
Abstract
Purpose: Burnout is a threat to the primary care workforce. We investigated the relationship between team structure, team culture, and emotional exhaustion of clinicians and staff in primary care practices.
Methods: We surveyed 231 clinicians and 280 staff members of 10 public and 6 university-run primary care clinics in San Francisco in 2012. Predictor variables included team structure, such as working in a tight teamlet, and perception of team culture. The outcome variable was the Maslach emotional exhaustion scale. Generalized estimation equation models were used to account for clustering at the clinic level.
Results: Working in a tight team structure and perceptions of a greater team culture were associated with less clinician exhaustion. Team structure and team culture interacted to predict exhaustion: among clinicians reporting low team culture, team structure seemed to have little effect on exhaustion, whereas among clinicians reporting high team culture, tighter team structure was associated with less exhaustion. Greater team culture was associated with less exhaustion among staff. However, unlike for clinicians, team structure failed to predict exhaustion among staff.
Conclusions: Fostering team culture may be an important strategy to protect against exhaustion in primary care and enhance the benefit of tight team structures.
Burnout is a threat to the primary care workforce. Staff and clinicians in primary care report high levels of emotional exhaustion,1 with primary care physicians evincing some of the highest levels of burnout among physician specialties. In a recent survey, more than 50% of primary care clinicians reported symptoms of burnout, compared with 28% of the general employed population.2
Characterized by low professional efficacy, high exhaustion, and high cynicism,3 burnout threatens recruitment and retention of primary care clinicians. Apprehensions about the stresses of primary care practice may contribute to the decreasing numbers of medical graduates and physician assistant graduates choosing careers in family medicine or general internal medicine.4⇓⇓⇓⇓–9 Clinicians experiencing burnout are more likely to leave medicine entirely.10,11 Although risk factors for and effects of burnout among clinical support staff have been less studied, these members of the primary care team face many of the same challenges associated with clinician dissatisfaction, such as a hurried and chaotic work pace and lack of control over their work environment.11
The consequences of burnout are pernicious and far reaching. Clinician burnout and corresponding professional dissatisfaction have been associated with medical errors,12⇓–14 reduced quality of medical care,15⇓–17 poor communication with patients,17 longer recovery time following hospitalization,18 poor adherence of patients to care plans,19 lower patient satisfaction,18,20 and a reluctance to take on new patients insured by Medicaid or Medicare.15 In the face of these challenges, clinician well-being has been proposed as a new quality indicator.21
Team-based care may serve as an antidote to the overwhelming demands of primary care.22,23 Case studies of high-performing practices frequently cite tight team structures as instrumental to practice transformation and the improvement of patient care.24,25 Effective team functioning in health care is associated with greater career satisfaction among clinicians as well as improved quality of care and greater patient satisfaction.24,26
We investigated the relationship between team structure, team functioning, and emotional exhaustion of clinicians and staff in primary care practices. Our hypotheses were 3-fold. First, we hypothesized that a tight team structure, such as a “teamlet” model in which a clinician works with the same medical assistant or other support staff on a consistent basis,23 would be protective against exhaustion, the central and most obvious symptom of burnout.3 Second, we hypothesized that team culture—a sense of effective team functioning among clinicians and staff—would be associated with lower exhaustion. Finally, consistent with the conceptual model of teamwork developed by Hackman27 positing structure as an enabler of team performance, we hypothesized that the relationship between team structure and exhaustion would depend on team culture within the clinic.
Methods
We conducted a cross-sectional survey of clinicians and staff in primary care practices using a self-administered questionnaire conducted in waves across the study sites between February and May 2012. The study included 10 of the 11 clinics providing comprehensive primary care services in a county-administered health system (one clinic declined to participate) and all 6 comprehensive primary care practices in a university-administered health system, with an annual visit volume of 264,000 in 2011. The county-administered system serves primarily publicly insured (64%) and uninsured (36%) populations, whereas the university system serves primarily patients with commercial insurance (66%) and Medicare (23%). Two of the practices in each system were residency program teaching clinics, and all practices were located in San Francisco, California. None of the participating practices had applied for formal recognition as a patient-centered medical home at the time of the survey. All staff and clinicians (physicians, nurse practitioners, and physician assistants) at the clinics were eligible for the study.
