may simply recommend leaving the relationship or respond judgmentally to a woman who expresses ambivalence about leaving. The purpose of this study was to understand women's perspectives about their experience with IPV disclosure in health care settings and to compare this with current expert guidelines for screening and intervention by HCPs.
Methods
In this study, we present the first analysis of this subsample from a larger project studying IPV-related health care and patient attitudes. Methods for this study are based on community-based participatory research strategies.37 The research team conducted preliminary discussions with women from a local battered women's shelter to obtain input about study recruitment and methodology. These women also participated in mock structured research interviews; the research team incorporated their feedback into the study protocol and structured interview script.38
Participants and Settings
Between February, 2007, and July, 2008, research assistants recruited participants from a family court, a primary care practice, and a tertiary care–based outpatient psychiatric practice for a health care research project. These sites were chosen to draw a sample of women with a range of experiences with health care. We specifically in the courts women who might not have an identified medical home. Inclusion criteria for the study were age older than 18 years, ability to consent, and self-reported lifetime history of IPV. Participants were asked to identify one abusive relationship, either past or present, and anchor all questions being asked to that relationship.
Procedures
At both health care sites (inner city primary care practice and hospital-based psychiatric practice), primary providers were trained to screen all patients for a lifetime history of IPV using an identification tool for domestic violence that was embedded into a pre-existing practice questionnaire. Those who screened positive were invited to meet with a research assistant conducting a study regarding relationships. At the primary care practice, a poster in the patient waiting area also advertised the study. At family court, recruiters approached potential participants in 2 locations: the secure area designated for petitioners of orders of protection and from a family court reception area.
At each site, trained recruiters arranged for a private, onsite interview or follow-up appointment with interested participants. Participants received a $25 cash incentive after the interview was completed, a small resource card with the names and numbers of appropriate agencies to provide the patient with information about abusive relationships, and a hotline number to speak with someone as needed. Those who declined participation at any stage in the process were offered only the small resource card.
Measures and Analyses
The survey included questions about demographic characteristics and patient interactions and discussions with HCPs about IPV.
Demographic Characteristics
Participants reported their age (recoded as 18 to 35 years, 36 to 45 years, or 46 to 65 years); education (recoded as high school graduate or less, or some college or more); individual income (recoded as less than $20,000 or $20,000 or more); ethnicity (recoded as white or nonwhite); and substance use (answered yes or no to having a problem with drugs or alcohol). Substance use was included because of its associated risk with IPV.39
HCP–Patient Interactions Regarding IPV
On the basis of the input from shelter participants noted earlier, the team developed 12 questions to assess HCP- and patient-driven communication regarding patients' experiences with IPV. Participants were asked if their HCPs asked them about abuse in their intimate relationships, excluding the screen done just before study recruitment. They also were asked to answer questions about their HCPs' openness, ability to help, and influence on their decision to stay or leave the abusive relationship (see Table 1).
Data Analysis
We conducted a mixed-method analysis40 of the scribed, semistructured interviews, which we informed with selective qualitative quotes from women who found their disclosure to their HCP to be either helpful or unhelpful. χ2 tests were conducted to determine the associations between participant demographic and background variables and recruitment site (see Table 2).
Descriptive analyses of the qualitative data were performed. For the portion of the structured interview questions that were open-ended, 2 individuals (one co-author [RL] and one research assistant [JB]) coded the narratives to help determine the nature of the HCP–patient communication regarding IPV. The coding was done separately, and any disagreements were resolved by discussion until consensus occurred. Regarding whether the HCP directly advised the patient to stay or leave, we looked to the “How do you know?” (that your HCP wished for you to stay or leave) question (Table 1). Regarding safety advice or referral and how the HCP was helpful or unhelpful, we looked for references to that physician behavior in all the open-ended questions (Table 1). We selected some participants' narrative statements that were illustrative of the major themes regarding helpful or unhelpful HCP behaviors or statements from the structured interviews to further inform this analysis.
