
Abstract
Background: The number and complexity of clinical laboratory tests is rapidly expanding, presenting primary care physicians with challenges in accurately, efficiently, and safely ordering and interpreting diagnostic tests. The objective of this study was to identify challenges primary care physicians face related to diagnostic laboratory testing and solutions they believe are helpful and available to them.
Methods: In this study, sponsored by the Centers for Disease Control and Prevention, a random sample of general internal medicine and family medicine physicians from the American Medical Association Masterfile were surveyed in 2011.
Results: 1768 physicians (5.6%) responded to the survey. Physicians reported ordering diagnostic laboratory tests for an average of 31.4% of patient encounters per week. They reported uncertainty about ordering tests in 14.7% and uncertainty in interpreting results in 8.3% of these diagnostic encounters. The most common problematic challenges in ordering tests were related to the cost to patients and insurance coverage restrictions. Other challenges included different names for the same test, tests not available except as part of a test panel, and different tests included in panels with the same names. The most common problematic challenges in interpreting and using test results were not receiving the results and confusing report formats. Respondents endorsed a variety of information technology and decision support solutions to improve test selection and results interpretation, but these solutions were not widely available at the time of the survey. Physicians infrequently sought assistance or consultation from laboratory professionals but valued these consultations when they occurred.
Conclusions: Primary care physicians routinely experience uncertainty and challenges in ordering and interpreting diagnostic laboratory tests. With more than 500 million primary care patient visits per year, the level of uncertainty reported in this study potentially affects 23 million patients per year and raises significant concerns about the safe and efficient use of laboratory testing resources. Improvement in information technology and clinical decision support systems and quick access to laboratory consultations may reduce physicians' uncertainty and mitigate these challenges.
Laboratory tests are essential tools for clinical diagnosis. Over the past 20 years, the number of laboratory tests available to clinicians has more than doubled to at least 3500 tests (ARUP Laboratories, Salt Lake City, Utah, personal communication). This complexity presents physicians with increasing challenges in accurately ordering and interpreting diagnostic tests and effectively using the results. These challenges are particularly acute for primary care physicians, who order the greatest variety of laboratory tests and order them during 30% to 40% of outpatient encounters.1
Proposed solutions to improve the accuracy, efficiency, and safety of ordering clinical laboratory tests and interpreting the results include clinical decision support tools, trending of test results in electronic medical records (EMRs),2 condition-specific algorithms to help select tests,3 professional practice guidelines,4 and reflex laboratory testing.5 Many electronic resources have been developed to aid diagnostic decision making.6 Well-designed information technology (IT) decision support tools may improve physicians' diagnostic accuracy and efficiency and patient safety. Poorly designed decision support tools or conflicting practice guidelines, however, present barriers to accurate and effective test selection and interpretation.7
In 2012, the Centers for Disease Control and Prevention's Clinical Laboratory Integration into Healthcare Collaborative (CLIHC), with support from the Altarum Institute, completed a national survey of family medicine and general internal medicine physicians to explore their degree of uncertainty when ordering and interpreting clinical laboratory tests, the challenges they face with laboratory diagnostic testing, and solutions to improve test utilization. Also of interest was the frequency with which primary care physicians initiate communication with laboratory professionals and the helpfulness of these consultations.
Methods
The Survey
Survey questions were based on the results of 3 focus groups comprising 27 primary care physicians and on suggestions from a panel of experts in primary care and laboratory medicine. Nineteen questions with subparts were constructed for the survey. Survey respondents were asked to consider laboratory testing for diagnostic purposes only, not for routine screening or monitoring of chronic diseases.
The survey domains included (1) physicians' uncertainty about ordering and interpreting tests, (2) tactics they use to overcome uncertainty, (3) factors that influence laboratory test ordering, (4) challenges in appropriate ordering and interpreting of diagnostic laboratory tests, and (5) perceived solutions to improve ordering and interpreting tests. We asked respondents about the number of patients per week for whom they ordered diagnostic tests, and the number for whom they felt uncertainty regarding the appropriate test to order or interpretation of the results. Responses were mostly forced choice, but open-ended responses also were allowed. Forced-choice responses were graded on 5-point scales. For frequency, responses ranged from “daily” to “never”; for how problematic, responses ranged from “extremely problematic” to “not at all problematic”; and for helpful/useful, responses ranged from “extremely helpful/useful” to “not at all helpful/useful.”
