
Abstract
Background: The extent to which adults with mental health disorders in the United States receive opioids has not been adequately reported.
Methods: We performed a cross-sectional study of a nationally representative sample of the noninstitutionalized U.S. adult population from the Medical Expenditure Panel Survey. We examined the relationship between mental health (mood and anxiety) disorders and prescription opioid use (defined as receiving at least 2 prescriptions in a calendar year).
Results: We estimate that among the 38.6 million Americans with mental health disorders, 18.7% (7.2 million of 38.6 million) use prescription opioids. Adults with mental health conditions receive 51.4% (60 million of 115 million prescriptions) of the total opioid prescriptions distributed in the United States each year. Compared with adults without mental health disorders, adults with mental health disorders were significantly more likely to use opioids (18.7% vs 5.0%; P < .001). In adjusted analyses, having a mental health disorder was associated with prescription opioid use overall (odds ratio, 2.08; 95% confidence interval, 1.83–2.35).
Conclusions: The 16% of Americans who have mental health disorders receive over half of all opioids prescribed in the United States. Improving pain management among this population is critical to reduce national dependency on opioids.
- Analgesics
- Opioid
- Anxiety Disorders
- Cross-sectional Studies
- Mental Health
- Opioid-Related Disorders
- Pain Management
- Prescriptions
- Surveys and Questionnaires
The United States is in the midst of an epidemic of morbidity and mortality due to prescription opioid use.1 Over the past 15 years the number of prescription opioid analgesic medications sold in the United States has quadrupled, yet the amount of pain or disability that Americans experience has remained unchanged.2 The Centers for Disease Control and Prevention reports that from 2000 to 2014, more than 165,000 people have died from overdoses related to prescription opioid use.2 The identification of specific populations that rely heavily on opioids is of strategic importance for risk mitigation efforts. For instance, attention has focused on patients recovering from trauma and surgery, among whom poor coping strategies were associated with long-term reliance on opioids.3,4
Previous studies suggest that adults with mental health disorders (ie, mood and anxiety disorders) are more likely to be prescribed opioids and remain taking them long-term.5⇓⇓–8 For example, adults with mood disorders are nearly twice as likely to use opioids long-term for pain.8 In fact, pain is very common among adults with mental health disorders,9,10 and the relationship between mental illness and opioid use is complex. However, some suggest that mental illness may be a moderator in the relationship between pain and opioid use.5 Despite the increase in the prevalence of mental health disorders11 and the importance of tracking use of prescription opioids nationally, the extent to which U.S. adults with mental health disorders use prescription opioids has not been thoroughly examined. Furthermore, identification of the specific factors that may underpin the association would help clarify the complex relationship between mental health and pain.
Therefore, we used the nationally representative Medical Expenditure Panel Survey (MEPS) to examine the relationship between mental health disorders and prescription opioid use. Because anxiety and depression are the predominate mental health disorders among adults in the United States,11 we focused our attention on these 2 conditions. Our objective was to derive national estimates of opioid use among Americans with mental health disorders and to examine factors associated with such use.
Methods
We performed a cross-sectional study using nationally representative data from the MEPS, a survey of the U.S. noninstitutionalized population that is conducted by the Agency for Healthcare Research and Quality that gathers extensive information on health care utilization (including prescription medications), expenditures, and health status.12 The survey uses an overlapping panel design consisting of a household component, a medical provider component, and an insurance provider component. To avoid potential recall bias, participants are surveyed about past health and health care use at 6-month intervals. Personal and family-level data obtained from the household, medical provider, and insurance provider components are aggregated by the MEPS study team. For this study we used data from the MEPS household component files, including the full-year consolidated, medical condition, and prescription medication files. Because our study used only publically available and deidentified data, it was granted an exemption from institutional board review.