Measures
Survey measures examined team structure, team culture, exhaustion, and respondent characteristics. Team structure may encompass several elements, such as the different professional disciplines and role definitions among team members.27 We focused exclusively on one important domain of team structure: the consistency with which clinicians are paired with the same clinical assistants, which has been suggested as an ingredient of high-performing primary care.23 We measured team structure using an item developed by the study team. For clinicians, the item asked, “Which of the following best describes your team model at your clinic?” Response categories were (1) I almost always work with the same medical assistant, (2) I almost always work with a small group of medical assistants, or (3) I rarely work with the same medical assistant or small group of medical assistants. For staff, the item asked, “Do you have a consistent working relationship with one provider or a small team of providers (a small subset of providers in your clinic, such as a pod or a teamlet)?” Response categories were yes or no.
Research has identified a number of domains that make up “team culture,” including the quality of task-related interactions (eg, communication, participation, effort) and the quality of social interactions (eg, social support, respect, shared objectives).27,28 After reviewing the literature, we did not find a concise, validated team culture measure for primary care that adequately captured the desired components. We therefore developed an 8-item measure by adapting items from the Team Climate Survey29 and the inventory of adaptive reserve.30 Each item was rated on a 10-point Likert scale, ranging from strongly disagree (1) to strongly agree (10). After reverse-coding 2 items, we tested the internal validity of the team culture scale by conducting a principal components factor analysis with promax rotation for these 8 items. Of the 8 items, 7 had factor loading scores >0.35 and were included in the final scale; the item “my most important task in clinic is to manage patient flow” had a low factor loading (0.20) and was excluded (Table 1). The final 7-item team culture scale had a Cronbach α of 0.80. Removal of the item with a loading score of 0.35 (“I feel unprepared for many of the tasks that I am asked to do every day”) did not improve the Cronbach α, and this item was retained in the scale. The team culture scale score was computed as the mean of the 7 scale items; a higher score indicates greater team culture.
We measured exhaustion, the most obvious symptom of burnout, using the validated 5-item Emotional Exhaustion scale from the General Survey version of the Maslach Burnout Inventory (Cronbach α = 0.92 in our sample).31 The Emotional Exhaustion scale produces a mean score ranging from 0 to 6, where 6 is the highest level of exhaustion; a score of 3.2 or higher (≥16 on the sum score) is classified as high exhaustion.
We assessed respondent characteristics using additional questions about issues such as hours or shifts worked per week (staff: ≤20 or >20 hours per week, clinicians: 1–2, 3–5, or ≥6 half-days per week); tenure (<1, 1–5, or >5 years); and system (county or university). For clinicians, we categorized respondents as resident physicians, nurse practitioners/physician assistants, or attending physicians. For staff, we grouped respondents into 2 categories to differentiate those working in direct patient care roles alongside clinicians from those working in other roles, using the question, “Do you room patients or take vitals?” From health system administrative data, we identified when each clinic first implemented its current electronic health record (EHR), hypothesizing that burnout might increase during EHR implementation (not in transition or in transition [±6 months to EHR go-live date]).
Survey Administration
The survey was offered in both web-based and paper form, based on the preferences of the clinic directors. Study personnel administered paper surveys during staff meetings. Clinicians and staff receiving web-based surveys were sent an initial invitation via E-mail and up to 3 additional reminders by E-mail. Medical directors and clinic administrators were advised about the response rate for their site and asked to encourage staff and clinicians to respond. Respondents to the survey were entered in a raffle for $25 gift cards.