The survey was judged exempt from institutional review board review by the Office of the Associate Director for Science, Office of the Director, Centers for Disease Control and Prevention. The full text of the questionnaire is available upon request.
Survey Administration
A random sample of 31,689 family medicine and general internal medicine physicians was drawn from the 2011 American Medical Association (AMA) Masterfile. In December 2011, letters were mailed to these physicians inviting them to complete the online survey. Those who did not complete the survey after receiving the letter of invitation were subsequently E-mailed a link to the survey. Two additional E-mails were sent to nonresponders in January and February 2012. To encourage participation, respondents were invited to direct a $10 donation to their choice of 1 of 5 charities.
Analysis
The analysis presented in this article is entirely descriptive. Not all respondents answered all questions, but we included their responses to the questions they did answer. Results are presented as the percentage of respondents who selected the top 2 of the 5 possible responses. For frequency, the top 2 were “daily” and “at least once a week”; for problematic this included “extremely” and “very” problematic; and for helpful/useful this included “extremely helpful/useful” and “very helpful/useful.”
Results
Respondent Characteristics
Of the 31,689 physicians, 29.67% opened one of the E-mail invitations and 18.8% (n = 1,768) of those who opened an E-mailed invitation completed the survey, a 5.6% overall response rate. Demographic characteristics of the respondents (Table 1) are similar to the AMA Masterfile physician population and to the sampling frame.
Uncertainty About Test Ordering and Results Interpretation and Tactics to Reduce Uncertainty
Physicians had an average of 80.9 patient visits per week and reported ordering diagnostic laboratory tests during an average of 31.4% of these patient encounters. They reported uncertainty about test ordering in 14.7% and uncertainty in interpreting results in 8.3% of these diagnostic encounters. Physicians reported using a variety of tactics to overcome uncertainty in ordering and interpreting laboratory tests, as summarized in Figures 1 and 2. As reported by physicians, the most helpful/useful tactics for overcoming these uncertainties about testing were curbside consultation, E-references, and referral to specialists. In addition, when physicians were uncertain about test interpretation, they frequently brought patients in for follow-up and a review of their medical histories. Only 6% of respondents consulted with laboratory professionals on a weekly basis, although they found that the consultation was useful.

Overcoming uncertainty in ordering laboratory diagnostic tests. The percentages of primary care physicians reporting the helpfulness of these tactics as very helpful or extremely helpful and the percentages using these tactics daily or at least once a week are shown. PCP, primary care physician.

Overcoming uncertainty in interpreting laboratory test results. The percentages of primary care physicians reporting the usefulness of these tactics as very useful or extremely useful and the percentages using these tactics daily or at least once a week are shown. PCP, primary care physician.
Influences on and Challenges in Test Ordering
Physicians agreed that the following factors were important influences on their test ordering: national (63%) and local (46%) clinical practice guidelines, patient factors related to insurance (40%), patients' cost (53%), and malpractice concerns (39%). Physicians' challenges in test ordering are listed in Table 2. Two general categories emerged: (1) cost and insurance and (2) test ordering mechanisms. Cost to patients and insurance company rules were the most challenging. The mechanisms for ordering tests were less problematic yet still important challenges.
Challenges in Interpreting and Using Test Results
Physicians' challenges with interpreting and using test results are summarized in Table 2 and comprised 2 general categories: receiving the results and report formats.