Study Sample
To increase the sample size in order to generate more stable national estimates for subgroups, we appended 2011 and 2013 MEPS data. These survey years were chosen because they were the most recently available at the time of analysis and ensured an adequate sample size. We excluded 2012 data because of duplication of participants due to the overlapping panel design (ie, aggregation of MEPS surveys in adjacent years would result in nonindependence of study participants). A total of 52,000 adults (aged ≥18 years) participated in MEPS in these 2 years (25,465 in 2011 and 26,535 in 2013). After ineligible respondents were removed, such as those who were institutionalized for a period of time during the study, our final analytic sample consisted of 51,891 adults.
Measures
Identification of Adults with Mental Health Disorders
Each MEPS participant is asked to identify any health conditions in 6-month time periods. For those who have a self-reported health condition, trained MEPS staff code conditions using the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes. A special feature of the MEPS is that the health care providers and facilities provide data on MEPS participants' health care use; such data are then cross-referenced with survey responses from the participant. Thus, if a person with a mental health disorder did not self-report having the condition, they would still be identified if they had a clinical diagnosis.
Based on the combination of self-report and administrative clinical data, we identified participants who had a mental health disorder. To do so we used ICD-9-CM codes truncated to the first 3 digits, including 300 (Anxiety, dissociative and somatoform disorders), 311 (Depressive disorder), and 296 (Episodic mood disorders), to identify adult MEPS participants with mental health disorders13 (Appendix Table 1).
Prescription Opioid Use
The MEPS collects detailed data on prescription medications using a unique combination of participant self-report and administrative data obtained from pharmacies. MEPS participants are asked to supply the name of any prescribed medications and the name and location of the pharmacy where they obtained the prescription. Participants provide written permission for the release of pharmacy records. Pharmacies are contacted to obtain records, which detail the date filled, the National Drug Code, medication name, strength of the medication (amount and unit), quantity (package size), and payments by source. To identify meaningful classes of drugs, National Drug Codes are merged to the comprehensive Multum Lexicon crosswalk.14 We used the Multum drug classes for oral “Narcotic analgesics” and “Narcotic analgesics combinations” in order to identify oral prescription opioid medications. In the MEPS prescription medication data, the most common oral opioid prescriptions—which account for approximately 65% of all opioid prescriptions—include hydrocodone with acetaminophen, tramadol, and hydrocodone. Our study was focused on examining the likelihood of receiving prescription opioid medications rather than chronic use; thus we operationally defined an opioid user as an adult who filled ≥2 prescription medications in the calendar year.
To explore the clinical diagnoses associated with prescription opioids, we also examined the top 10 clinical diagnoses for which opioids were prescribed. To collapse ICD-9-CM codes into relevant clinical disorders, the MEPS uses the Clinical Classification Software developed by the Healthcare Cost and Utilization Project.15
Covariates
We extracted a variety of health measures to be used as covariates (Appendix Table 2). The MEPS administers the 12-Item Short Form Survey (SF-12) to participants.16 From these data, we calculated the mean physical component summary (PCS) and mental component summary (MCS) scores of the SF-12 (PCS and MCS scores range from 0 to 100, with 100 indicating the highest level of health). We examined several items of the SF-12 separately as well. We collapsed self-reported health status17 into “excellent, very good, or good” versus “fair or poor.” Because pain is the primary driver of prescription opioid use, we examined the SF-12 item on pain. The item inquires, “During the past 4 weeks, how much did pain interfere with your normal work (including work outside the home and housework)?” We collapsed the response set into none or little (“not at all” or “a little bit”), moderate (“moderately”) or severe (“quite a bit” or “extremely”). Based on a combination of measures of both physical and cognitive limitations, we also calculated the percentage of participants with “any functional limitation,” “physical limitation,” “social limitation,” and “cognitive limitation.” We also identified those who were smokers (current vs never or former). Last, based on all medical conditions (ICD-9-CM diagnosis codes reported in the medical condition files) we generated a comorbidity score. To do so, we applied a modified version of the Charlson Comorbidity Index18 developed by D'Hoore et al.19
We used ICD-9-CM diagnosis codes 303 (Alcohol dependence syndrome), 304 (Drug dependence), and 305 (Nondependent abuse of drugs) to identify study participants with substance abuse disorders. The MEPS inquires about cancer diagnoses; we used these items to identify participants who had cancer. We also identified participants with musculoskeletal conditions using a previously applied approach.20
From the MEPS annual consolidated files, we extracted sociodemographic data for participants in our study, including age, sex, race/ethnicity, marital status, level of education, and health insurance coverage. Age was collapsed into relevant age categories, including young adult (18–44 years), middle-aged adult (45–64 years), and older adult (≥65 years). We also identified those adults who underwent an outpatient surgery, underwent surgery during an inpatient admission, or visited an emergency department specifically related to a physical injury.