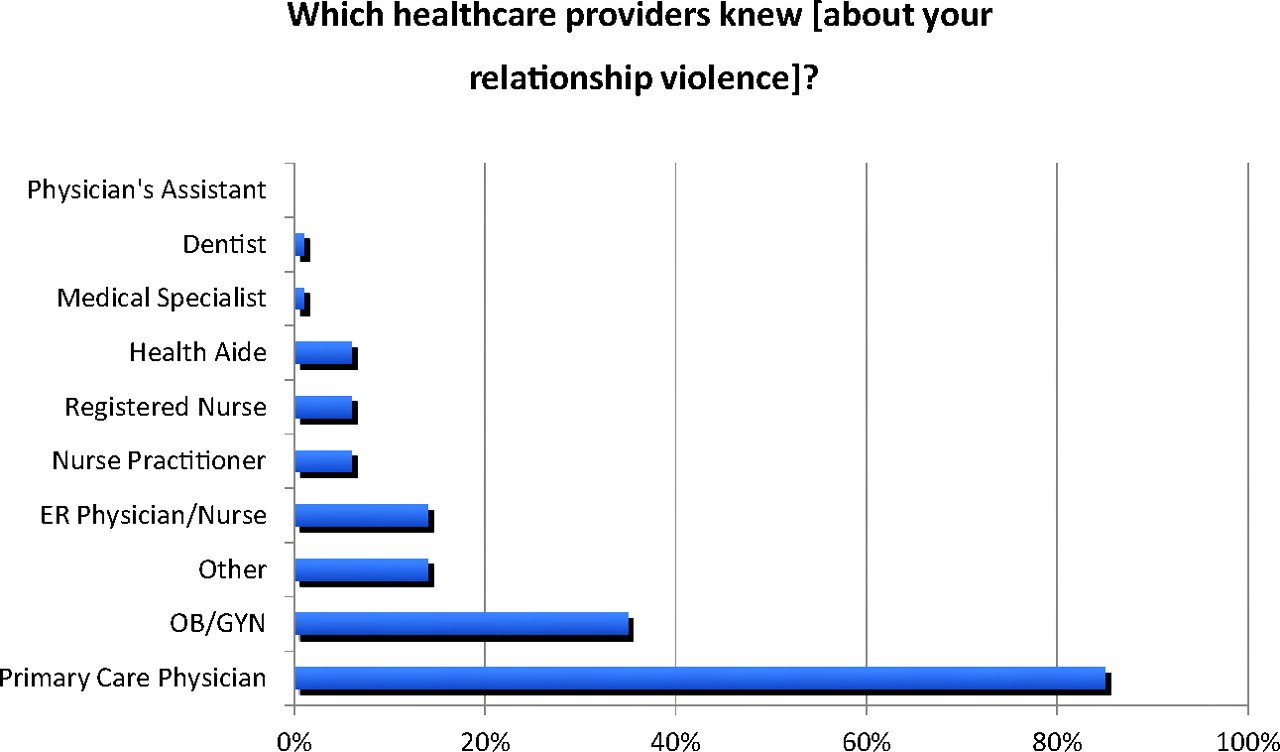
We quantified the various HCPs with whom patients discussed IPV, as shown in Figure 1. To assess whether demographic characteristics were associated with HCPs asking about IPV or not, we performed multivariate logistic regression with the HCPs asking about IPV as the dependent variable and age, race, substance abuse history, and employment as independent variables for all 142 participants. Lastly, we performed χ2 bivariate analysis with 72 participants who reported discussing IPV with an HCP. We analyzed variables relating to these participants' views of their HCPs' attitudes, perceptions, and knowledge about the care of women in abusive relationships.
