
Abstract
Pregnancy is associated with many physiologic and hormonal changes along with changes in sleep architecture, placing pregnant women at risk for the development of sleep-disordered breathing or worsening of preexisting sleep apnea. Snoring, the most common symptom of sleep-disordered breathing, is markedly increased during pregnancy. The exact prevalence of obstructive sleep apnea in pregnant women is unknown. Because the apneic episodes are commonly associated with oxyhemoglobin desaturations, the combination of obstructive sleep apnea and pregnancy can be potentially harmful to the fetus given the low oxygen reserves during pregnancy. Obstructive sleep apnea has been associated with an increased risk of hypertension among the general population, and this raises the possibility of its association with gestational hypertension and preeclampsia. In this clinical review, we discuss the physiologic changes of pregnancy that predispose pregnant women to the development of obstructive sleep apnea and the effects of sleep-disordered breathing on pregnancy outcomes. We also review the recommendations regarding evaluation for sleep apnea and treatment options during pregnancy and postpartum.
Sleep-disordered breathing (SDB) includes snoring, upper airway resistance syndrome, and obstructive sleep apnea (OSA)-hypopnea syndrome. OSA-hypopnea syndrome is characterized by recurrent episodes of upper airway collapse and obstruction during sleep and is associated with recurrent oxygen desaturations and arousals from sleep. These disorders represent a continuum of SDB, with snoring at one end of the spectrum and OSA-hypopnea syndrome at the other end. The exact prevalence of OSA among pregnant women is unknown. The prevalence of OSA is estimated to be 5% to 6% among women of reproductive age.1
Apnea is defined as the complete cessation of airflow for a minimum of 10 seconds. Apneas are usually associated with oxygen desaturations or sleep fragmentation (arousals). There is disagreement regarding the definition of hypopnea. Per the American Academy of Sleep Medicine Manual for the scoring of sleep and associated events,2 a ≥30% reduction in airflow associated with ≥4% drop in oxygen saturation or, alternately, a ≥50% reduction in airflow associated with a ≥3% desaturation or associated with an electroencephalogram arousal is considered a hypopnea. Respiratory effort-related arousal is the sequence of breaths lasting at least 10 seconds characterized by increasing respiratory effort leading to an arousal from sleep that does not meet criteria for an apnea or hypopnea. Respiratory effort-related arousals suggest the presence of upper airway resistance syndrome. The average number of apneas and hypopneas per hour of sleep is called the apnea-hypopnea index (AHI), and this information is obtained from overnight polysomnogram (sleep study). OSA-hypopnea syndrome is diagnosed when a patient has clinical symptoms in conjunction with an AHI of >5 events per hour.
Symptoms and signs most suggestive of OSA include habitual snoring, witnessed apneas, gasping and choking sensations during sleep, large neck (>16 inches in a woman of normal height), and hypertension. During the day, patients often complain of nonrefreshing sleep, excessive daytime sleepiness, fatigue, impaired concentration, and personality changes. However, these daytime symptoms are less specific, especially in pregnant women who experience high rates of disturbed sleep and diminished daytime functioning for reasons other than SDB.
Effect of Pregnancy on Sleep-Disordered Breathing
Physiologic changes of pregnancy, including progressive weight gain and upward displacement of the diaphragm, may predispose women to OSA. Estrogen and progesterone levels rise significantly during the course of pregnancy. Estrogen induces hyperemia, nasopharyngeal mucosal edema,3 and vasomotor rhinitis,4 which can lead to a narrowing of the upper airway with increased resistance to airflow. Nasal obstruction, especially chronic nocturnal nasal congestion, has been shown to be an independent risk factor for SDB in the general adult population.5,6 Hence it is plausible that upper airway congestion secondary to estrogen-mediated mechanisms and/or physiologic hypervolemia of pregnancy may increase the risk of SDB among pregnant women. Reduced upper airway dimensions, which is a risk factor for SDB, has been demonstrated among women in the third trimester of pregnancy.7,8 Progesterone may have some protective effect because it enhances respiratory center sensitivity to CO2,9 thereby increasing respiratory drive and minute ventilation. Increased ventilatory drive with resultant respiratory alkalosis has been postulated to cause instability in the respiratory control pathways, thereby predisposing patients to central sleep apneas,10 but whether a similar effect is seen in pregnant women is uncertain. Frequency of central apneas may also be augmented by the increased stage 1 nonrapid eye movement sleep and sleep fragmentation that happens in late pregnancy.11,12 In keeping with the increased respiratory drive of pregnancy, there is increased diaphragmatic effort leading to greater suction pressures at the level of upper airway, which can potentiate upper airway collapse.13,14 Upward displacement of the diaphragm during pregnancy decreases the functional residual capacity by 20%15 in addition to the normal decline of functional residual capacity during sleep. This will decrease maternal oxygenation, further compounding the increased alveolar-arterial oxygen gradient found during pregnancy.16 Because of a reduction in functional residual capacity, the caudal traction on the trachea and pharynx exerted by lung inflation decreases, thereby enhancing the collapsibility of the pharynx;17 however, it is unclear whether this effect occurs in pregnant women. In addition, there is increased small airway closure at lung volumes greater than functional residual capacity, especially in the late pregnancy,18 resulting in ventilation-perfusion mismatch. All of these changes can lead to a reduction in maternal oxygen reserves. Episodes of apnea and hypopnea coupled with low maternal oxygen reserves may possibly increase the risk of maternal hypoxemia and compromise oxygen delivery to the fetus.
