
Abstract
Introduction: The steady increase in the use of computed tomography (CT) has particular concerns for children. Family physicians must often select pediatric imaging without any decision support. We hypothesized that point-of-care decision support would lead to the selection of imaging that lowered radiation exposure and improved guideline congruence.
Methods: Our double-blind, randomized simulation included family physicians in the Military Health System. Participants initially reviewed a pediatric hematuria scenario and selected imaging without decision support. Participants were subsequently randomized to either receive imaging-appropriateness guidelines and then estimated radiation exposure information or receive estimated radiation information then guidelines; imaging selections were required after each step. The primary outcome was the selected imaging modality with point-of-care decision support.
Results: The first arm increased CT ordering after viewing the guidelines (P = .008) but then decreased it after reviewing radiation exposure information (P = .007). In the second arm radiation information decreased CT and plain film use (P = not significant), with a subsequent increase in ultrasound and CT after the guideline presentation (P = .05).
Conclusions: Decision support during a simulated pediatric scenario helped family physicians select imaging that lowered radiation exposure and was aligned with current guidelines, especially when presented with radiation information after guideline review. This information could help inform electronic medical record design.
The increased use of computed tomography (CT) may unnecessarily expose children to ionizing radiation.1 Risks associated with radiation exposure are greater in children because of their longer life span and greater radiosensitivity.2 Given the need to weigh risks and benefits before any medical test,3 physicians need to better understand doses of radiation associated with common imaging modalities.4 In current practice up to 40% of CT scans ordered are unnecessary.5,6 As a result, imaging guidelines7 and clinical decision support systems5 have been developed to improve appropriate use of medical imaging. To date, these initiatives have been inconsistently adopted and are largely unavailable for children.8 Of those available, the American College of Radiology (ACR) Appropriateness Criteria are evidence-based imaging guidelines that address imaging recommendations for different clinical scenarios, including several that involve pediatric patients. To our knowledge, no decision support products to encourage appropriate medical imaging within the clinical workflow are currently in use.
