
Abstract
Background: Unprecedented federal interest and funding are focused on secure, standardized, electronic transfer of health information among health care organizations, termed health information exchange (HIE). The stated goals are improvements in health care quality, efficiency, and cost. Ambulatory primary care practices are essential to this process; however, the factors that motivate them to participate in HIE are not well studied, particularly among small practices.
Methods: We conducted a systematic review of the literature about HIE participation from January 1990 through mid-September 2008 to identify peer-reviewed and non–peer-reviewed publications in bibliographic databases and websites. Reviewers abstracted each publication for predetermined key issues, including stakeholder participation in HIE, and the benefits, barriers, and overall value to primary care practices. We identified themes within each key issue, then grouped themes and identified supporting examples for analysis.
Results: One hundred and sixteen peer-reviewed, non–peer-reviewed, and web publications were retrieved, and 61 met inclusion criteria. Of 39 peer-reviewed publications, one-half reported original research. Among themes of cost savings, workflow efficiency, and quality, the only benefits to be reliably documented were those regarding efficiency, including improved access to test results and other data from outside the practice and decreased staff time for handling referrals and claims processing. Barriers included cost, privacy and liability concerns, organizational characteristics, and technical barriers. A positive return on investment has not been documented.
Conclusions: The potential for HIE to reduce costs and improve the quality of health care in ambulatory primary care practices is well recognized but needs further empiric substantiation.
Health information technology (IT) shows great promise for improving the efficiency, quality, and safety of medical care.1–3 The American Recovery and Reinvestment Act (ARRA) of 2009 reflects the Federal government's unprecedented interest in increasing the use of health IT to optimize our health care system.4 The ARRA devotes approximately $19 billion to increasing participation in health information exchange (HIE); that is, the electronic sharing of health-related information according to nationally recognized standards for interoperability, privacy, and data security.5 The goal is to create regional health information organizations (RHIOs) that will ultimately be linked to form a Nationwide Health Information Network.6
Adoption of electronic health records (EHRs) and HIE has lagged in primary care, where the majority of patient encounters occur.1 Currently only 21% of primary care physicians report having EHRs in their practices,1 and fewer still participate in HIEs. A fuller understanding of the factors associated with HIE adoption by primary care practices is needed to achieve the ambitious goal of nationwide HIE. This article is a systematic review of literature related to the adoption of HIE by ambulatory primary care practices, with an emphasis on benefits, barriers, and the overall value to the practice.
Methods
Databases, Search Strategy, and Article Selection
Research teams from the University of Minnesota and the University of Colorado applied a definition of HIE consistent with terminology from the Office of the National Coordinator for Health IT5 and conducted systematic, multifaceted searches to identify peer-reviewed publications from standard bibliographic databases for medicine, business, technology, and the social sciences, as well as non–peer-reviewed publications such as reports from business and governmental agencies. Searches were restricted to English language publications between January 1990 and September 2008.
All types of research studies, reports, and editorials were considered for review, provided that the focus was on HIE in the United States and involved barriers or benefits to ambulatory primary care practices or physicians. In addition, for non–peer-reviewed literature, the citation had to include primary information; for example, it could not merely summarize a peer-reviewed publication. Authors at each site (see Appendix) independently reviewed abstracts or complete articles to determine whether inclusion criteria were met. Details of the databases, search strategy, and process of article selection are available in the Appendix.