There are some protective mechanisms against SDB during pregnancy. Apart from the above-mentioned increased minute ventilation by progesterone, postural changes during sleep and changes in sleep architecture may protect pregnant women from SDB. By late pregnancy, most women tend to sleep in the lateral posture, which decreases the frequency of OSA events. Rapid eye movement sleep decreases in late-stage pregnancy;11,19 this is protective against SDB because obstructive events are more common during this sleep stage. Rightward shift of oxyhemoglobin dissociation curve during pregnancy enhances oxygen delivery to the placenta,20 compensating for the low maternal oxygen reserves.
Sleep-Disordered Breathing in Pregnant Women
The prevalence of OSA is estimated to be 5% to 6% among women of reproductive age;1 however, its prevalence in pregnant women is unknown. Sleep apnea during pregnancy was first reported in 1978 by Joel-Cohen et al,21 and until the turn of the twentieth century, the literature about SDB during pregnancy consisted largely of case reports.22,23 Research studies that evaluated SDB during pregnancy were limited by small sample sizes and inherent limitations of study design to draw definite conclusions. Many studies were based on questionnaires24,25 and were limited by a lack of polysomnographic confirmation of sleep apnea. All of these studies indicate that snoring is common during pregnancy, especially among obese women. Although snoring is the most common symptom for OSA, it is less specific than other symptoms like witnessed apneas and choking sensations during sleep.26,27 Tables 1 and 2 summarize the research studies that have evaluated sleep disordered breathing in pregnant women.
Research Studies Evaluating Sleep-Disordered Breathing Among Pregnant Women
Research Studies Investigating Sleep-Disordered Breathing and Gestational Hypertension/Preeclampsia
Sleep-Disordered Breathing and Adverse Pregnancy Outcomes
SDB had been proposed as a risk factor for adverse maternal-fetal outcomes.42 Numerous case reports described adverse pregnancy outcomes in pregnant women with OSA, eg, fetal heart rate abnormalities associated with maternal apneic episodes,21 fetal growth retardation,21,22,43,44 fetal death,45 pulmonary hypertension,46 gestational diabetes mellitus,22,23,47 and preeclampsia.23,43,48,49 Some observational studies also suggested that SDB was associated with adverse pregnancy outcomes; however, other studies did not find a significant association. Most of the studies were limited by small sample size and an absence of polysomnographic confirmation of OSA, resulting in inconsistent results. Franklin et al24 suggested that habitual snoring is a risk factor for fetal growth retardation. In their study of 502 pregnant women, incidence of gestational hypertension (14% vs 6%; P < .01); preeclampsia (10% vs 4%; P < .05); and fetal growth retardation (7.1% vs 2.6%; P < .05) were significantly higher in pregnant women with habitual snoring compared with nonsnorers. In contrast, Loube et al28 did not find any increased risk of adverse fetal outcomes among pregnant women who reported frequent snoring. A recent study35 reported that 3 out of 4 pregnant women diagnosed with OSA delivered babies with lower mean Apgar scores and birth weights compared with that of women without OSA. Preliminary results of another study showed that sleep apnea might be a risk factor for gestational diabetes.50 This study analyzed the 2003 Health Care Cost and Utilization Project nationwide inpatient data of all pregnant women (n = 3,979,840 deliveries). Controlling for race, gender, and obesity, sleep apnea conferred twice the likelihood of having gestational diabetes and 4 times the likelihood of having pregnancy-induced hypertension.