Building on our previous research,9 this study examined how decision support, in the form of estimated radiation exposure coupled with current imaging guidelines, influenced family physician selection of pediatric imaging modalities. We hypothesized that decision support information, and the order in which data were presented, would impact physician choice of imaging modality. This would ideally enhance the use of guideline-recommended imaging and lower estimated radiation exposure in pediatric patients.
Methods
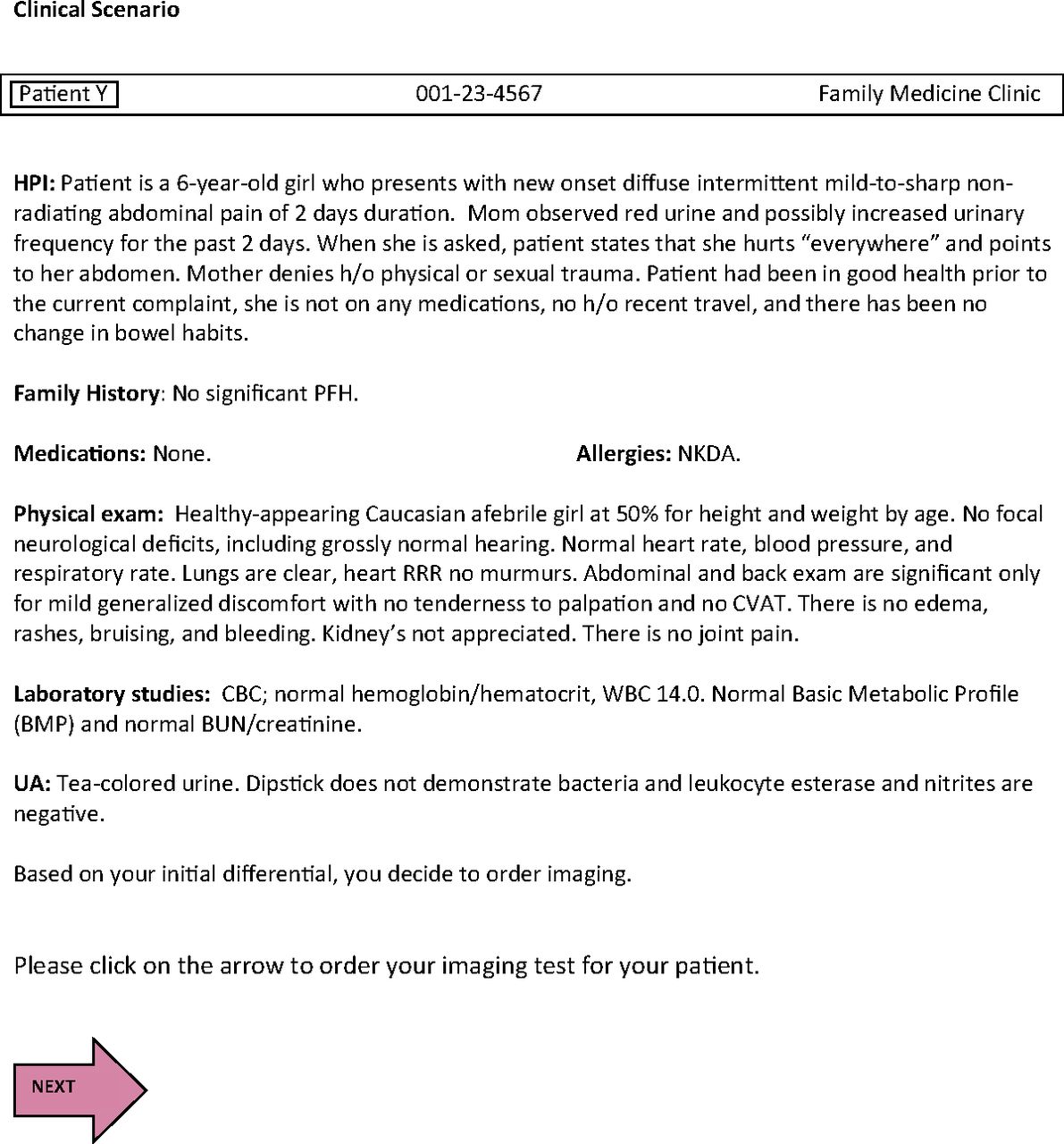
A double-blind, randomized simulation trial was conducted within the 17 family medicine training programs in the Military Health System (MHS). Physicians accessed an online clinical scenario describing a 6-year-old girl with painful, nontraumatic hematuria. There was no incentive for participation and no penalty for abstaining (see the screenshots in Appendix 1).
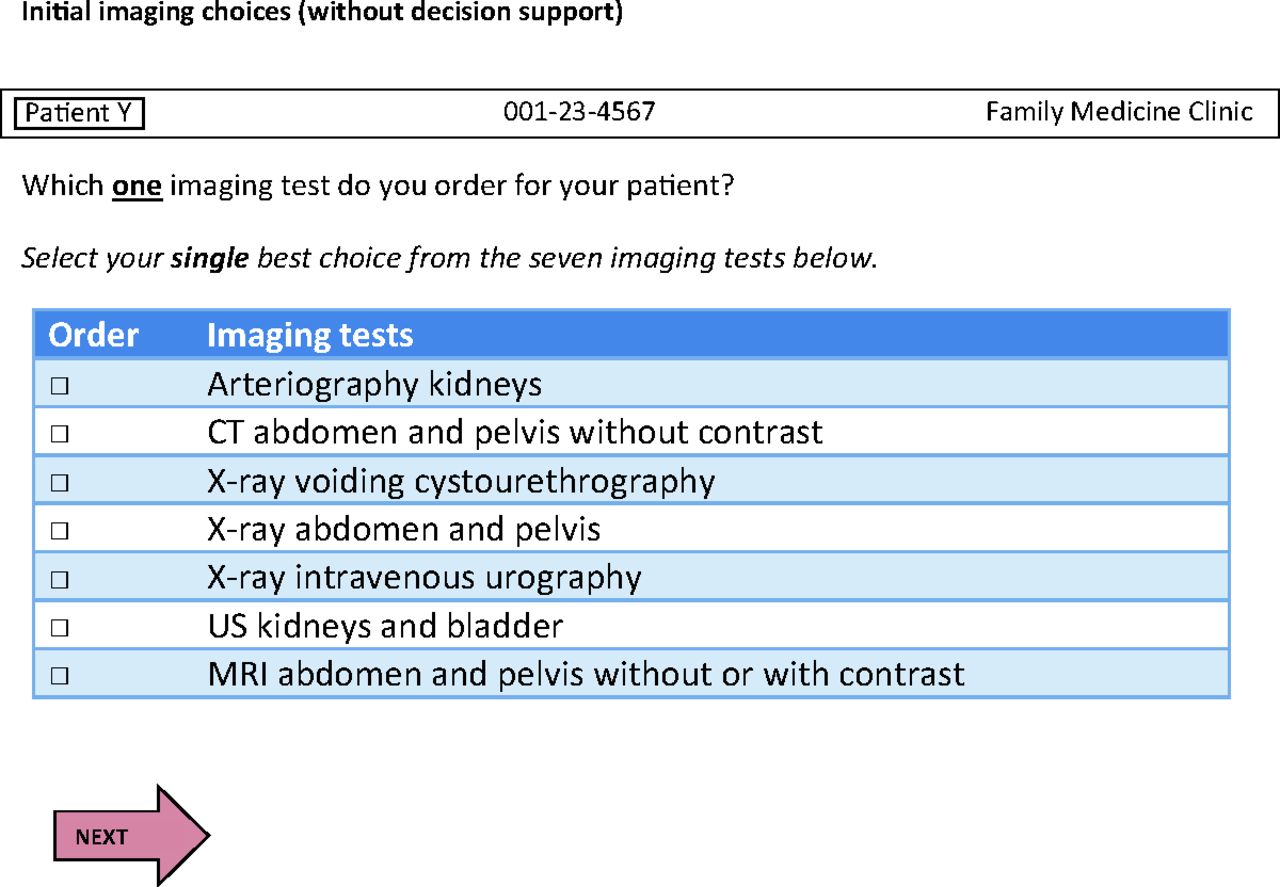
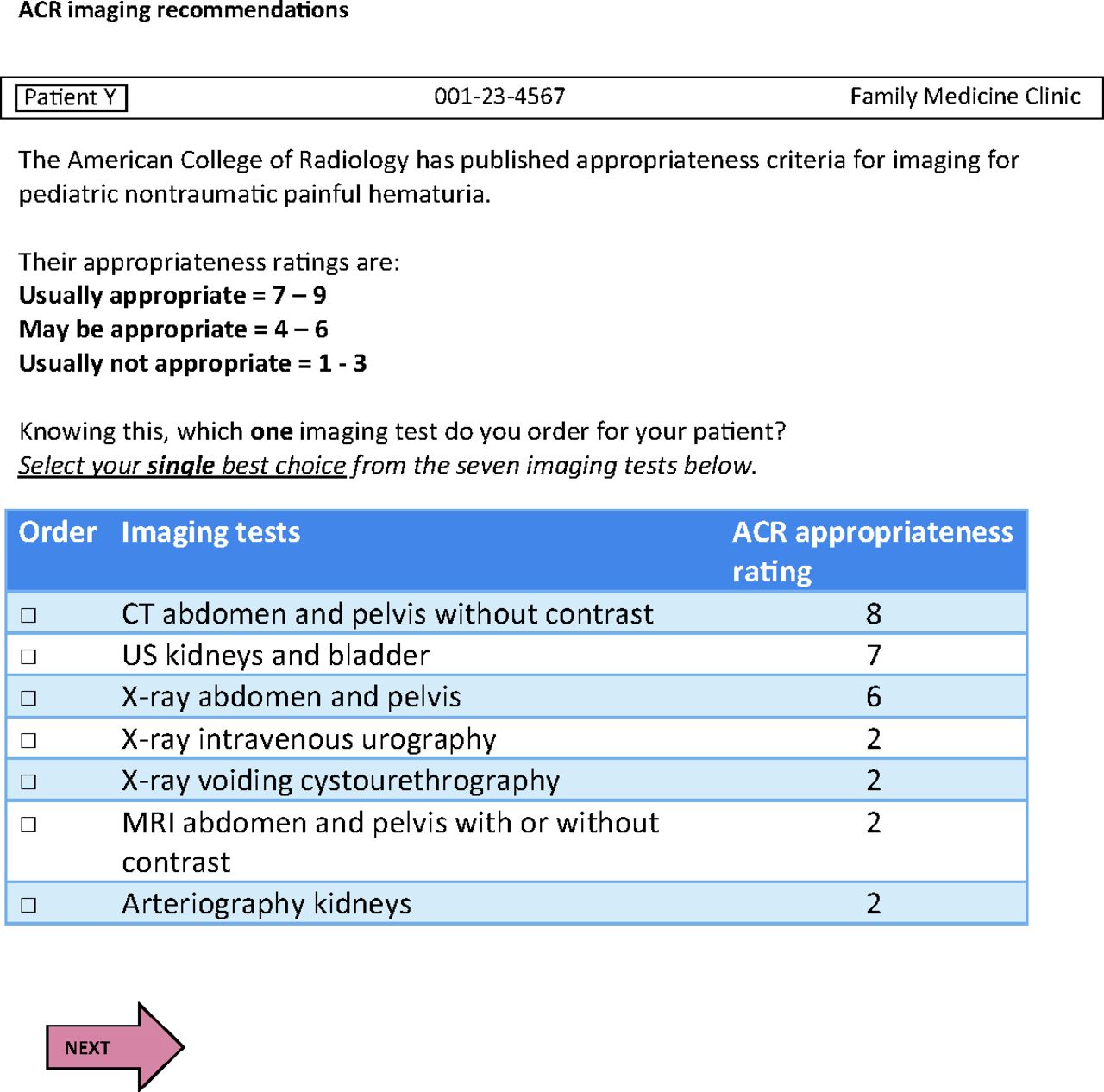
Without the aid of clinical decision support, participants selected a single, best-choice medical imaging modality from 7 randomized options derived from the ACR Appropriateness Criteria for painful, nontraumatic pediatric hematuria.10 The 2 imaging choices rated as “usually appropriate” (the highest possible ACR category, inclusive of numeric ratings of 7 to 9) in the selected ACR Appropriateness Criteria were CT of the abdomen and pelvis without contrast (rating of 8) and ultrasound of the kidneys and bladder (rating of 7). Of these 2 modalities, the estimated pediatric radiation dose for an abdominal and pelvic CT is 3 to 10 mSv, whereas ultrasound causes no radiation exposure.