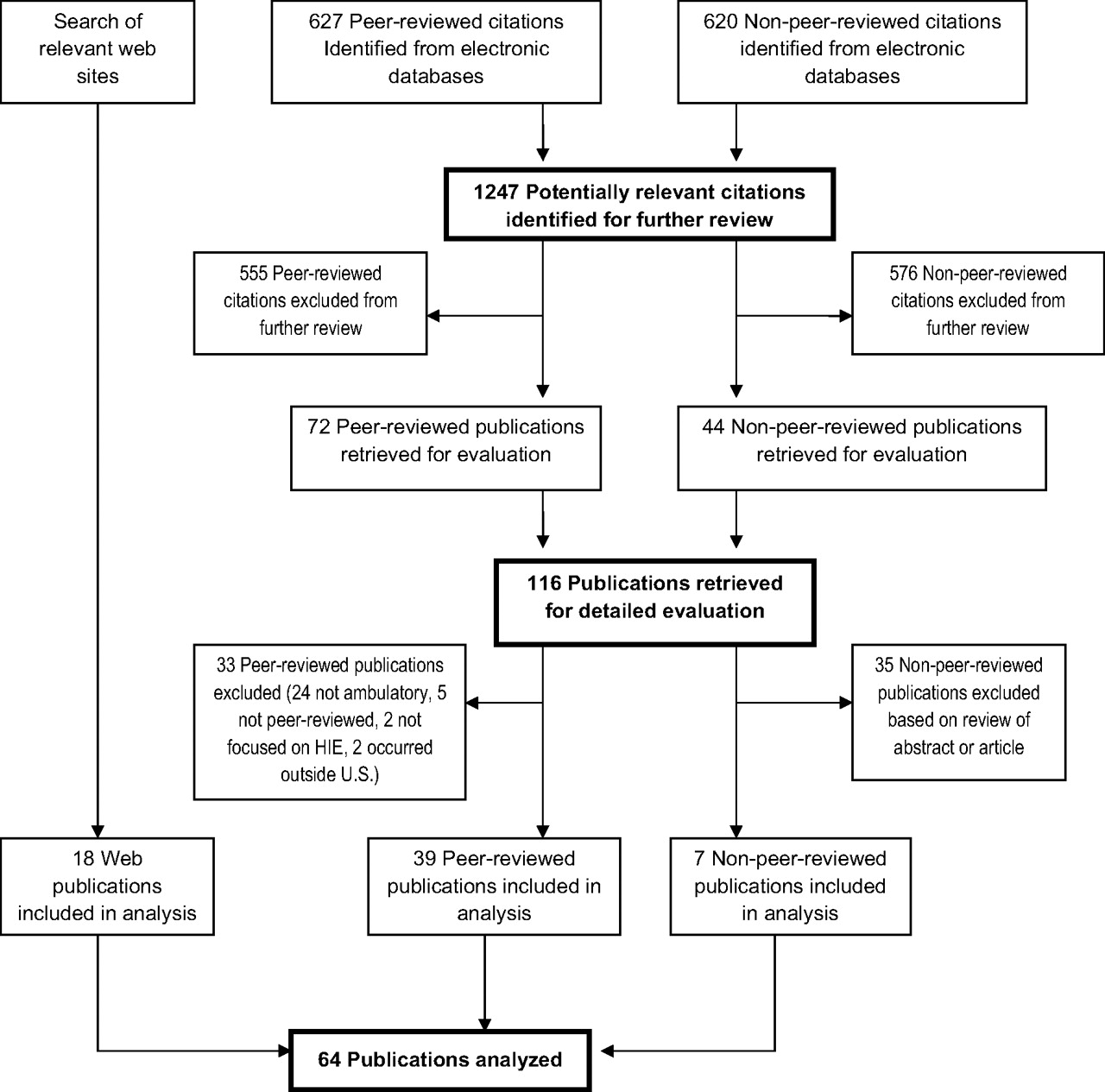
Figure 1 displays the selection process for articles from bibliographic databases and describes the inclusion criteria. Table 1 details the 39 peer-reviewed publications, 7 non–peer-reviewed publications, and 18 web publications included in the systematic review.