Statistical Analyses
Our primary analyses examined the relationship between having a mental health disorder and the likelihood of prescription opioid use. We used simple descriptive measures to examine differences between adults with mental health disorders and those without, restricted to those with specific characteristics (eg, a cancer diagnosis, those self-reporting having severe pain, etc.). The χ2 test was used to compare proportions and an independent t test was used to compare means. A 2-sided P value <.05 was considered statistically significant.
We used logit models to examine the relationship while adjusting for differences, and coefficients from our models were exponentiated to express associations in the form of odds ratios. Covariates in our model included age (continuous), sex, race/ethnicity (non-Hispanic white, non-Hispanic black, Hispanic, other), health insurance coverage (private, public, uninsured), having a usual source of care, self-reported limitation due to pain (little/none, moderate, severe), PCS score (continuous), physical limitation, substance use disorder diagnosis, outpatient surgery use, and inpatient surgery use. Because our operational definition of an opioid user was based on receiving 2 or more prescriptions in the calendar year, we also performed a sensitivity analysis in which we varied our definition to include between 1 and 5 prescriptions and then reexamined associations.
For all analyses we used complex survey design methods to make national estimates, which account for a participant's probability of selection and sampling methodology. Because our study aggregated 2011 and 2013 MEPS data, survey weights were adjusted so that the data represented a single calendar year. Analyses were based on complete case analysis, and we assumed any missing values to be missing completely at random. Analyses were conducted using Stata MP, version 14.0 (StataCorp, College Station, TX).
Results
Among the 239.4 million U.S. adults, we estimate that 38.6 million had a mental health disorder (Table 1 and Figure 1). Of the adults with mental health disorders, 18.7% were opioid users, compared with only 5.0% among those without mental health disorders (P <.001) (Figure 2). We estimate that approximately 115 million opioid prescriptions are distributed each year in the United States, 51.4% (60 million prescriptions) of which are received by adults who have a mental health disorder.
Sociodemographic Characteristics and Health Status of U.S. Adults According to Mental Health Disorder Status and Opioid Use
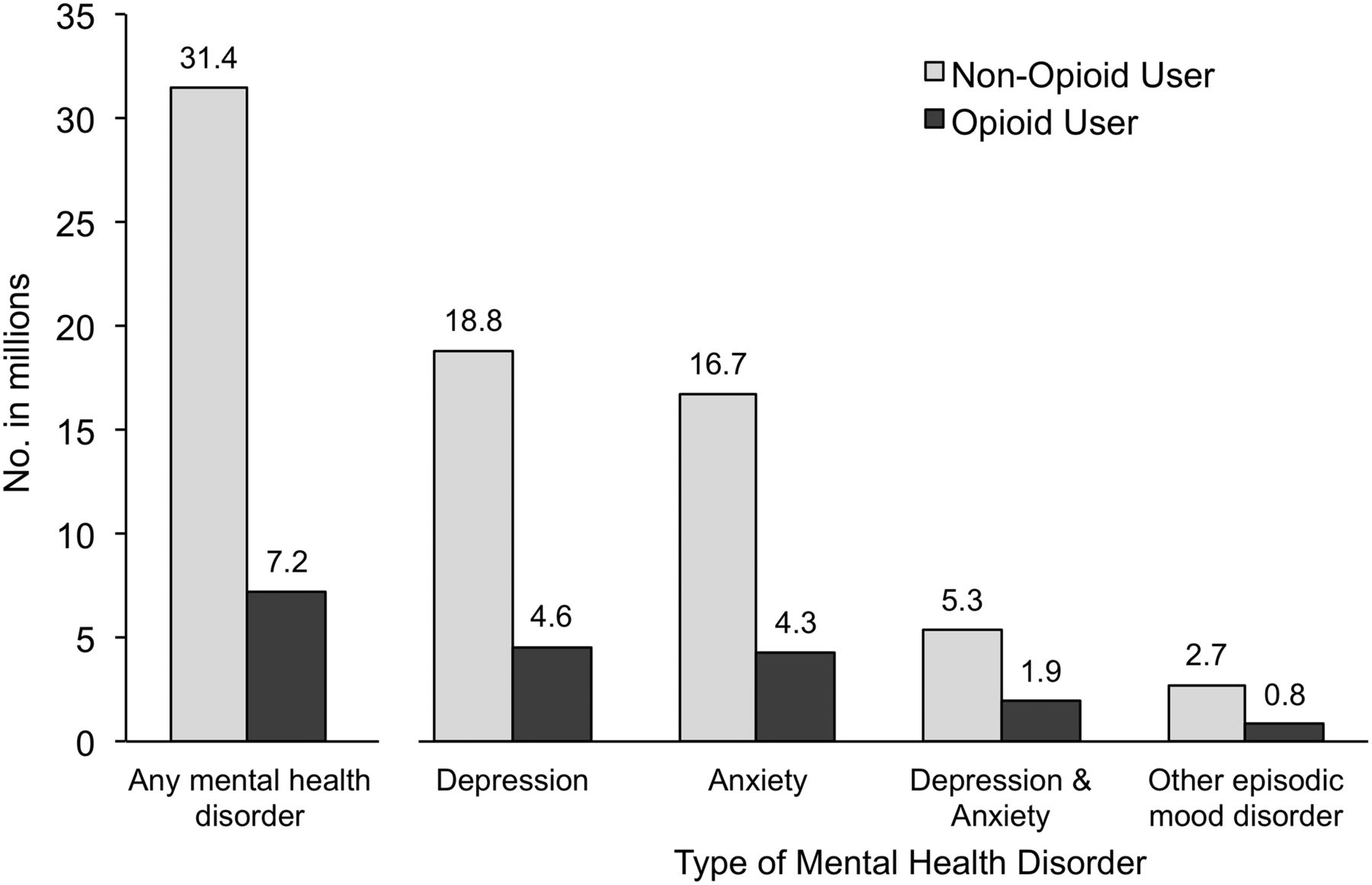