Data Analysis
Data analysis was conducted using SPSS version 20 (SPSS Inc/IBM, Chicago, IL). We examined predictors of exhaustion using generalized estimating equation (GEE) models to account for clustering by clinics. Models were examined in stepwise fashion. Model 1 included only individual GEE models with only one predictor included at a time to examine bivariate relationships between team structure, team culture, respondent characteristics, and exhaustion scales. Models 2 to 4 were multivariate GEE models that included all participant characteristics as covariates and sequential addition of the 2 main predictor variables. Model 2 added team structure. Model 3 added team culture in addition to team structure. Model 4 included an interaction term for team structure and team culture. Analyses were conducted separately for clinicians and staff. Quasi-likelihood under the independence model criterion was calculated as a measure of goodness of fit for each model. The independence model criterion compares fit across GEE models (model selection), where a smaller model fit statistic relative to another model statistic indicates greater fit. There was a concern that residents could skew the results because of their unique experiences as clinicians in training, so we conducted a sensitivity analysis excluding this group.
The protocol was approved by the University of California, San Francisco, Committee on Human Research (11-08048). All individual-level responses were kept confidential. Medical directors and clinic administrators were provided with results aggregated at the level of their own clinic, along with results for all clinics in their system combined for comparison.
Results
Of 420 eligible clinicians, 231 (55%) responded; 280 of 428 eligible staff (65%) responded. Clinicians and staff of teaching clinics were less likely to respond to the survey than those at nonteaching clinics, and resident clinicians were less likely to respond than nonresidents. Most clinicians (83%) worked part time, whereas the majority of staff worked full-time (Table 2). More than a third of clinicians responding to the survey were residents (37%), 13% were nurse practitioners or physician assistants, and half (50%) were attending physicians. Just over half of respondent staff (56%) played clinical support roles involving rooming patients or taking vital signs. Most staff (61%) reported working in a consistent team. A few clinicians (10%) reported rarely working with the same team members; most worked with the same group of medical assistants in a team (72%), and almost 1 in 5 (18%) consistently worked with the same medical assistant in a teamlet model.
The mean team culture rating among staff (6.90) was somewhat higher than that among clinicians (6.17). More than half of clinicians (60%) and 43% of staff reported high levels of emotional exhaustion. Resident physicians reported the highest prevalence of exhaustion, with 69% of residents reporting high exhaustion (data not shown).
In bivariate GEE models, clinician exhaustion was positively associated with the number of half days worked, being in transition to an EHR, and being a resident (Table 3). Being in a tighter team structure and reporting a greater team culture were associated with less clinician exhaustion. For staff, working full time, having longer tenure, and being in transition to an EHR were associated with more exhaustion, whereas a greater team culture was associated with less exhaustion (Table 4). Staff working in a tighter team structure reported greater team culture (β = 0.82; 95% confidence interval [CI], 0.46–1.17; P < .001). Clinicians working in teamlets (β = 1.36; 95% CI, 0.55–2.16; P < .001), but not those working in teams (β = 0.30; 95% CI, −0.39 to 0.99; P = .40), reported greater team culture than clinicians not working in teams (results not shown in tables).