Postulation about the association of SDB with gestational hypertension is based on the fact that OSA is an independent risk factor for hypertension among the general population. It has been speculated that intermittent maternal hypoxia induced by SDB could cause placental ischemia, triggering oxidative stress and endothelial activation.40,51 Oxidative stress and endothelial dysfunction are implicated in the pathogenesis of pregnancy-induced hypertension.52 Absence of nocturnal dipping in systolic blood pressure is seen in both preeclampsia53,54 and OSA55–57, suggesting a common link between the two. Because maternal hypoxemia can adversely affect fetal growth and development,58,59 SDB with accompanying hypoxemia and hypertension can result in intrauterine growth retardation. A case-control study showed that preeclamptic women had significantly higher respiratory disturbance index (18.4 vs 8.3; P < .05) and lower endothelial function index (1.5 vs 1.8; P < .05) compared with the control group, suggesting that both SDB and endothelial dysfunction are more likely to occur in pregnant women with preeclampsia.40 However, this study was limited by small sample size and a lack of “gold standard ” methods to evaluate SDB and endothelial dysfunction. Sleep-induced mild upper airway inspiratory flow limitation was commonly noted in preeclamptic women,36,38 and the use of nasal continuous positive airway pressure (CPAP) therapy eliminated the airflow limitation and showed improvements in blood pressure readings.36 These low-frequency inspiratory flow limitations did not meet standard apnea-hypopnea definitions and were not associated with arousals, suggesting that they may be a subtle form of SDB. It is unclear whether the upper airway changes precede the development of preeclampsia or the diffuse edema present in preeclamptic women leads to upper airway edema and inspiratory flow limitation.12 Preeclamptic women with coexisting OSA also demonstrate augmented blood pressure responses to obstructive respiratory events during sleep.39 In summary, only preliminary evidence exists to suggest that SDB confers the risk of hypertensive disorders of pregnancy and is associated with adverse maternal and fetal outcomes.51
Evaluation of OSA During Pregnancy
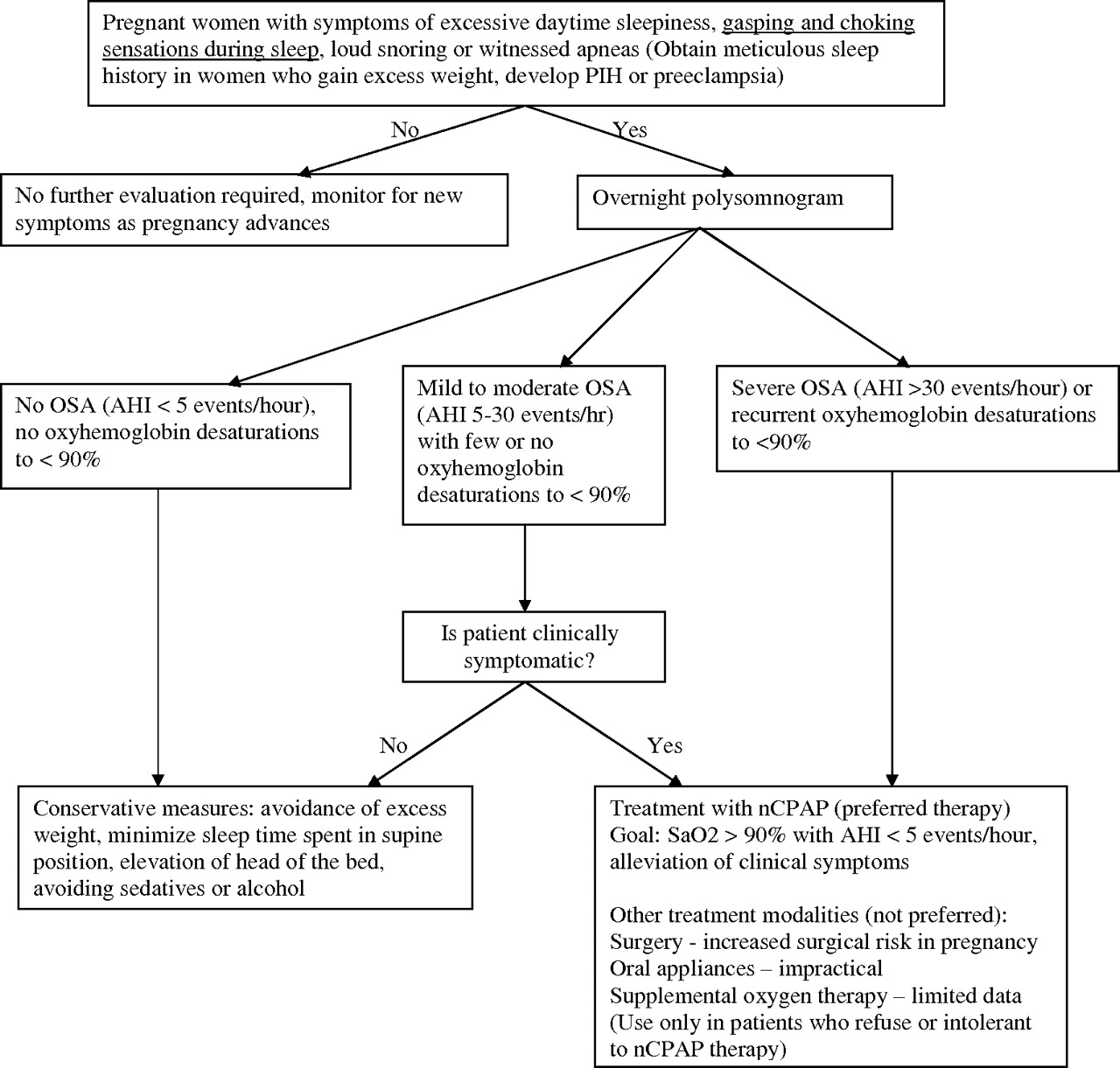
There are no specific guidelines for screening pregnant women for OSA because the data are limited in this population. Pien and Schwab51 have proposed that pregnant women with excessive daytime sleepiness, loud snoring, and witnessed apneas should be evaluated for OSA with overnight polysomnography (strength of recommendation, C). The excessive daytime sleepiness should not be explained by simple insufficient sleep caused by other stresses created by the pregnancy (eg, pain). It would also be prudent to obtain a meticulous sleep history for women with preexisting obesity and a large neck size who develop gestational hypertension or preeclampsia. Pien and Schwab51 stated that uncomplicated snoring, pregnancy-induced hypertension, or intrauterine growth retardation alone in the absence of sleep apnea symptoms are insufficient indications for ordering polysomnography. However, Santiago et al60 argued that until the incidence of SDB in normal and complicated pregnancies is defined, the indications for polysomnography in pregnant women should probably be expanded to include those with hypertension, previous babies with unexplained intrauterine growth restriction, and persistent sleep-related symptoms (hypersomnia or insomnia) associated with snoring or obesity (strength of recommendation, C).