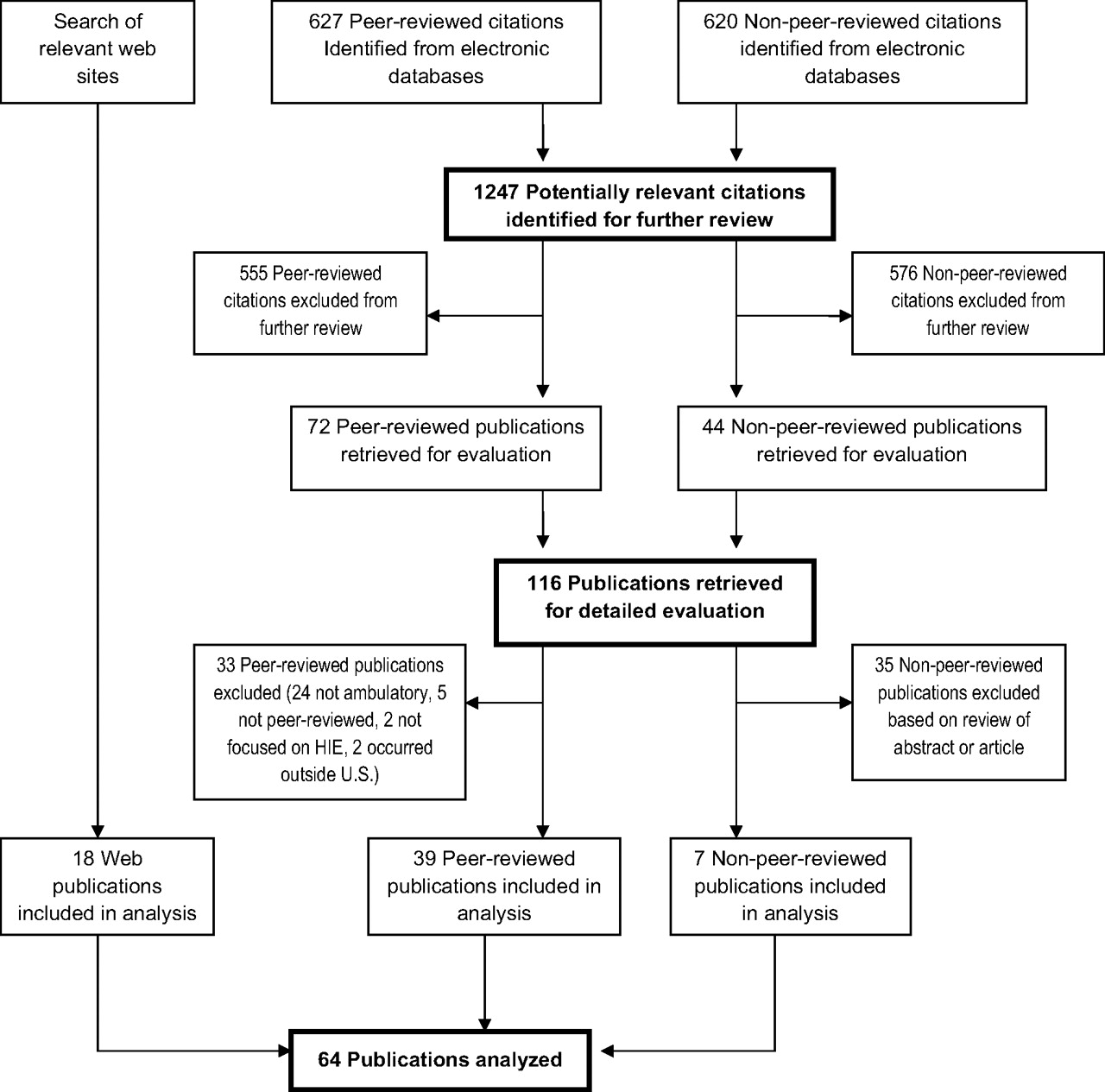
Selection process for publications included in the systematic review. Inclusion criteria were (1) the content dealt with electronic health information exchange (HIE) in the United States; (2) the HIE involved at least one stakeholder in an ambulatory office or primary care practice, or described benefits, barriers, or concerns relevant to ambulatory practices; (3) the publication date was January 1990 through mid-September 2008; and (4) the publication was available in English.