Solutions to Improve Test Ordering and Results Interpretation
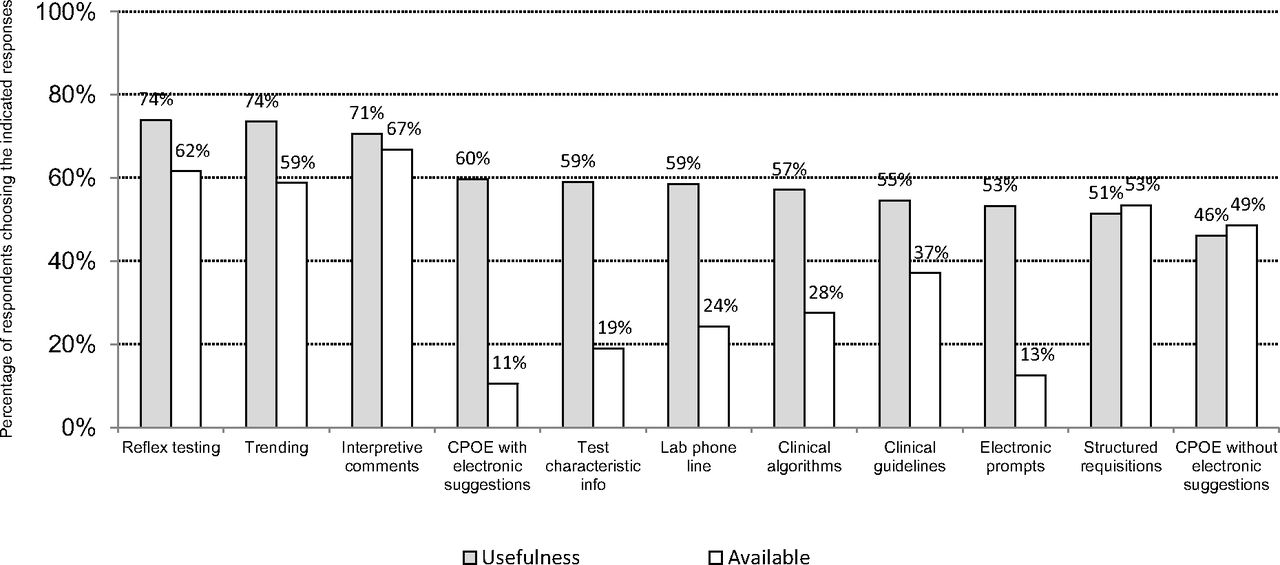
Physicians' degree of endorsement of 11 possible solutions to improve test ordering and results interpretation is shown in Figure 3. Usefulness ranged from 46% for computerized physician order entry (CPOE) without electronic suggestions to 74% for reflex testing and trending of laboratory results over time. Almost 50% of respondents have CPOE without electronic suggestions but they rank it the lowest in usefulness. Availability of solutions ranged from 11% for CPOE with electronic suggestions for appropriate tests to 67% for interpretative comments. Only 11% of respondents had CPOE with electronic suggestions, but 60% of these physicians found it useful.
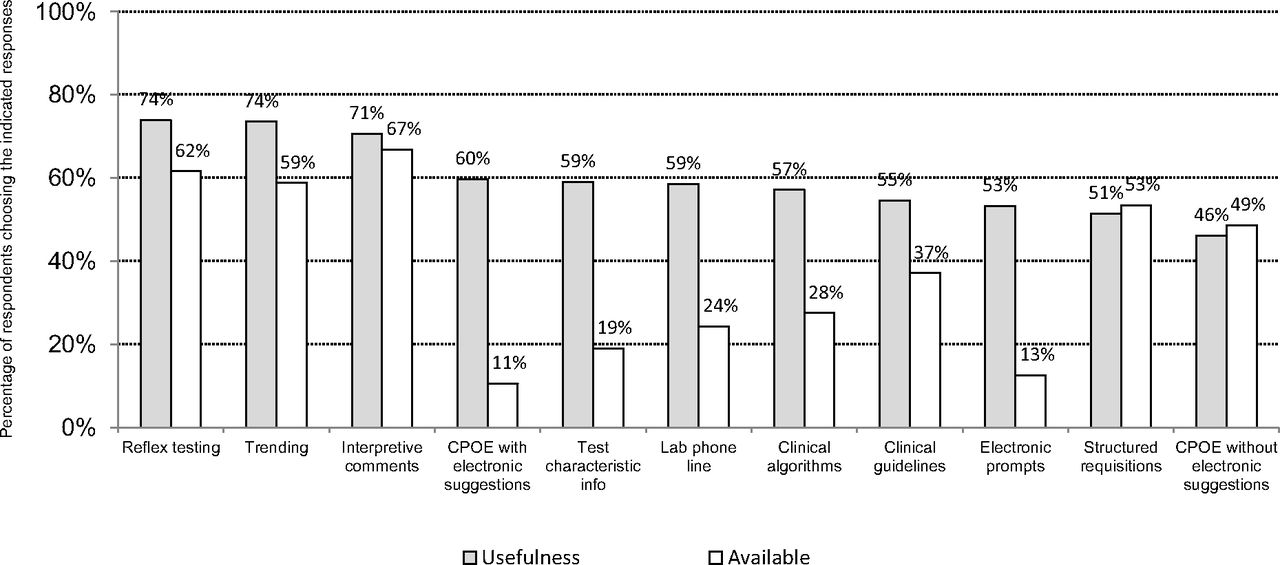
Solutions for more effective use of diagnostic laboratory testing. The percentages of primary care physicians endorsing these solutions as very useful or extremely useful and the percentage with these solutions available at their site. CPOE, computerized physician order entry.