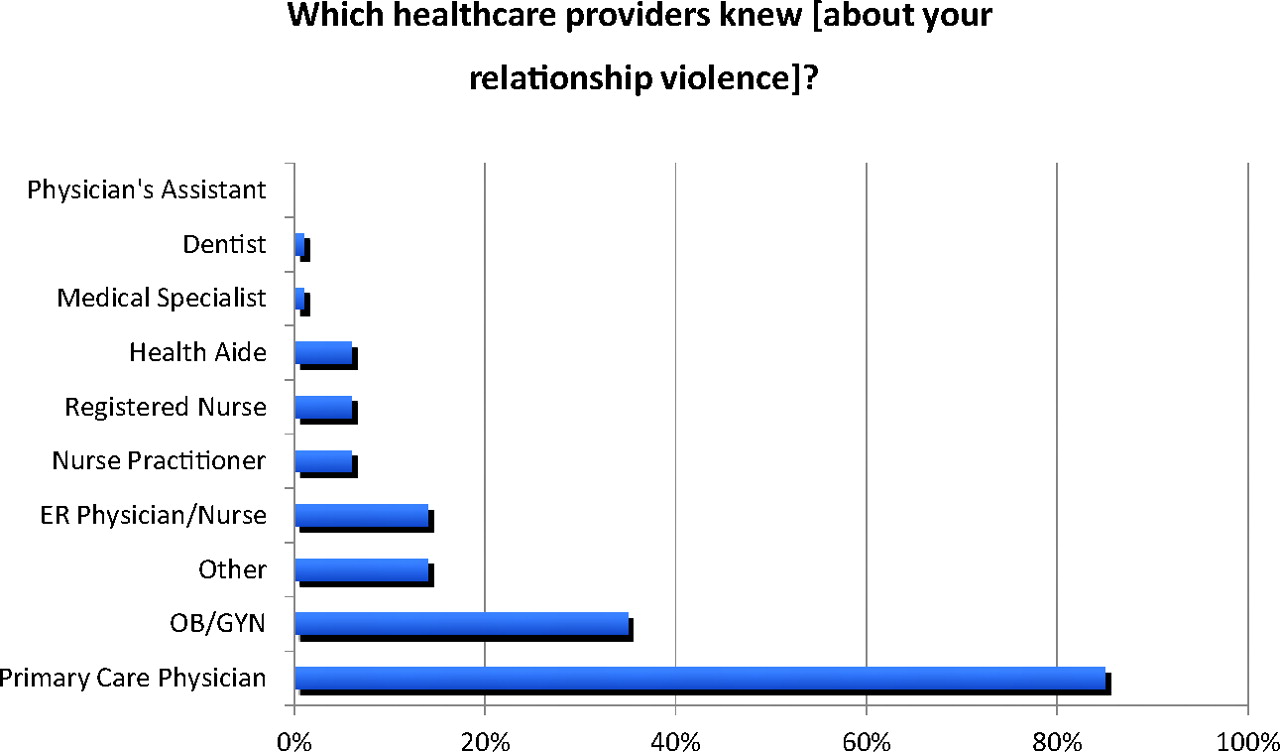
Interview response percentages to question, “Which health care providers knew [about your relationship violence]?”
Results
Data were available from 142 of the original 150 women who took part in the health care study (we excluded 8 participants because of missing demographic data). Sixty-one percent (n = 87) of the women were nonwhite. Participants had relatively low educational attainment, with 68% (n = 97) having earned a high school diploma or less, and were low income, with 88% (n = 124) reporting an annual individual income less than $20,000. Participation criteria required an age range from 18 to 65 years, with 41% (n = 59) aged 18 to 35 years, 32% (n = 45) aged 36 to 45 years, and 27% (n = 38) aged 46 to 65 years.
The demographics of the sample, divided by recruitment site, are displayed in Table 2. The demographics of our participants differed by site for race, age, education, and alcohol abuse. The family court (70.5%; n = 31) and primary care practice (66.1%; n = 41) sites had more minority women compared with the psychiatric practice (41.7%; n = 15). Family court also had a greater number of younger women (65.9%; n = 29). Twenty-four percent of respondents at the primary care practice noted an alcohol problem, in contrast with only 13.9% and 2.3% at the psychiatric practice and family court sites, respectively. Differences in reported drug use between sites were not significant. Notwithstanding these differences in race, age, and alcohol abuse, we combined the samples for our subsequent analyses because they represent predominantly low-income women with histories of relationship violence.