Peer-Reviewed and Non–Peer-Reviewed Publications Included in the Systematic Literature Review
Data Extraction and Analysis
Three authors (PF, SER, LMS) abstracted publications for findings relating to predetermined key issues of stakeholder participation in HIE, benefits, and barriers. Because so few of the studies had prospective or randomized experimental designs, it was impossible to apply standard meta-analysis methodologies. Instead, we systematically identified themes that emerged from the publications and recorded them on a spreadsheet with columns for each of the 3 key issues. For example, organizational characteristics and leadership and governance themes were recorded under stakeholder participation; themes within HIE benefits included improved workflow efficiency, improved quality and safety, and cost savings; themes within HIE barriers included costs, concerns regarding privacy/security/liability, competition, and technical barriers. We then grouped the themes and further analyzed supporting examples within each theme.
Results
Summary Description of the Publications
The oldest publications to meet inclusion criteria were published in 2004 (non–peer-reviewed) and 2000 (peer-reviewed). A notable increase in publications occurred after the Office of the National Coordinator for Health IT was established in 2004.6
Although approximately half of peer-reviewed articles presented original findings (20 of 39; 51%), only 2 reported results from a randomized controlled trial7,8; 8 others reported survey results, 4 described “case studies” of HIEs, 3 reported qualitative studies of HIE participants, and 2 analyzed cost. Expert opinion made up 26% of the peer-reviewed publications in the form of 10 editorials, letters, and commentaries. There were 7 review articles and 2 articles about research methodology, making up 18% and 5% of the total, respectively.
Stakeholder Participation in HIE
Much of the literature about HIE describes the organizations involved. The Veterans Health Administration and its unified EHR exemplify exchange of information within “closed” systems.9 “Open” systems are exemplified by community-based HIE initiatives, known as RHIOs,10 which promote exchange of information among independent entities within a geographic region.11 Open systems face much larger barriers to HIE than do closed systems, including more complicated technical and administrative issues across different technology vendors and organizations, and less clear incentives for stakeholders to share data.9,10,12,13
The failure rate of RHIOs reflects the difficulty of HIE sustainability in open systems. Of RHIOs known to exist in July 2006, nearly one-quarter were defunct by early 2007. Several high profile failures document lessons learned about HIE processes and the importance of alignment with stakeholder values.14,21,24–27 Nevertheless, HIE development is proceeding. A nationwide 2006 survey identified 136 organizations that were either planning or participating in community-based HIE initiatives. By 2007, 32 HIE initiatives were fully operational, and by 2008 an additional 10 initiatives (42 total) had reached the fully operational stage.47
Organizational Characteristics of Successful HIE Initiatives
For successful HIE implementation, a compelling vision needs to be balanced by reasonable expectations and the ability to deliver a demonstrable benefit to providers. Descriptive studies favor an incremental implementation approach that demonstrates early value without pushing stakeholders too fast. For example, the ambitious vision to build a communitywide, interoperable HIE from the ground up was shown to be insupportable in Santa Barbara, California.9,10,16,37,43 By contrast, an incremental building philosophy that capitalized on existing infrastructure and data-sharing efforts showed early promise in Tennessee.2 Examples of achievable early successes include access to test results and clinical notes.14,15 Public health reporting that provides primary care practices with outbreak/epidemic surveillance information, reporting services, or provider/patient notification assistance also provides value.41 Such HIE successes reinforce the altruistic motivation to improve community health care quality.16–20
The long-term success of an HIE initiative depends on its ability to provide services within a sustainable business model (possibly involving membership or user fees).9,10,21,22 For both early adoption and sustainability, a critical mass of data elements and providers along with a preponderance of benefits over barriers may be required to make participation worthwhile for small practices.21,23 Our systematic review identified themes and examples of benefits and barriers to participation in HIE by primary care practices, which are outlined in Table 2.
Benefits and Barriers to Participation of Primary Care Practices in Health Information Exchanges
Benefits
Workflow Efficiency.