Estimated number of adults with mental health disorders who use prescription opioids in the United States. All estimates are weighted to represent the U.S. noninstitutionalized population.
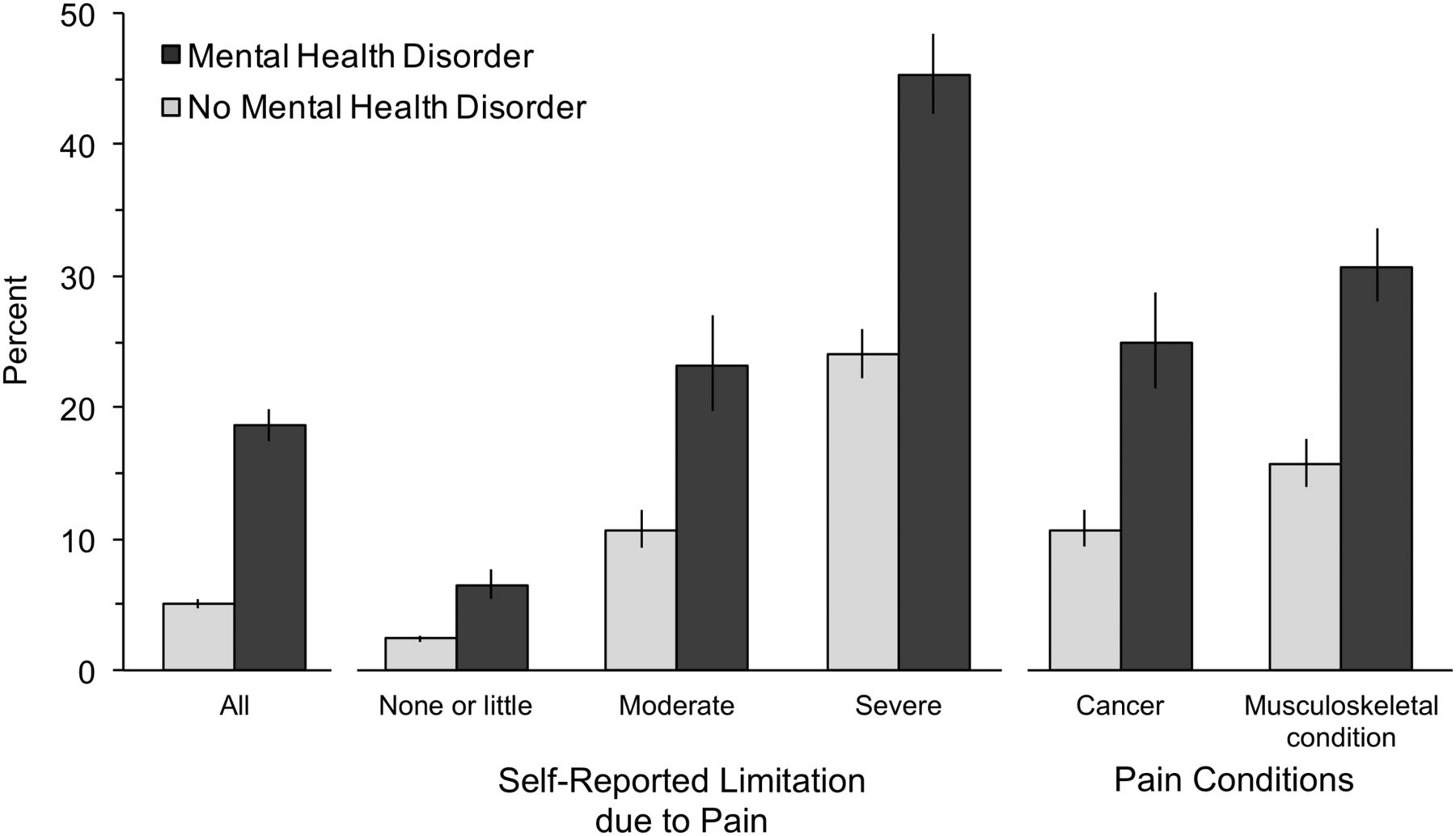
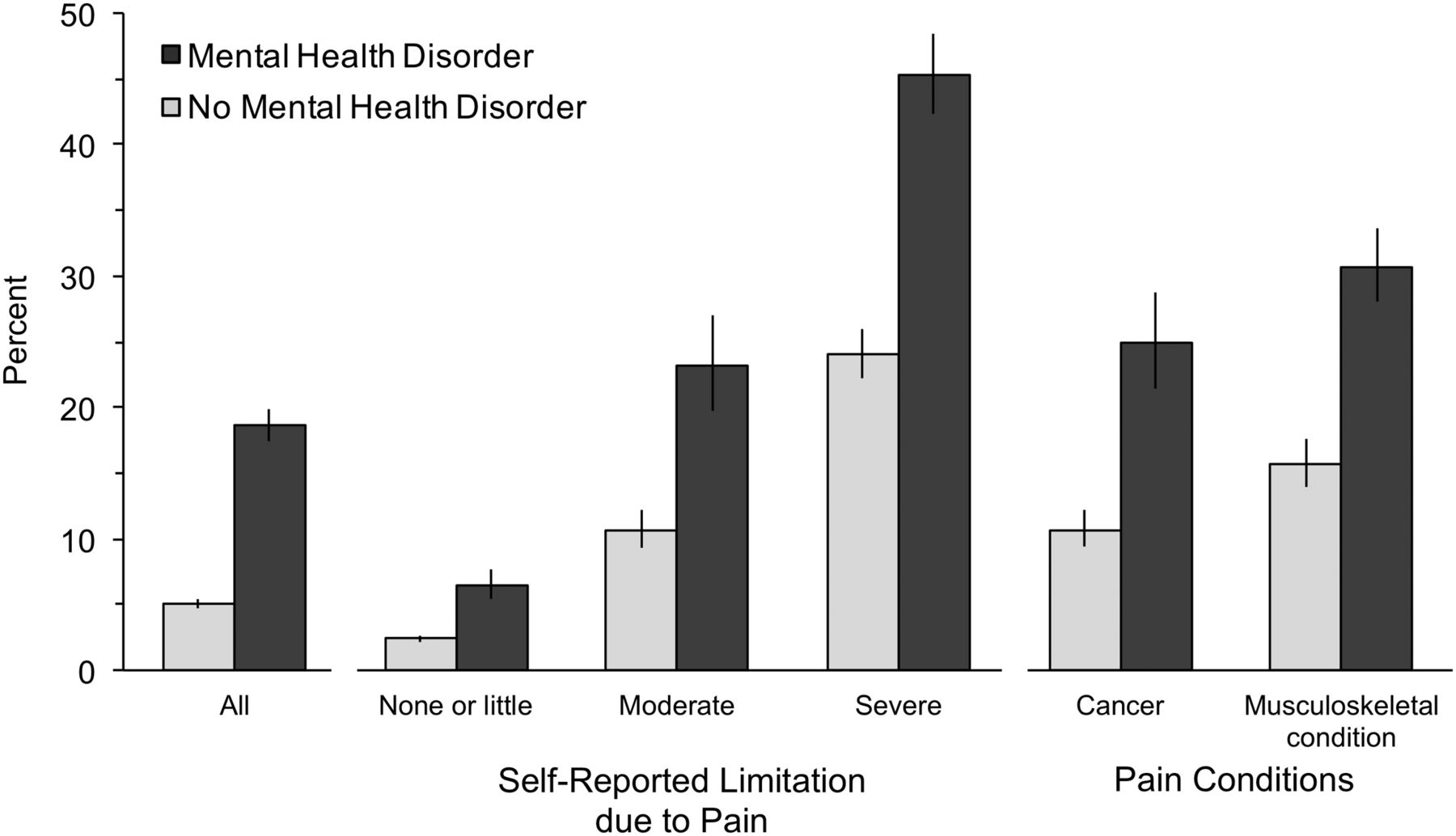
Estimated percentages of U.S. adults with and without mental health disorders who use prescription opioids, according to selected characteristics. All estimates are weighted to represent the U.S. noninstitutionalized population. Error bars represent 95% confidence intervals. Musculoskeletal conditions include all forms of arthritis, and other pain-related conditions.
Characteristics of Adults with a Mental Health Disorder Who Use Opioids
Among adults with mental health disorders, opioid users differed in several ways. Opioid users were older (nearly 75% of opioid users were aged ≥45 years compared with 60% among nonopioid users), more likely to be non-Hispanic white, and completed less educational (P < .001 for all) (Table 1). Comparing opioid users with and without a mental health disorder, those with a mental health disorder were more likely to be middle-aged, female, non-Hispanic white, and divorced, separated, or widowed.
Among adults with mental health disorders, opioid users were considerably less healthy than nonopioid users (Table 1 and Appendix Table 2). The mean PCS score was 33.5 (standard error, 0.50) among opioid users versus 47.7 (standard error, 0.20) among nonopioid users (P < .001). Likewise, among adults with mental health disorders, opioid users had considerably more comorbidities; for instance, 18.1% of opioid users had ≥3 comorbidities, compared with just 6.3% among nonopioid users. Adults with mental health disorders who use opioids also had much higher self-reported pain levels (eg, 60.0% of opioid users reported severe pain compared with only 16.2% among nonopioid users). Among opioid users, those with mental health disorders were less healthy than those without mental health disorders, but the differences were less pronounced.
Opioid Use Among Adults with Mental Health Disorders
Among specific subpopulations based on the level of self-reported pain, cancer diagnosis, and musculoskeletal conditions, the higher percentage of opioid users persisted among adults with mental health conditions compared with those without (P < .001 for all) (Figure 2). Most notable was nearly twice the percentage of opioid users among adults with severe pain (45.3% of adults with mental health disorders were opioid users compared with 24.1% among those without mental health disorders).