Of the 142 female participants, 51% (n = 72) reported that their HCPs—including medical doctors, nurses, nurse practitioners, and physician assistants—knew of the abuse in their relationships (see Table 1). Of those participants, 65% (n = 47) reported that they had been asked about IPV by a HCP, which indicates that 65% of these HCPs are following the recommended guidelines. However, in a different question, only 31% (n = 22) reported having volunteered information about IPV to an HCP. Eighty-five percent of the participants whose HCP knew of their abuse (n = 61) reported having told at least one primary care provider, including 25 who said they reported to their obstetrician/gynecologist. Of the 49% (n = 70) who reported that their HCPs did not know about the abuse, 63% (n = 44) indicated they would have disclosed the information if their HCP had asked.
Logistic regression revealed that race, employment, and self-reported drug use were not associated with an HCP asking about IPV. However, women aged 36 to 45 years were almost 4 times as likely to say they had been asked (odds ratio, 3.99; 95% confidence interval, 1.53–10.44) compared with the reference group (women aged ≤36 years).
Of the 72 women who reported that their HCP knew about the abuse, 85% (n = 61) reported their HCP was open to talking about IPV, 65% (n = 47) felt comfortable approaching their HCP about it, and 74% (n = 53) felt their HCP was knowledgeable about the topic.
Among the 72 participants whose HCPs knew of the abuse, 71% (n = 51) reported they felt their HCPs wanted them to leave the abusive relationships, and half of those (n = 27), or 37.5% of the total, stated that their HCP specifically advised them to leave their abusive partners (see Table 3). Twenty-five percent (n = 18) of the abused women reported their HCP advised them to leave the abusive partner but the women did not indicate they were given any safety advice. Few participants (31%; n = 22) reported safety assistance such as referral to community agencies. Only 6 women (8%) stated that HCPs offered safety advice and left the decision about leaving or staying in the abusive relationships to them. Considered by site among the same 72 participants who spoke with their HCP about abuse, 43% (n=9) recruited at the psychiatric practice reported receiving safety advice, compared with 31% (n=10) at the primary care practice and 16% (n=3) recruited at the family court.
The following quotes are from participants who described the HCP as helpful:
“[My doctor] was a friend and the only one I could trust…”
“[My doctor was] compassionate, supportive. She took her time with me and spent about 2 hours when I broke down.”
“I felt like it helped me because [the doctor] was supporting my decision to get help…”
“He will kill you—get out…” [HCP statement to participant]
The following quotes are from participants who described the HCP as unhelpful:
“I felt scared that [the doctor] would report me to the police, welfare…”
“Persons in emergency brought up the situation when my husband was still there…then they asked him to leave and I was scared.”
“‘All those times that you kept going back, I told you not to go back, now you are on your own.’ [HCP statement to participant] I changed doctors after that.”
“[I felt] embarrassed and unprotected. I felt like [my doctor] defended my husband.”
“I was in such denial that I didn't want to hear any of her advice and opinions; closed ears…”
“I want to get pregnant. My OB/GYN [won't prescribe] my meds, so I won't get pregnant. If I leave him she will give them to me again. I have an illness that keeps me from getting pregnant.”
Discussion
In this study of 142 low-income women who have experienced IPV, half of the participants reported disclosing abuse to an HCP. Of those who disclosed IPV to an HCP, 65% did so in response to being asked; only 31% volunteered their IPV status. Among those who did not disclose to an HCP, 63% stated that they would have disclosed if they had been asked. Eighty-five percent of the women who disclosed IPV told a primary care provider. Among the women that disclosed IPV to an HCP, 71% felt that their provider wanted them to leave the relationship, with 37.5% reporting being specifically directed to leave. Among the women who disclosed IPV to an HCP, 69% were not provided safety advice. Finally, among the women who disclosed IPV to an HCP, 65% to 85% felt comfortable and believed their HCP to be open or knowledgeable regarding IPV. In this study, women aged 36 to 45 years are 4 times more likely to be screened for IPV.