Sleep studies among pregnant women can be performed in a manner similar to those performed among nonpregnant women. However, given the preference of pregnant women to sleep in the lateral position, it is possible that AHI may be underestimated. There is no evidence to suggest that performing nocturnal polysomnographic studies is difficult in pregnant women. There are multiple studies that have successfully performed nocturnal polysomnograms in pregnant women without difficulty.31,35,39,41
Treatment of OSA During Pregnancy
All pregnant women should follow conservative measures, like the avoidance of excess weight gain, sleeping in a lateral position, elevation of the head end of the bed, and restrained use of sedatives and alcohol (strength of recommendation, C). Treatment guidelines for pregnant women with OSA are similar to that of the general population because data in pregnant women are limited. Data from animal studies demonstrated fetal growth retardation with maternal hypoxia;61–63 an important goal in pregnant women is to avoid maternal hypoxemia51 (strength of recommendation, C). CPAP is the standard treatment for OSA among general population64 (strength of recommendation, A). CPAP is indicated for the treatment of moderate (AHI, 15–30 events/hour) to severe (AHI, >30 events/hours) OSA among the general population64 (strength of recommendation, A). Using the guidelines for the treatment of SDB among the general population as a reference, Pien and Schwab51 recommended that pregnant women with severe sleep apnea (AHI, >30 events/hour); mild-to-moderate sleep apnea (AHI, 5–30 events/hour) with clinical symptoms; or recurrent oxyhemoglobin desaturations <90% should receive treatment (strength of recommendation, C). Although there are theoretical concerns about the ability of CPAP to decrease cardiac output, clinically it is unlikely to occur in individuals with normal cardiac output.65 CPAP therapy also has been shown to improve cardiac output while reducing total peripheral resistance in patients with preeclampsia.66 A study involving 12 pregnant women showed that CPAP was safe and well tolerated during pregnancy.31 Two recent studies have also confirmed that nasal CPAP is well tolerated by hypertensive pregnant women.34,41 No adverse events were reported among pregnant women with OSA who were treated with nasal CPAP therapy.22,44–46,49
Oral appliances are impractical during pregnancy in view of multiple sessions needed during a short period of time for optimization of therapy; however, they may be an option, especially in patients who cannot tolerate CPAP. Because of the increased surgical risk during pregnancy, upper airway surgical therapies like uvulopalatopharyngoplasty are not routinely performed. Moreover, uvulopalatopharyngoplasty is not a predictably effective treatment for OSA.67,68 Tracheostomy as a treatment for OSA during pregnancy has been reported in one case47 but it is rarely indicated. Women who refuse to use or are unable to tolerate CPAP can be considered for supplemental oxygen therapy to improve minimal or nadir oxyhemoglobin saturation. However, there is no conclusive evidence to support chronic use of supplemental oxygen as a therapy for OSA69 and it is not recommended as a primary treatment for OSA.70 Moreover, there are potential dangers like prolongation of apnea duration, increased hypercarbia, and ventricular irritability associated with oxygen therapy.69 Pien and Schwab51 also suggested that in pregnant women with preexisting OSA, symptom recurrence should be assessed, especially if there is excess weight gain or gestational hypertension, and a repeat polysomnogram or titration of CPAP pressure is indicated if insufficient treatment is suspected (strength of recommendation, C). Figure 1 summarizes recommendations regarding evaluation and treatment of OSA in pregnant women.