HIE has been reported to improve access to test results and other data from outside the practice, to improve referral processes and claims processing, and to decrease staff time required for handling these processes.9,10,33,42–44 Rapid electronic access to test results from outside the practice is a valued benefit of HIEs.10,33,42–44 In the 2008 eHealth Initiative survey, 16 of 42 HIEs (38%) reported improved access to test results.41 A 2-person specialty practice saved 1.5 hours of staff time per week by using an HIE to receive laboratory results.41
A study of web-supported referral applications demonstrated the following efficiencies: (1) reduced return visits to the emergency department, (2) decreased misdirected referrals, and (3) fewer specialty follow-up visits. However, these efficiencies may not translate into reduced costs in small practices because of the multiple roles assumed by support staff.23
Regarding claims processing and billing, the 2008 eHealth Initiative survey showed that 18 of 42 HIEs (43%) were exchanging claims data and 16 (38%) were offering enrollment/eligibility verification.41 The Utah Health Information Network is an example of a standardized communication format for providers and payers, allowing 85% of commercial claims to be paid within 7 days.25 The New England Healthcare EDI Network (NEHEN) has decreased billing write-offs and accounts receivable days since implementing electronic claims processing.44 In addition, 19 of 42 operational HIE initiatives (45%) reported that their efforts had resulted in reduced staff time; 9 (21%) reported decreased support staff as a direct result of efficiencies gained through implementation of the HIE.41 Barriers to achieving such efficiencies include inappropriately redesigned workflow, lack of time to train staff, lack of technical proficiency among staff, and a general lack of an “IT culture.”29
Improved Quality of Care and Patient Safety
A key theme of the literature is the potential of HIE to prevent medical errors and improve safety.18,19,34,45–47 However, much of the evidence for actual improvements in quality and safety is self-reported from small numbers of HIEs. In the 2008 eHealth Initiative survey, 6 of 42 HIEs (14%) reported better care outcomes for patients, 5 (12%) documented reduced patient admissions, and 4 (9.5%) reported decreased prescribing errors. Ten (24%) offered disease or chronic care management services and 8 (19%) reported improved compliance with chronic care and prevention guidelines.41
HIE has been proposed to enhanced patient–provider communication. A personal health record is one example, envisioned as portable, patient-controlled electronic record derived from various sources, including the EHR. Personal health records may be well suited to patients with chronic diseases who are encouraged to be active in self-care, and full access to electronic records could facilitate engagement with their providers and improve quality and safety.45,47
Some HIEs work closely with stakeholders to facilitate quality incentives for providers.26 In 2008, 8 HIEs offered quality improvement reporting for clinicians, and 5 offered it for purchasers or payers.41 However, further development and evaluation are needed to optimize benefits from quality incentive programs and patient safety initiatives facilitated by HIEs in the ambulatory setting.22,47
Cost Savings/Increased Revenue.
The most clear-cut savings resulting from HIE participation have been in reducing the cost of testing agencies that deliver test results.13,39–41 The degree to which providers and their practices experience savings from HIE is unclear. In the 2008 eHealth Initiative survey of fully operational HIE networks, 69% (29 of 42) reported a positive return on investment for their stakeholders in general, whereas only 9 (21%) reported a return on investment for physician practices.41 In addition, 19 of 42 operational HIE initiatives (45%) reported that their efforts had resulted in reduced staff time; 9 (21%) reported decreased support staff as a direct result of efficiencies gained through implementation of the HIE.41 Even so, potential efficiency-driven cost savings (eg, reducing costs of storing paper records and downsizing personnel) may not be realized. Practices may be unable to downsize because staff often perform multiple office tasks.2,3,31
HIE may result in savings for the overall health care system by reducing redundant tests and through better medical decision making that shortens hospital stays. One cost-benefit model suggests that at the highest level of interoperability, nationwide HIE would have a net value of $77.8 billion per year after the first 10 years.3 The model's assumptions, however, have been challenged,23,31 and actual savings from HIE-enabled improvements of care have yet to be demonstrated.