After initial imaging selection, the study's first group was presented with the ACR Appropriateness Criteria ratings and then estimated radiation exposure information (RADS) for each imaging modality (ACR-RADS group). Participants were asked to select an imaging modality after each decision support screen. The second group had similar steps, but was presented with the same information in reverse order (RADS-ACR group; Figure 1).
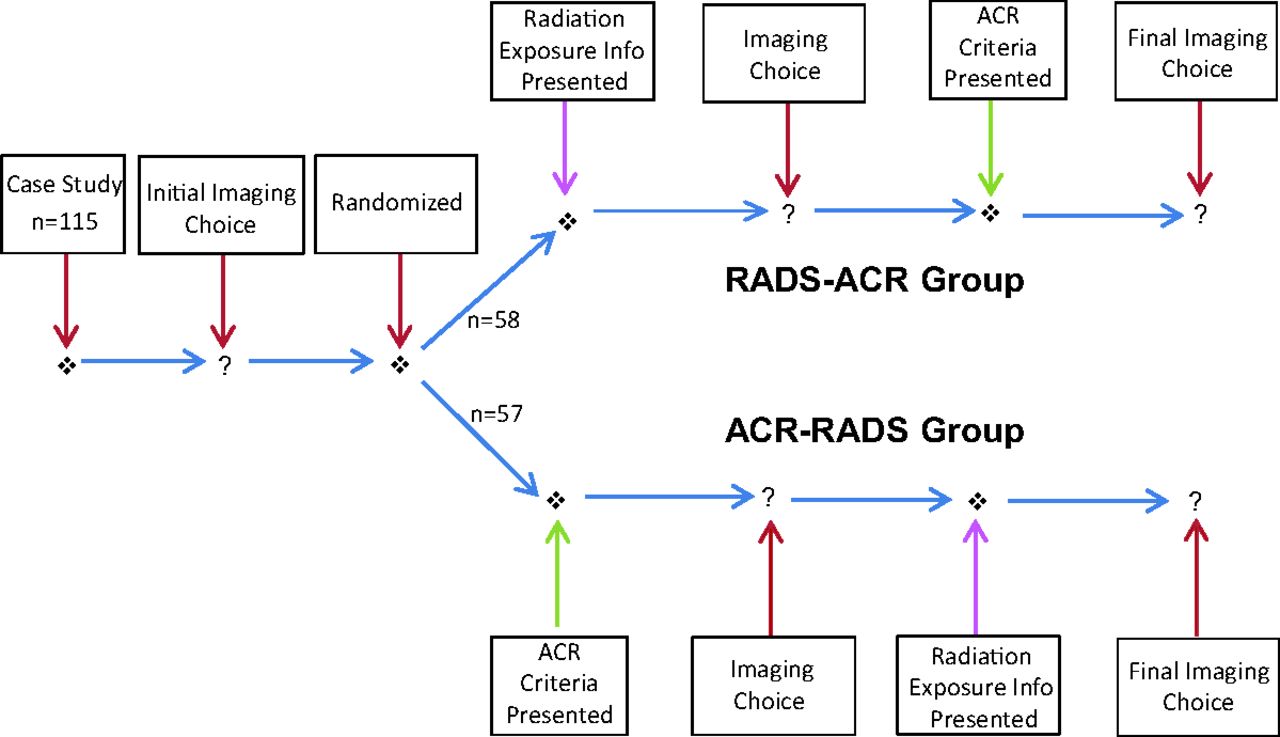
Participant study flow. After informed consent, review of a clinical case study, and an initial imaging decision, participants were randomized to 1 of 2 arms: ACR-RADS, a decision support screen presented with American College of Radiology (ACR) appropriateness criteria (ACR criteria) for each potential imaging order, followed by an imaging decision and then additional decision support with estimated radiation exposure for each potential image order (radiation exposure info) and a final imaging decision; and RADS-ACR, which presented estimated radiation exposure information followed by ACR Criteria with subsequent imaging decisions.
Data were entered into Microsoft Excel (Microsoft Corp., Redmond, WA) and imported into SAS (SAS Institute, Inc., Cary, NC). The Stuart-Maxwell test was used to test for equality of distributions under the initial, ACR, and RADS