Most of our participants who told an HCP about IPV reported having disclosed their abuse to a primary care provider. This finding demonstrates the prominent role such providers play for these patients and supports current recommendations for primary care providers to screen for and address IPV. Importantly, women seeking orders of protection sought care at the emergency department at twice the rate that they utilized primary health care, and 40% reported delayed medical care in the past year.38 Hence, HCPs may see a patient only once, further reinforcing asking all patients about IPV, even at the first visit.
Another important finding in our study is that only half of our participants had disclosed IPV to a HCP; almost two thirds of those disclosed IPV only when they were asked, and most of those who did not disclose IPV reported that they would have disclosed it if they had been asked. These findings support the practice of routine inquiry of IPV in all patients, as has recently been recommended by an IOM report,23 a recommendation accepted by the secretary of the DHHS. Women who have disclosed their IPV experience to an HCP have been found to be more likely to report receiving an IPV intervention, which is associated with leaving the abusive relationship and improved health outcomes.41,42 Not inquiring of all patients ensures that IPV will be underdetected and therefore undertreated. To fulfill the DHHS directives, HCPs will benefit from using evidence-based guidelines to respond to women who disclose IPV on routine inquiry.
Among our participants, 69% reported that they had not received safety advice regarding IPV, whereas 71% reported feeling that their HCP wanted them to leave the abusive relationship. If providers feel helpless to address the needs of women experiencing IPV, they may focus on counseling the woman to leave the abusive relationship without adequately providing information about other strategies and, if the woman wants to leave, ensuring safety procedures are in place. Risk of femicide is increased significantly during the year after an abused partner leaves the abuser,36 yet only 50% of survivors of attempted femicide reported being aware of their extreme risk, hence increasing susceptibility to possibly unsafe suggestions or a lack of adequate safety planning.43 Furthermore, some abused women reported that fearing providers will require them to leave an abusive relationship to receive help was a barrier to seeking such help, supporting the importance of our results.44
A positive finding in this study is the degree of comfort with and confidence in their HCPs, most of whom were primary care providers, that abused women reported and the extent to which the women looked to the HCPs for help in managing this complex situation. However, there is discordance between this confidence and the finding that HCPs rarely provided safety planning and a nonjudgmental approach to the question of staying or leaving the abusive relationship. In addition, supporting patients' autonomy to make their own choices is associated with other positive outcomes such as improvements in satisfaction, well-being, and change associated with intrinsic rather than extrinsic motivation.45,46
Our finding that participants perceived their HCP to be advocating leaving the abusive relationship raises the question of whether someone who becomes aware of a dangerous (physically, emotionally, or both) situation would not reasonably want the person in danger to leave it. It is also possible that those participants who were not directly advised to leave may have assumed their provider wanted them to do so because it is one reasonable response to an abusive relationship. The fundamental question is whether someone can be supportive of a patient making her own decision and still want her to change her situation. Research on motivation regarding substance abuse and adherence to medical recommendations helps to address these questions. Empathy, information, and support can be provided to increase patient autonomy and perceived competence, consequently improving health outcomes.47⇓–49 Qualitative research among the IPV survivor population supports the notion that respectful information-sharing and support by HCPs will help break the cycle of control, degradation, and physical violence that constitutes IPV.28⇓⇓–31
In July 2011 the IOM recommended universal IPV screening, noting the prevalence of IPV and the need to address current and future health risks.23 Nevertheless, there has been a lack of consensus regarding the utility of screening women for IPV.50 It is possible that one reason for the lack of clear efficacy of some screening interventions relates to the difficulty HCPs have with the complex and numerous tasks that have been suggested when the patient screens positively, such as assessing mechanisms of injury and child safety.51 Clinical practice, policy, and research implications of this study would be to focus on establishing fewer HCP responses to a determination of ongoing IPV. In this study, participants reported that HCPs conveyed support, as has been suggested by IPV survivors,29 but did less well with safety-related suggestions. Hence, focusing educational efforts on getting HCPs to provide a referral to a trained IPV provider at a local shelter or a national toll-free hotline (1-800-799-SAFE (7233)52 may be the appropriate strategy for primary care providers with multiple important tasks. Research regarding such a strategy could be important as well.