Medicare and some states provide financial incentives to physicians who use health IT.19 HIE facilitates the transfer of quality measures that can result in physician compensation in the form of pay-for-performance incentives.19 Legislative mandates are also potent motivators.34
Barriers
Costs.
Implementation costs are significant barriers to the adoption of IT such as HIEs.28–31 Participation in HIE may be highly dependent on EHR adoption and the use of EHR functionality for storage, documentation, and computerized entry of medical orders linked to clinical decision support.3,32,33 Therefore, the cost of implementing an EHR, estimated at $5,500 to $36,000 per physician,11,34 needs to be considered. Start-up costs include direct costs of hardware, software, and technical assistance, as well as the indirect costs of reduced productivity during the early stages of adoption.23 When looking at the role that cost plays in the adoption of new technology, 79% of primary care providers and 67% of specialists cite cost as a barrier (a significant difference; P < .01).29
For small practices, the major start-up cost for an HIE initiative is likely to be connectivity between the practice's existing clinical information systems and the HIE network.32,35 Ongoing costs of HIE implementation include maintenance expenses and membership or transaction fees.9,10 Costs of implementation could potentially be subsidized by community hospitals, but the physician self-referral law and antikickback laws are perceived barriers.34
Overall, there is uncertainty that practices will obtain a positive return on investment.11,30,34,36 Payers may be the stakeholders most likely to benefit financially from HIE, yet they are noticeably absent from most initiatives.3,10 Because primary care practices are not the main stakeholders to derive economic benefit from HIE,11 the costs they are willing to bear to participate are likely to be small compared with the costs of running the network,25,33,36,37 particularly in rural areas where revenues are constrained and geographic dispersion increases the cost of maintaining HIE networks.12,38
Security/Privacy/Liability.
Privacy concerns are perceived as barriers that must be addressed early in the formation of HIE initiatives.16 Because the United States has a large, private data collection industry governed by a conflicting patchwork of federal and state laws and agencies, federal regulations will need to be modified to encourage secure data exchange in the Nationwide Health Information Network.34,48 Because 76% of patients are somewhat or very concerned about the privacy of their personal health information (PHI),48 patients’ concerns about sharing their PHI also need to be addressed.11,12 Concerns include the unauthorized sharing of “super confidential” information about a patient's mental health, chemical dependency, and genetics; medical identity theft; and fear of discrimination based on health-related conditions.3,48
Ownership of health information is another key issue. Two decades ago, provider resistance to relinquishing patient data to a centralized database contributed to the failure of community health information networks.9 The more popular contemporary approach is a decentralized and federated model for HIE, where ownership of PHI remains in the hands of patients, providers, and insurers.49 Even so, HIE by definition results in greater transparency, which some providers fear may expose them in a negative light.23 Trust in fellow stakeholders and in governance and security policies, as well as the establishment of rules regarding access to and use of data, are important for overcoming this barrier.14,25
Liability concerns center around providers not acting on external data made available through HIE, or for acting on external data that is inaccurate. There is scant legal precedent to offer guidance about the liability of a physician who acts on clinical information made available in such situations.13
Leadership/Strategic Planning/Competition.