The top 10 clinical diagnoses associated with prescription opioids for Americans with mental health disorders included musculoskeletal disorders, poorly defined conditions, or an otherwise missing diagnosis (Figure 3). The top 10 clinical diagnoses we identified among adults with mental health disorders account for 54.0% of the total opioids prescribed to this population, suggesting considerable variation in clinical diagnosis.

Top 10 clinical diagnoses for prescription opioids among U.S. adults who have a mental health disorder. All estimates are weighted to represent the number of prescriptions among the U.S. noninstitutionalized population. The χ2 test was used to compare proportions.
Association Between Mental Health Disorders and Opioid Use
In unadjusted analyses the odds of opioid use was >4 times higher among adults with mental health disorders than among those without (odds ratio [OR], 4.34; 95% confidence interval [CI], 3.93–4.77) (Table 2). After adjusting for sociodemographic characteristics, health status, and use of selected health services, although attenuated, the association persisted: adults with mental health disorders had more than twice the odds of being an opioid user (OR, 2.08; 95% CI, 1.83–2.35). Other notable factors in the fully adjusted model associated with opioid use included having a usual source of care (OR, 1.67), having moderate or severe self-reported pain (ORs, 2.15 and 3.15, respectively), reporting a physical limitation (OR, 1.84), having had surgery (ORs, 2.73 and 3.58 for outpatient and inpatient surgery, respectively), and having a substance abuse diagnosis (OR, 2.42).
Odds Ratios For the Association Between Independent Factors and Prescription Opioid Use
In our sensitivity analyses, all associations persisted when varying our opioid user definition (from 1 to 5 prescriptions/year), and were more pronounced with more stringent definitions of opioid use.
Discussion
Although, previous reports have documented the association between having a mental health disorder and opioid use in specific populations, our study offers several contributions. First, we found that the population of adults with mental health disorders receive more than half of the total opioid prescriptions in the United States. Second, among the nearly 40 million Americans who have a mental health condition, approximately 19% use prescription opioids. Last, higher opioid use among those with mental health disorders persists across key characteristics, including cancer status and various levels of self-reported pain.
Although evidence-based prescribing guidelines are emerging,21,22 there exists a complex interaction of factors related to the patient, provider, and medical and social conditions that ultimately results in the decision to prescribe an opioid.23 Our findings that patients with mental illness are more likely to receive opioid prescriptions across all different levels of pain suggests that there may be additional patient- and provider-related factors specific to those with mental illness that increase the likelihood of receiving prescription opioids. Such a relationship is particularly concerning because mental illness is also a prominent risk factor for overdose and other adverse opioid-related outcomes.24,25 Thus, the expectation would be that physicians would be more conservative with their prescribing behaviors in the setting of mental illness and favor nonopioid alternatives. The ability to identify populations that may use prescription opioids independent of pain would be of strategic importance for mitigating potential risk at a population health level.
The challenge with pain management is that there is no biological measure of pain or objective assessment of efficacy of treatment. The International Association for the Study of Pain adopted a definition of pain that is widely accepted.26 The definition states that pain is “an unpleasant sensory and emotional experience, associated with actual or threatened tissue damage, or described in terms of such.” The definition thus relies on physician interpretation and the subjective experience of the patient. Thus, one could hypothesize that increased opioid use in patients with mental health disorders may be related to a variety of psychological factors that may contribute to an increased subjective experience of pain or to increased likelihood of using opioids irrespective of pain level.5
Our finding that approximately 19% of adults with mental health disorders use prescription opioids aligns with what is to our knowledge the only other article that used nationally representative data to examine this relationship. Halbert and colleagues8 examined patients with pain-related conditions and found those who had mood disorders were more likely to initiate opioid use than those without mood disorders: 19.3% of patients with pain and mood disorders initiated opioid use, compared with 17.2% of patients with pain without mood disorders. Evidence indicating an increased risk of depressive symptoms in patients receiving chronic opioids may raise concerns regarding reverse causality.27 The relationship between mental health disorders and pain is also likely bidirectional, with improvements in pain leading to improvements in mental health symptoms and vice versa.28 Furthermore, some evidence indicates that optimizing depression and pain treatment can improve outcomes in both areas for patients seen in primary care.29 Although the relationship between mental health disorders, pain, and opioid use is complex, we found that having a mental health disorder is associated with increased opioid use even after controlling for a wide array of other demographic and clinical risk factors, including substance abuse. The high prevalence of mental health disorders coupled with prescription opioid use suggests that this population is critical to consider when addressing the issue of opioid use from a health system or policy perspective. Although a number of important steps are already underway to address opioid use in this country, such as the recent Centers for Disease Control and Prevention opioid prescribing guidelines,22 improving treatment of comorbid mental health disorders and pain will be an important focus when trying to reduce the overall negative impacts of opioid use on patients and communities.