Our results suggest that patients look to their HCP for guidance and information, giving HCPs an opportunity to respectfully educate women to seek safety planning and impact their ability to make positive change. The cumulative evidence suggests that, after such referrals, HCPs should support patients' choices and decrease the focus on leaving the abusive relationship until resources are present to help avoid potentially serious harm.
A strength of this study is that women were recruited from different sites. Although other articles have focused on patient responses to HCPs in primary or emergency medical settings,18,31 ours broadens the population studied and adds to the literature by including participants recruited from 2 sites where biomedical care was not being obtained. Some differences by site were noted (Table 2) with regard to ethnicity and age. The family court sample was seeking an order of protection and was more likely to be younger and nonwhite, whereas the psychiatric practice clinic sample was likelier to be older and white. The primary health care population was less likely to have some college education, had a lower income, and was more likely to have an alcohol problem. These findings support our belief that we have assembled a diverse population. A larger sample may be needed to determine associated differences in IPV communication beyond the finding of women in the middle age group range being more likely to be asked about IPV by an HCP.
Our results should be considered with caution. This study is based on patient report. Other studies have utilized audiotape, videotape, or chart review to document actual HCP behaviors. This study focuses more on diverse patients' perceptions of and response to community HCPs' behaviors. Another limitation of this study is the lack of a qualitative thematic analysis of participant comments. Because such an analysis was not the purpose of this study, the depth and breadth of responses needed for such an analysis were not obtained.
Future studies could aim to test specific hypotheses regarding interactions between patient characteristics, HCP behaviors, and patient attitudes toward their HCPs. For example, do patient race, education, and income affect the likelihood that HCPs will ask about IPV? Would HCPs asking about IPV increase patient comfort and confidence and could that lead to an increase in needed health services use? If HCPs were trained to support patient autonomy regarding their decisions to stay or leave the abusive relationship, would this improve patient motivation to increase controllable safety behaviors?53 These important questions have yet to be addressed.
Conclusions
Among our diverse sample of women IPV survivors, only half felt comfortable enough to disclose IPV to an HCP. Among the half who did not disclose, 63% would have done so if they had been asked. For the half that did disclose, almost three-fourths thought that their HCP wanted them to leave the relationship, and only 31% received safety information. These findings contrast with more than three fourths of the survivors believing their HCPs to be knowledgeable about abuse. Although the sample size was limited, our results have implications for provider training and for new hypotheses that can be studied in larger intervention studies.
Acknowledgments
The authors thank Susan H. Horwitz, PhD, LMFT (primary investigator of McGowan project); Michelle LaRussa-Trott, LMSW; Joan Pearson, MA, MS, LMFT; Lizette Santiago, MS, LMFT; and David Skiff, PhD, MDiv, LMSW, for their help with project design and implementation. The authors thank the interviewers: Lorena Billone, BA, MFTT, Jessica Bougie, BA, and Stacy Kolb-Tripp, MS, and their statistical consultant, Harry Reis, PhD. The authors thank Meaghan Bernstein and Jessica Band for help with data entry and management and Jacqueline Campbell, PhD, RN, for her review of the manuscript. This project would not have been possible without the support of many administrators, mentors, and most importantly, participants. Special thanks to the organizations, Safer and Delphi, that assisted this study in the design before implementation.
Notes
This article was externally peer reviewed.
Funding: Funding provided by National Institute of Mental Health grants T32 MH18911, K01MH75965-01, and K01MH080660-01A2, as well as the McGowan Foundation.
Conflict of interest: none declared.
- Received for publication June 9, 2011.
- Revision received December 18, 2011.
- Accepted for publication December 21, 2011.




{kind=link}