Almost two thirds of primary care physicians surveyed in 2006 cited the lack of a strategic plan as a barrier to health IT implementation.34 The lack of business and medical personnel with the informatics training and expertise to develop the strategic plans may be a bottleneck in HIE efforts.34,47 In addition, leadership must counter resistance stemming from fears that IT systems increase physicians’ workload and administrative burdens,50 that physicians have insufficient knowledge34 and insufficient time29 to learn new technologies, and that the benefits of HIE are oversold.11 Once HIEs are implemented, however, physicians are likely to access information they deem clinically useful and have also been shown to comply with mandates, eg, required electronic signatures for inpatient records.9
Competition can create conflict and misalignment of incentives that become a barrier to communitywide HIE.22 By definition, a communitywide HIE effort “requires competing and adversarial parties to collaborate and share their most valued asset: patients and their data.”9 For example, hospital executives may perceive that the benefits of a RHIO accrue to the community while providing no return for the hospital's investment of resources.9 The fragmented and competitive US health care system provides few offsetting incentives for sharing clinical data.34
The perspective of insurers is illustrative. Although insurers may reap financial benefits from HIE-generated improvements in quality and efficiency, a health care system with multiple competing insurance plans creates a “first-mover disadvantage,” where the first insurance plan to subsidize a health IT innovation will benefit its competitors as well.23
Furthermore, some health care organizations have already invested considerable resources in the development of electronic data sharing to gain competitive advantage. Broader HIE in the community may erode this advantage and may be opposed by those who already have effective data sharing.39
Nonetheless, providers with sufficient market share may feel competitive pressures to participate in HIE if participation is necessary to serve customers and address gaps in care delivery.21,39 Provider networks have demonstrated that competitive pressures and potential conflicts of interest can be overcome, allowing clinical data and best practices to be shared to improve care.25
Technical Barriers.
The lack of interoperability between proprietary EHR systems is currently a significant technical barrier encountered by communitywide HIEs, and the lack of nationally recognized standards for data codes, storage, and retrieval is one root cause. The Department of Health and Human Services has encouraged adoption of nationwide standards68 to overcome known disagreements and competition among vendors and other stakeholders.47 Proposed solutions include federal mandates47 and the concept of a common framework49 that provides standards and procedures that allow systems to exchange information, regardless of whether both support highly coded data. The Health IT for Economic and Clinical Health Act contained within the 2009 ARRA established the Health IT Policy Committee and the Health IT Standards Committee, both of which have been charged with making recommendations for policies, technical standards, and certification criteria for a nationwide, interoperable health IT infrastructure.69 Experts warn that the converse—the outgrowth of heterogeneous initiatives—may lead to the possibility that many well-intentioned and locally successful networks will be unable to exchange data.49
Discussion
Primary care plays a major role in the US health care system, so clearly it is desirable for the potential benefits of HIE to extend not only to large organizations, but to small primary care practices as well. From the perspective of the small primary care practice, however, the overall balance sheet of benefits versus barriers remains an open ledger.
At this time, the barriers to adoption of HIE by small practices are significant and include financial and technical barriers as well as concerns about security breaches, liability, and competitive disadvantages. HIE leaders will need to meet these barriers with specific solutions for financial and technical support, as well as a clear and compelling vision of benefit.
Financial incentives for the meaningful use of EHRs are one attempt to address the cost barrier and encourage more practices to acquire technologies that can form the basis for broader HIE. Since this literature review was concluded there has been ongoing progress in defining meaningful use and in plans for Medicare and Medicaid to provide incentive payments to eligible professionals and hospitals that are meaningful users of certified EHRs.70 For providers, this could take place as early as January 2011. The Health IT for Economic and Clinical Health Act will fund a variety of programs that will give technical support and training to providers through Health IT Regional Extension Centers and will also foster the development of HIE within states.71 Finally, technical barriers are being addressed by the development of an initial set of standards, implementation specifications, and certification criteria for EHRs, which were released in the form of an interim final rule in January 2010.72
Regarding known benefits of HIE to primary care practices, our review of the literature identified improved access to test results as the clearest early benefit, with good evidence that HIEs can improve the efficiency with which practices process test results. The evidence that HIE improves the quality and safety of care is more limited, yet it is certainly reasonable for practices to conclude that speedier access to clinically useful information will benefit patient care and prevent errors.
We recognize some limitations in this literature review. First, we were unable to search by MeSH terms because none existed for HIE. We used a comprehensive set of text word searches in an extensive set of bibliographic databases; however, it is possible that some publications were omitted because the term health information exchange was not used and alternative terms were not captured in our search. Second, we limited our search to English-language publications and did not search EMBASE. Finally, our search of the Internet was, by necessity, focused on the most respected and informative websites; a complete search of the web would be boundless.