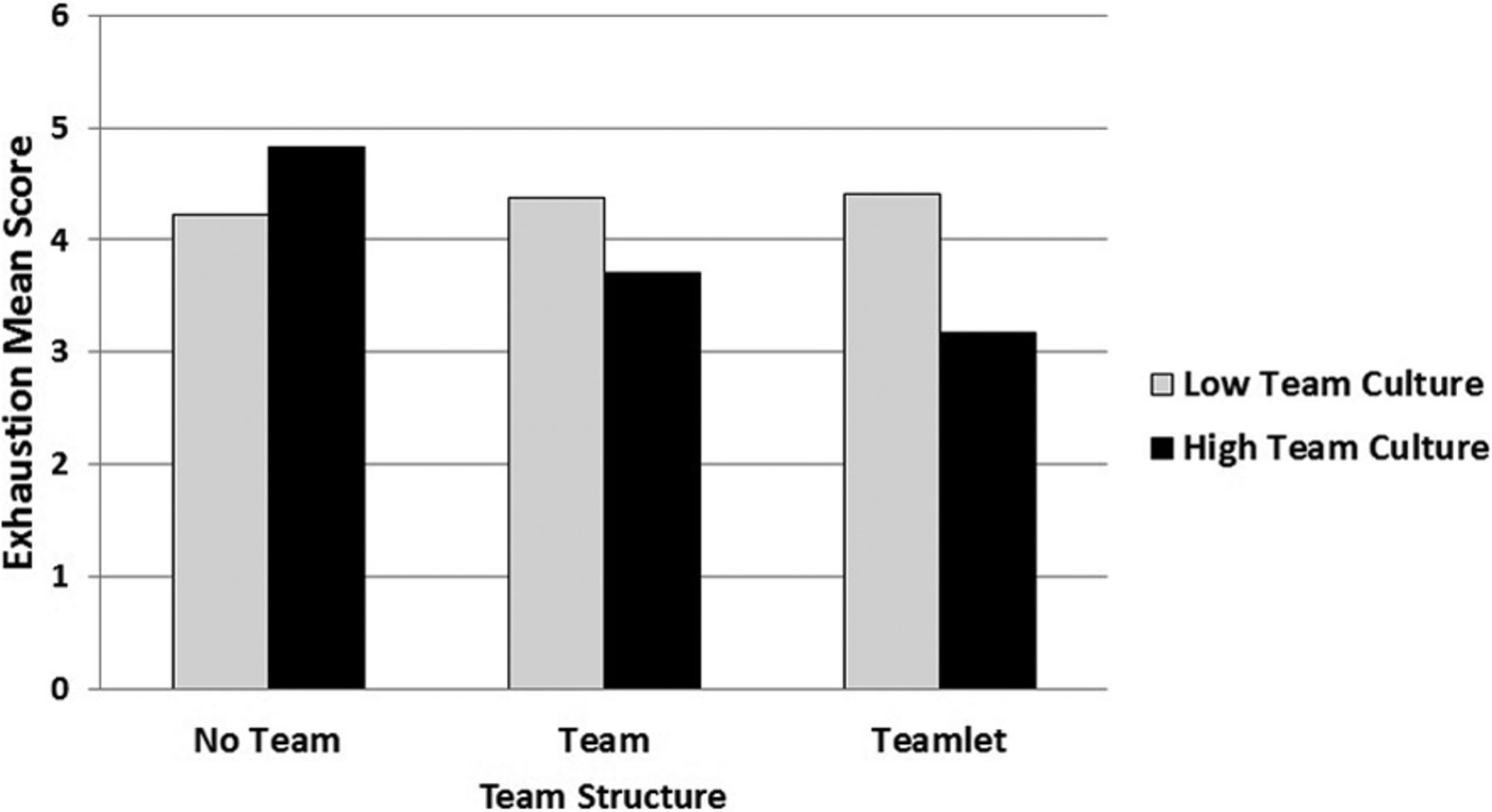
In multivariate GEE models, more clinician exhaustion was associated with a larger number of half days worked, being in transition to an EHR, and being a resident (Table 3; Models 2 to 4). Across all models, being in a tighter team structure was associated with less exhaustion. Team culture was independently associated with less exhaustion, and adding team culture to model 3 decreased the magnitude of the association of team structure and exhaustion. Team structure and team culture interacted to predict exhaustion, such that among clinicians reporting low team culture, team structure seemed to have little effect on exhaustion, whereas among clinicians reporting high team culture, tighter team structure was associated with less exhaustion (see Table 3, model 4; Figure 1). Clinicians in the tightest team structure (teamlets) and who reported high team culture (using a median split) had exhaustion scores that were >1.5 points lower than clinicians not working in teams who reported high team culture, an effect size of >1. After removing residents from the regression models, we found a virtually identical pattern of results for the association between team culture and structure and burnout among attending physicians and nonphysician clinicians (data not shown).