Recommendations for the evaluation and treatment of pregnant women suspected of having sleep-disordered breathing. AHI, apnea-hypopnea index; nCPAP, nasal continuous positive airway pressure; OSA, obstructive sleep apnea; PIH, pregnancy-induced hypertension; SaO2, arterial oxygen saturation. Modified from Pien GW et al.51
Postpartum Management
OSA precipitated by pregnancy usually improves after delivery because nasopharyngeal edema resolves and excess weight is lost. Breastfeeding does not seem to have an effect on the improvement of sleep apnea symptoms during the postnatal period.32 Significant spontaneous improvement in AHI values, minimum oxyhemoglobin saturations, and arousal indices occurred by 3 to 6 months postpartum in a group of 10 women diagnosed with OSA during pregnancy.32 Nasal CPAP therapy was discontinued within 2 weeks of delivery in all the patients. The following recommendations for postpartum management of pregnancy-associated OSA are based on expert opinion51 (strength of recommendation, C).
Postpartum withdrawal of CPAP therapy with follow-up for symptom recurrence can be attempted in mild to moderate pregnancy-associated sleep apnea. If symptoms recur, a repeat polysomnogram to assess baseline AHI is indicated.
For severe pregnancy-associated sleep apnea, therapy should be continued and, when weight returns to 10% to 15% of baseline, a repeat polysomnogram should be obtained to establish baseline AHI and any need for continued therapy.
Patients with preexisting OSA can safely return to prepregnancy therapy when their weight returns to 10% to 15% of baseline, with close follow-up for symptom recurrence.
All women with gestational sleep apnea should be monitored closely for symptom recurrence in subsequent pregnancies.
Table 3 summarizes postpartum recommendations for managing pregnancy-associated OSA.
Postpartum Recommendations for Women with Pregnancy-Associated Sleep Apnea51
Conclusions
OSA can complicate pregnancy given the risk factors of weight gain, upper displacement of the diaphragm, and hormonal-induced hyperemia of the nasopharyngeal passages. Preliminary evidence suggests that SDB confers the risk of hypertensive disorders of pregnancy and is associated with adverse maternal and fetal outcomes. There are no specific guidelines for screening pregnant women for OSA. In women with preexisting obesity who develop gestational hypertension or preeclampsia, there should be a high index of suspicion for testing for SDB. Nasal CPAP is the standard treatment in the nonpregnant population but there is a paucity of literature regarding its use among pregnant women. However, all patients should be encouraged to follow conservative measures, eg, elevation of the head of the bed, sleeping in a lateral position, and the avoidance of excess weight gain, alcohol use, and sedative use. Postpartum withdrawal of therapy with close monitoring of symptoms can be attempted, especially if weight returns to baseline.
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: none declared.
- Received for publication March 12, 2008.
- Revision received June 8, 2008.
- Accepted for publication June 17, 2008.
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- Ketamine decreases inflammatory and immune pathways after transient hypoxia in late gestation fetal cerebral cortex
- Sleep-Disordered Breathing and Gestational Diabetes Mellitus: A meta-analysis of 9,795 participants enrolled in epidemiological observational studies
- Women's Physical Health, Mental Health, and Practical Hints for Common Practice Issues