Consulting the Clinical Laboratory
We asked several questions about the helpfulness of consultation with the clinical laboratory. The percentage of respondents who reported contacting laboratory professionals at least once per week ranged from 4% for medical or scientific opinion of significance of results to 26% for status of missing results. The percentage reporting that these communications were very or extremely helpful ranged from 37% for assistance with appropriate test ordering based on patient's symptoms and history to 65% for technical assistance regarding sample collection or submission.
Discussion
From this national survey, we compiled a database of the challenges primary care physicians face in ordering and interpreting laboratory tests and physicians' suggestions for improving clinical laboratory utilization. Many respondents reported challenges in ordering and interpreting appropriate laboratory tests. These survey respondents reported some degree of uncertainty in ordering tests for 14.7% of patient encounters and interpreting test results for 8.3% encounters in which physicians ordered diagnostic laboratory tests. With more than 500 million patient visits to primary care physicians per year8 and 31.4%, or 157 million patient visits, resulting in test ordering, the levels of self-reported uncertainty in this study could affect ordering tests for 23 million patients and interpreting test results for 13 million patients per year. This level of uncertainty raises significant concerns about the safety and efficient use of laboratory testing resources.
More than 50% of physicians reported that a variety of IT solutions would be very useful to them; however, these decision support technologies were not yet available to most of our respondents in December 2011. Of all respondents, 88% use CPOE at least weekly, but they did not find CPOE per se useful for guidance in test selection. CPOE that has embedded in the software suggestions or prompts about appropriate testing (ie, electronic clinical decision support) was judged to be very to extremely useful by 60% of the physicians, but only 11% had access to it. Mobile devices with clinical decision support applications are emerging as alternatives to those embedded in EMRs. We believe that EMRs and mobile applications are 2 platforms for clinical decision support that hold great promise for improving test selection and interpretation.
Physicians identified cost as a significant barrier to ordering laboratory tests. Between 2006 and 2011, the proportion of privately insured patients facing a deductible greater than $1000 increased from 10% to 31%.9 Few diagnostic laboratory tests are exempt from these deductibles. The absence of information about laboratory test costs for patients and clinicians as well as the effect of these costs on clinical practice and care have been issues of concern for many years.10⇓–12 When physicians were informed of charges for outpatient visits, Tierney et al11 observed a 16.8% decrease in laboratory test orders, a 15.3% decrease in charges for laboratory tests, and no effect on hospitalizations or emergency department visits. Providing physicians with laboratory test fees at the time of order entry resulted in modest decreases in test ordering, but the effect on patient outcome was not determined.13 Technology for rapid availability of cost data at the point of care may be helpful to modify escalating health care costs. Some institutions have restructured their order forms to reduce unnecessary or redundant test ordering.14
Physicians frequently obtain curbside consults, consult E-references, and refer patients to specialists when uncertain about diagnostic issues. Consultation with pathologists and laboratory personnel could also be a rapid and cost-effective method for reducing uncertainty about test ordering and interpretation. Smith et al15 proposed this potential metric to improve primary care laboratory testing processes: “Primary care providers should have convenient access to laboratory physicians to assist in laboratory test ordering and interpretation.” Laboratory managers and pathologists should develop better communication channels with busy physicians to make consultative services easily available. This could improve patient care through more appropriate laboratory utilization and potentially reduce costs by avoiding specialist referrals solely for test interpretation.