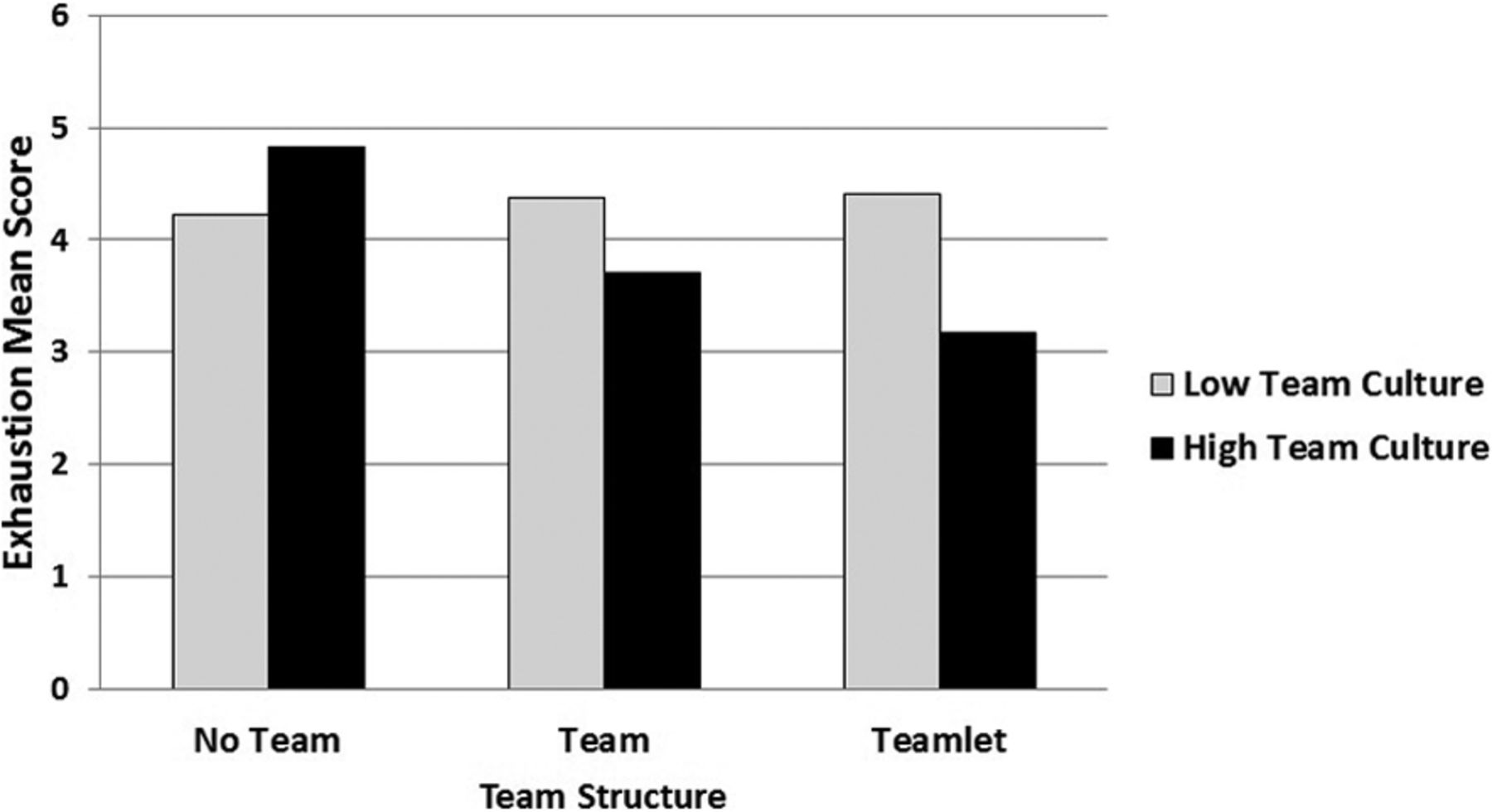
Interaction between team structure and team culture on exhaustion for clinicians (adjusted for covariates). A median split is used to define low versus high team culture.