Conclusion
Overall, our literature review helps to identify the key issues that will need to be addressed for HIE to be broadly adopted and for the Nationwide Health Information Network to become a reality. As HIE initiatives and pilot projects proliferate, there is a pressing need for them to be formally evaluated with research methods that will provide robust evidence about the financial impacts and actual efficiency, quality, and safety gains that are achieved.
Appendix: Databases, Search Strategy, and Process of Article Selection
The literature searches included the following databases: Medline; AMED; CINAHL; ISI Web of Knowledge (Science Citation Index or Web of Science); EBSCO Host (Academic Search Premier, Master File Premier, Business Source Premier, Corporate ResourceNet, and McClatchy-Tribune Collections); Econ Lit; Engineering Village; Social Science Abstracts; and PAIS International and ProQuest.
The Minnesota team (PF and Raymond Boyle, PhD, research assistant for the literature review) analyzed peer-reviewed literature and the Colorado team (LS and SR) analyzed the non–peer-reviewed literature. Both teams consulted medical librarians regarding appropriate databases and search algorithms.
Databases were searched using key words “health information,” “health information exchange,” “health data exchange,” “regional health information organization,” and “RHIO.” Boolean operators, wild cards, and truncation symbols were used to increase search sensitivity or specificity. Both searches were restricted to English-language publications between January 1990 and September 2008. A manual search of reference lists identified additional relevant publications.
Non–Peer-Reviewed Process for Article Retrieval
A list of relevant websites was compiled with assistance from experts from the Agency for Healthcare Research and Quality and the Colorado Regional Health Information Exchange. Websites were reviewed by (1) searching using the site's search tool, (2) manually browsing relevant navigation tool bars and links, and (3) browsing the sitemap.
Peer-Reviewed Process for Article Retrieval
Searches in Ovid (including Medline, AMED, and the Cochrane Database of Systematic Reviews) produced 195 unduplicated citations. Searches in other databases retrieved 824 citations from the Web of Knowledge, 524 for the 3 EBSCO host databases (including CINAHL), and 868 from Engineering Village. To further refine the search, given the large number of citations, we limited to the predetermined areas of interest, ie, barriers or obstacles and benefits. Within these limits we retained 88 citations from the Web of Knowledge, 269 from the 3 EBSCO host databases, and 75 from Engineering Village (a total of 432 citations). Two investigators reviewed the titles and abstracts of 627 citations (195 from Medline and 432 from other databases). Duplicates were eliminated and unduplicated citations were judged for inclusion. If there was disagreement about whether the citation met inclusion criteria, the full text was reviewed and the decision to include or exclude was made by consensus. A total of 72 citations remained, with publication dates ranging from 1998 to 2008.
Acknowledgments
The authors thank Elizabeth Staton for her writing assistance.
Notes
This article was externally peer reviewed.
Funding: Support was provided by Agency for Healthcare Research and Quality contracts HHSA290200710010-2 and HHSA2902007100008-3. The Agency for Healthcare Research and Quality project officer approved the study design, consulted on definitions and literature search strategies, and reviewed and provided feedback on the manuscript.
Conflict of interest: none declared.
- Received for publication August 10, 2009.
- Revision received April 8, 2010.
- Accepted for publication April 15, 2010.
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- The Impact of Community Health Information Exchange Usage on Time to Reutilization of Hospital Services
- Late adopters of the electronic health record should move now
- Physician leadership and health information exchange: literature review
- Accelerated Adoption of Advanced Health Information Technology in Beacon Community Health Centers
- Despite The Spread Of Health Information Exchange, There Is Little Evidence Of Its Impact On Cost, Use, And Quality Of Care
- Assessing the efficacy of the electronic patient record system EDeR: implementation study--study protocol
- The Words We Use, the Procedures We Do, and How We Change (Medical Care Information for Family Physicians)