conditions. A power analysis and parametric comparisons between the ACR-RADS group and the RADS-ACR group were conducted using the χ2 test of homogeneity, with a 5%, 2-sided significance level. A sample size of 50 per group, with a difference in proportions between groups of at least 30%, led to a power exceeding 80%.
Results
A total of 115 physicians were enrolled and randomized to either the ACR-RADS (n = 57) or RADS-ACR groups (n = 58). Most respondents were men (75%), active military (85%), attending physicians (80%) from 31 to 50 years old (70%). There were no significant demographic differences between groups (Appendix 2).
Ultrasound was the initial imaging modality of choice for 70% (n = 80) of all respondents, followed by plain film (17%, n = 19) and CT (12%, n = 14). Over half of all participants initially selected and then maintained ultrasound as their imaging choice throughout the study (73%, n = 32 in the ACR-RADS group; 86%, n = 31 in the RADS-ACR group) (Table 1).
After presentation of the ACR Appropriateness Criteria, ultrasound selection (77% [n = 44] to 65% [n = 37]) and plain film use (14% [n = 8] to 3.5% [n = 2]) slightly decreased in the ACR-RADS group, whereas CT use (7% [n = 4] to 32% [n = 18]) increased (P = .008). After the ACR-RADS group was subsequently presented with RADS information, ultrasound use increased (81%, n = 46), whereas CT orders decreased (12%, n = 7; P = .007) (Table 1).