In multivariate analysis staff exhaustion was associated with greater tenure and with being in transition to an EHR (Table 3). As was found for clinicians, greater team culture was associated with less exhaustion among staff. However, unlike for clinicians, team structure failed to predict exhaustion among staff, either alone or as part of an interaction term.
Discussion
Burnout in primary care threatens the engagement of team members and the quality of patient care. We found that perceptions of a better team culture were significantly associated with less clinician exhaustion. A tight team structure seems to have added benefit for the outcome of clinician exhaustion, but only when clinicians perceived an underlying positive sense of team culture. For staff, team culture but not team structure was associated with staff exhaustion.
These findings suggest that fostering a team culture may be an important strategy to protect against burnout in primary care. Prior studies have identified problematic personalities and hierarchy as challenges to effective teamwork.28 Health care lags behind many other sectors in institutionalizing training to promote team culture. Examples of training approaches systematically adopted in other settings include crew resource management by the aviation industry and team dimensional training by the US military.30 In our own work coaching primary care practices to improve, we have found that one of the basic tasks is facilitating a culture of teamwork through activities such as establishing ground rules, empowering staff to take on new roles, and inverting hierarchical relationships in meeting structures and processes.
Creating structures in which clinicians work consistently with the same medical assistant in a teamlet model, the tightest of team structures, may also reduce clinician exhaustion. However, our results also sound a cautionary note about placing staff in teams without efforts to improve team culture. In practices without a team culture, team structure alone may be ineffective in reducing exhaustion. Particularly for staff, exhaustion did not seem to be directly related to team structure but was associated with team culture. The finding that culture trumps structure for staff is consistent with our experience that when members of a team do not get along or communicate well, team structure alone does not improve the quality of work life. Comments written in response to open-ended questions on the survey support this interpretation, with some staff articulating apprehensions about working in tighter team structures if clinic leadership does not set and enforce expectations for respectful communication and personal responsibilities, both of which are key elements of team culture. The divergence in findings for team structure between clinicians and staff may reflect differences in role authority, with clinicians experiencing a tighter team structure as an opportunity to delegate responsibilities and prescribe workflow tasks to medical assistants, and medical assistants finding themselves in a subordinate position irrespective of team structures.33,34
The level of exhaustion measured in this study population is troublingly high but similar to that found in the literature. More than half of nonresident clinicians (55%) reported high exhaustion, which is comparable to the 50% reported among a national sample of family physicians and general internists.2 Among residents the proportion reporting high exhaustion (69%) was greater than the level found in several other studies.13,35 The proportion of staff reporting high exhaustion (43%) was greater than the 33% found in a previous study.1 Although not one of our primary research questions, our study detected that transitioning to a new EHR is a stressful experience for clinicians and staff alike.
The types of transformed practice models that are commonly referred to as patient-centered medical homes may change the structure and culture of primary care practice in a way that either enhances or worsens work life experiences. An initial attempt to implement a patient-centered medical home model at group health cooperative was associated with increased clinician fatigue and dissatisfaction; a second attempt that took into account quality of work life demonstrated a significant reduction in clinician and staff exhaustion.1 A study using cross-sectional methods found that patient-centered medical home attributes were associated with lower morale at a group of safety net clinics,36 although there is evidence that improvements in quality and care delivery at safety net clinics are associated with higher morale and lower burnout when there is adequate staffing, fair distribution of responsibility, and training infrastructure.37 Keeping a focus on team culture could enhance the effects of practice transformation on work life experiences.