Study Limitations
Our study has several limitations that must be acknowledged. First, our study used a cross-sectional, observational design and therefore is not intended to demonstrate a cause–effect relationship between having a mental health disorder and using opioids. Thus we cannot rule out the effects of residual confounding nor potential reverse causality. However, with regard to the latter, recent evidence from longitudinal analyses suggests opioid-naïve patients with mood disorders are in fact more likely to initiate prescription opioids and to transition to longer-term opioid use than those without a mood disorder.8 Second, because we focused on determining whether clinical treatment varies by mental health disorder status, our study only examined prescription opioid use and therefore neglects any concurrent illicit medication use. Third, we investigated the association between mental health disorders and opioid use among noninstitutionalized U.S. adult citizens. Therefore, findings among children or institutionalized adults may differ. Last, the MEPS data on health care utilization and expenditures are self-reported by patients, potentially causing inaccuracies; however, the MEPS attempts to correct self-reported errors by verifying response data with the participant's health care and insurance providers.
Despite these inherent limitations, our study offers valuable insights regarding opioid use among Americans with mental health disorders. Although the relationship between mental health and pain management is complex, we find that as a population, adults with mental health disorders receive more than half of all opioid prescriptions distributed each year in the United States. This finding warrants more research to understand further the association between mental health disorders and prescription opioid use, and to promote safer opioid use among this population.
Appendix
Medical Expenditure Panel Survey Participants with Mental Health Disorders According to International Classification of Diseases, Ninth Revision, Clinical Modification Diagnosis Codes
Health Status of U.S. Adults According to Mental Health Disorder Status and Opioid Use
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: none declared.
To see this article online, please go to: http://jabfm.org/content/30/4/407.full.
- Received for publication March 2, 2017.
- Revision received March 6, 2017.
- Accepted for publication March 10, 2017.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Opioids Diminish the Placebo Antidepressant Response: A Post Hoc Analysis of a Randomized Controlled Ketamine Trial
- Examining non-linearity in the association between age and reported opioid use in different socioeconomic strata: cohort study using Health Survey for England waves from 1997 to 2014
- New, long-term opioid use after lung cancer surgery is associated with reduced 2-year survival: a retrospective population-based cohort study in South Korea
- Anxiolytic and sedative polypharmacy among US opioid users: a cross-sectional study
- Mental Health and Benzodiazepine Use Among Patients on Chronic Opioid Therapy
- Opioid-related diagnoses and HIV, HCV and mental disorders: using Pennsylvania hospitalisation data to assess community-level relationships over space and time
- Observational retrospective study of the association of initial healthcare provider for new-onset low back pain with early and long-term opioid use
- Multimodal Local Opioid Prescribing Intervention Outcomes in Chronic Noncancer Pain Management
- Opioid and benzodiazepine prescription among patients with cirrhosis compared to other forms of chronic disease
- How acute pain leads to chronic opioid use
- Content Usage and the Most Frequently Read Articles of 2017
- In This Issue: Opiates, Tobacco, Social Determinants of Health, Social Accountability for Non-Profit Hospitals, More on PCMH, and Clinical Topics