In the RADS-ACR group, ultrasound use (62% [n = 36] to 71% [n = 41]) slightly increased, whereas CT use (17% [n = 10] to 7% [n = 4]) and plain film use (14%, n = 8) slightly decreased; other tests (2% [n = 1] to 9% [n = 5]) increased slightly after receiving RADS information (P = not significant). When this group was presented with ACR guideline information, ultrasound use slightly increased (72%, n = 42), CT use (17%, n = 10) returned to the level it was before decision support, and plain film use slightly decreased (10%, n = 6; P = .05) (Table 1).
Discussion
Childhood exposure to ionizing radiation increases the lifetime risk of malignancy.2,8 To mitigate pediatric exposure, an international campaign to raise awareness about appropriate medical imaging is underway.11 Our study evaluated whether electronic medical record decision support with ACR guideline ratings and estimated RADS would change family physician decision making at the point of care.
We acknowledge that painful, nontraumatic pediatric hematuria is less common in the primary care setting. To determine whether physicians considered radiation exposure in their imaging selections, however, our construct required a pediatric scenario that had at least 2 guideline-recommended imaging choices that were at different ends of the radiation exposure spectrum. In this scenario and with this guideline, CT and ultrasound both were rated as “usually appropriate” yet have dramatically different radiation exposure risks.
Our results suggest that point-of-care access to RADS and imaging guidelines influences clinical decision making. There was a statistically significant difference in imaging modality selection when the first group received the ACR guidelines after their initial imaging choice. This effect was not noted when the second group received RADS after their initial choice.
The order in which family physicians received the information also affected their imaging modality selection. There was a statistically significant difference in imaging selection when the first group received RADS after the ACR guideline presentation. This did not occur in the second group, which received ACR guideline information after estimated radiation exposure decision support.
Our finding that ultrasound was the most frequently ordered modality across groups potentially suggests an underlying awareness of and concern for childhood radiation exposure. This also was demonstrated when both groups increased ultrasound use and decreased CT use when presented with data about estimated radiation exposure. This shift was more pronounced when such information was presented following the ACR Appropriateness Criteria guidelines presentation, likely because of the highest rating for CT in those guidelines. This result is consistent with our previous findings in adult patients.9
The ACR Appropriateness Criteria alone also seemed to influence the imaging modality selection. Both CT and ultrasound were rated as “usually appropriate,” but CT had the highest ACR rating among the 7 options, and CT selection increased whenever this information was presented. Interestingly, when family physicians initially (without decision support) selected an imaging modality rated “usually not appropriate” (eg, arteriography of the kidneys or magnetic resonance imaging of the abdomen and pelvis with or without contrast),10 subsequent presentation of the ACR Appropriateness Criteria eliminated the selection of these modalities in future decisions.
We acknowledge that this study involved a simulated case. Research suggests that imaging decisions made during an actual patient encounter may be influenced by external considerations such as patient expectations4,6 and the practice of “defensive” medicine,5,6 potentially limiting the generalizability of our findings. Also, our data were collected from a cohort of predominantly military physicians practicing within the MHS. This limitation is mitigated by studies suggesting similarities between physician behavior and patients in the MHS versus those in large civilian health care systems.9 While a CT may be obtained following a negative ultrasound, the opposite is rarely true; this is an additional limitation that may have influenced image ordering after decision support.
In this pediatric clinical scenario with 2 “usually appropriate” medical imaging options available, providing clinical decision support led to the selection of a guideline-recommended modality with lower estimated radiation exposure. This information could help inform safe, accurate, and clinically useful decision support algorithms in future electronic medical record systems.
Appendix 1
Screenshots Each Participant Viewed During the Study



Appendix 2
Participant Demographics
Notes
This article was externally peer reviewed.
Funding: Intramural funding was provided by the Uniformed Services University (grant no. R02930.4) and the US Department of Defense Patient Safety Program.
Conflict of interest: none declared.
Disclaimer: The views expressed herein are solely the views of the authors and do not represent those of the Uniformed Services University, the United States Air Force, the United States Navy, or the Department of Defense.
- Received for publication September 1, 2014.
- Revision received December 1, 2014.
- Accepted for publication December 9, 2014.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}