Our study has several limitations. This cross-sectional survey cannot examine causal or longitudinal relationships. Data were self-reported. While response rates were comparable to or higher than reported response rates for other surveys of clinicians,38 nonresponders may have differed from participants in the survey. Residents and clinicians at teaching clinics and staff at nonteaching clinics were less likely to respond to the survey than their counterparts, which may have influenced the results. Four of the 16 practices included in this sample were teaching clinics, which may also limit generalizability. However, the findings were robust even when residents were excluded. Surveys were conducted in 2 organized health systems with employed physicians, and findings may not be generalizable to other settings and populations. However, the majority of primary care physicians in the United States are now practicing under employed arrangements.39 We selected one aspect of team structure—the arrangement of clinicians and clinical assistants—but there are undoubtedly additional structural aspects that are important for effective functioning of teams. In addition, work life factors other than the ones measured in our study may contribute to the experience of exhaustion.
Conclusion
Our findings suggest that a strong team culture may protect against exhaustion for both staff and clinicians in primary care. Tight team structures such as the teamlet model may help to promote team culture, in particular among clinicians. However, in the absence of a strong team culture, tight team structures may not protect against exhaustion. In addition to advancing the patient-centered triple aims of better care, better health, and more affordable costs, the movement to transform primary care may rightly be considered to have quadruple aims, with the fourth aim being to make the practice of primary care a joyful and sustainable job for clinicians and staff. Our findings suggest that to achieve these aims, primary care transformation will need to address not only the structure of team-based care but also infuse these structures with a spirit of team culture.
Acknowledgments
This research is the result of close partnership with the leadership and staff of 16 primary care clinics across San Francisco. Without the wisdom, expertise, and candid feedback of their clinic leadership, clinicians, and front-line staff, this survey would not have been possible. The study team thanks the San Francisco Department of Public Health and the University of California San Francisco Medical Center for their support of this project in conjunction with primary care reforms undertaken for the Centers for Medicare and Medicaid Services Incentive Program for these health systems under the Section 1115 California Medicaid Waiver.
Notes
This article was externally peer reviewed.
Funding: This work was supported by funding from the California Medicaid Waiver Delivery System Reform Incentive Program to San Francisco General Hospital and the University of California, San Francisco Medical Center.
Conflict of interest: none declared.
- Received for publication July 24, 2013.
- Revision received November 21, 2013.
- Accepted for publication November 27, 2013.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Physician burn-out, transformational and servant leadership
- Caregiving Responsibilities, Organizational Policy, and Burnout Among Primary Care Clinicians and Staff
- The effect of general practice team composition and climate on staff and patient experiences: a systematic review
- Ensuring Community Is at the Table in Family and Community Medicine Research: Highlighting Dr. Kevin Grumbachs Speech as Recipient of the 2022 NAPCRG Wood Award
- Qualitative examination of collaboration in team-based primary care during the COVID-19 pandemic
- Differences in Occupational Burnout Among Primary Care Professionals
- Resource Brokering: Efforts to Assist Patients With Housing, Transportation, and Economic Needs in Primary Care Settings
- Trainee doctors experiences of learning and well-being while working in intensive care during the COVID-19 pandemic: a qualitative study using appreciative inquiry
- Team Configurations, Efficiency, and Family Physician Burnout
- Primary Care Practice Transformation Introduces Different Staff Roles
- Capacity to Address Social Needs Affects Primary Care Clinician Burnout
- A Longitudinal Study of Trends in Burnout During Primary Care Transformation
- Practice Transformation Under the University of Colorados Primary Care Redesign Model
- Primary Care Providers Believe That Comprehensive Medication Management Improves Their Work-Life
- Physician Burnout and Higher Clinic Capacity to Address Patients' Social Needs
- Task Delegation and Burnout Trade-offs Among Primary Care Providers and Nurses in Veterans Affairs Patient Aligned Care Teams (VA PACTs)
- A Randomized Trial of High-Value Change Using Practice Facilitation
- Family Medicine Panel Size with Care Teams: Impact on Quality
- Teamlets in Primary Care: Enhancing the Patient and Clinician Experience
- Estimating the Residency Expansion Required to Avoid Projected Primary Care Physician Shortages by 2035
- Investigating Patient-Centered Care