The low response rate in this survey (5.6%) and inclusion of only primary care physicians limits the generalizability of these results. The low response rate may have been due in part to the length of the survey. The web-based survey design may have deterred physicians who are less adept with technology. The respondents' demographic characteristics, however, are similar to those of the population included in the AMA Masterfile of family physicians and general internal medicine physicians and cover a wide range of ages, years in practice, and practice settings from physicians throughout the United States. Therefore, results may broadly represent the common experiences of primary care physicians. We solicited physicians' opinions; therefore, we cannot verify the extent to which objective evaluation would confirm our findings. Finally, prior research shows that physicians may be overconfident about their knowledge,16 which, when combined with social desirability bias, may have resulted in underreporting of uncertainty regarding test selection and results interpretation.
Conclusion
Improved ordering methods, improved reporting formats, and access to laboratory consultation are potential ways to lessen uncertainty about ordering laboratory tests and interpreting the results. Collaborations among primary care physicians, laboratory professionals, and bioinformatics experts could generate electronic tools to address the challenges identified in this survey, thus enhancing the safety, effectiveness, efficiency, and timeliness and decreasing the cost of clinical laboratory testing. Our survey results suggest that many physicians are ready to embrace sophisticated electronic clinical decision support tools.
Notes
This article was externally peer reviewed.
Funding: This study was supported in part from a contract (GS-10F-0261K) funded by the Centers for Disease Control and Prevention/Agency for Toxic Substances and Disease Registry. OMB Control Number 0920–0893.
Conflict of interest: none declared.
Disclaimer: The findings and conclusions in this publication are those of the author(s) and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
- Received for publication March 25, 2013.
- Revision received November 17, 2013.
- Accepted for publication November 25, 2013.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Improving the primary care clinical testing process in southwest Scotland: a systems-based approach
- Successful demand management in diagnostic immunology testing
- Patient, hospital and environmental costs of unnecessary bloodwork: capturing the triple bottom line of inappropriate care in general surgery patients
- Successful demand management in diagnostic immunology testing
- Benefits and barriers to implementing precision preventive care: results of a national physician survey
- Downstream activities after laboratory testing in primary care: an exploratory outcome of the ELMO cluster randomised trial (Electronic Laboratory Medicine Ordering with evidence-based order sets in primary care)
- Why is there variation in test ordering practices for patients presenting to the emergency department with undifferentiated chest pain? A qualitative study
- Influence of serum iron test results on the diagnosis of iron deficiency in children: a retrospective observational study
- Educational intervention to optimise serum immunoglobulin test use in Irish primary care: an interrupted time series with segmented regression analysis
- Overutilization of Test for Hemoglobinopathy Evaluation: Experience from a Tertiary Care Academic Medical Center
- Practical Guidance for Clinical Microbiology Laboratories: Viruses Causing Acute Respiratory Tract Infections
- A Review of Published Studies on the Value of Laboratory Medicine
- How are junior doctors managing patients with self-limiting illnesses at their first presentation? A video vignette study
- Promoting Interprofessionalism Within an Academic Environment
- Labtracker+, a medical smartphone app for the interpretation of consecutive laboratory results: an external validation study
- Removing Cerebrospinal Fluid Antibody Orders from the Test Menu Results in a Dramatic Decrease in Order Volume
- Launching a Laboratory Testing Process Quality Improvement Toolkit: From the Shared Networks of Colorado Ambulatory Practices and Partners (SNOCAP)
- Content Usage and the Most Frequently Read Articles of 2014
- Current Evidence and Future Perspectives on the Effective Practice of Patient-Centered Laboratory Medicine
- Investigating Patient-Centered Care