
Abstract
Background: Purulent skin and soft tissue infections (SSTIs) requiring medical attention are often managed in primary care. The prevalence of SSTIs caused by community-acquired Methicillin-resistant Staphylococcus aureus (CA-MRSA) has been increasing rapidly, including in otherwise healthy individuals. The Centers for Disease Control and Prevention (CDC) issued guidelines to improve the management of SSTIs in primary care.
Purpose: In primary care settings, to assess the prevalence of CA-MRSA using an electronic chart audit and then evaluate SSTI management strategies consistent with CDC guidelines.
Methods: A practical intervention that compared a historical cohort to an intervention cohort of patients seen for SSTI in 16 primary care practices in two health care systems. The intervention included a ready-made kit for I & D procedures, MRSA information for clinicians, a patient information handout, provider education, and patient follow-up.
Results: A total of 3112 SSTI cases (cellulitis or purulent) were observed during the preintervention period and 1406 cases during the intervention. For purulent infections in the intervention period (n = 148), univariate and multivariate analyses showed no significant improvement in the rate of I & D procedures or cultures obtained but showed increased use of antibiotics overall and agents that typically cover MRSA strains (OR, 2.183; 95% CI, 1.443 to 3.303 and 2.624; 95% CI, 1.500 to 4.604, respectively). For infections that were cellulitis with or without purulence (n = 1258), overall rates in the use of antibiotics and those that cover MRSA increased significantly, but secular trends could not be ruled out as an explanation for this increase.
Conclusion: In SSTIs, this intervention resulted in increased use of antibiotics, including antibiotics that typically cover MRSA strains, but did not demonstrate increased rates of recommended drainage procedures. It is replicable and portable, and may improve antibiotic selection in other settings.
- CA-MRSA
- Community-Acquired Infections
- Practice-based Research
- Primary Health Care
- Soft Tissue Infections
Purulent skin and soft tissue infections (SSTIs) requiring medical attention are often managed in primary care. Although these infections account for less than 0.5% of outpatient visits,1 SSTI management is becoming more complex. Staphylococcus aureus is the most common pathogen causing this condition. The prevalence of SSTIs caused by community-acquired methicillin-resistant S. aureus (CA-MRSA) has been increasing rapidly, including in otherwise healthy individuals.2 MRSA was observed in 57.8% of S. aureus in a national laboratory surveillance network.3 A 2007 to 2008 study in Texas primary care practices found that 38% of skin and soft tissue infections cultured positive for MRSA.4 CA-MRSA is a significant public health concern, as it has the potential to develop quickly into an invasive skin infection and cause other life-threatening complications.5–7
Like other SSTIs, most CA-MRSA infections are managed initially on an outpatient basis in primary care settings. The rate of visits to primary care physicians and emergency rooms for abscess or cellulitis nearly doubled from 1997 to 2005.8 Therefore, it is critical that primary care clinicians recognize and appropriately treat potential CA-MRSA infections. Current evidence suggests that although treatments that take into account the possibility of CA-MRSA infections are increasing over time, it is still not the norm. In the National Ambulatory Medical Care Survey (NAMCS) and the National Hospital Ambulatory Medical Care Survey (NHAMCS) datasets, a CA-MRSA-covering antibiotic was prescribed to 28% of patients with an ICD-9 code for cellulitis or abscess in 2005, compared with less than 5% in 2002.8
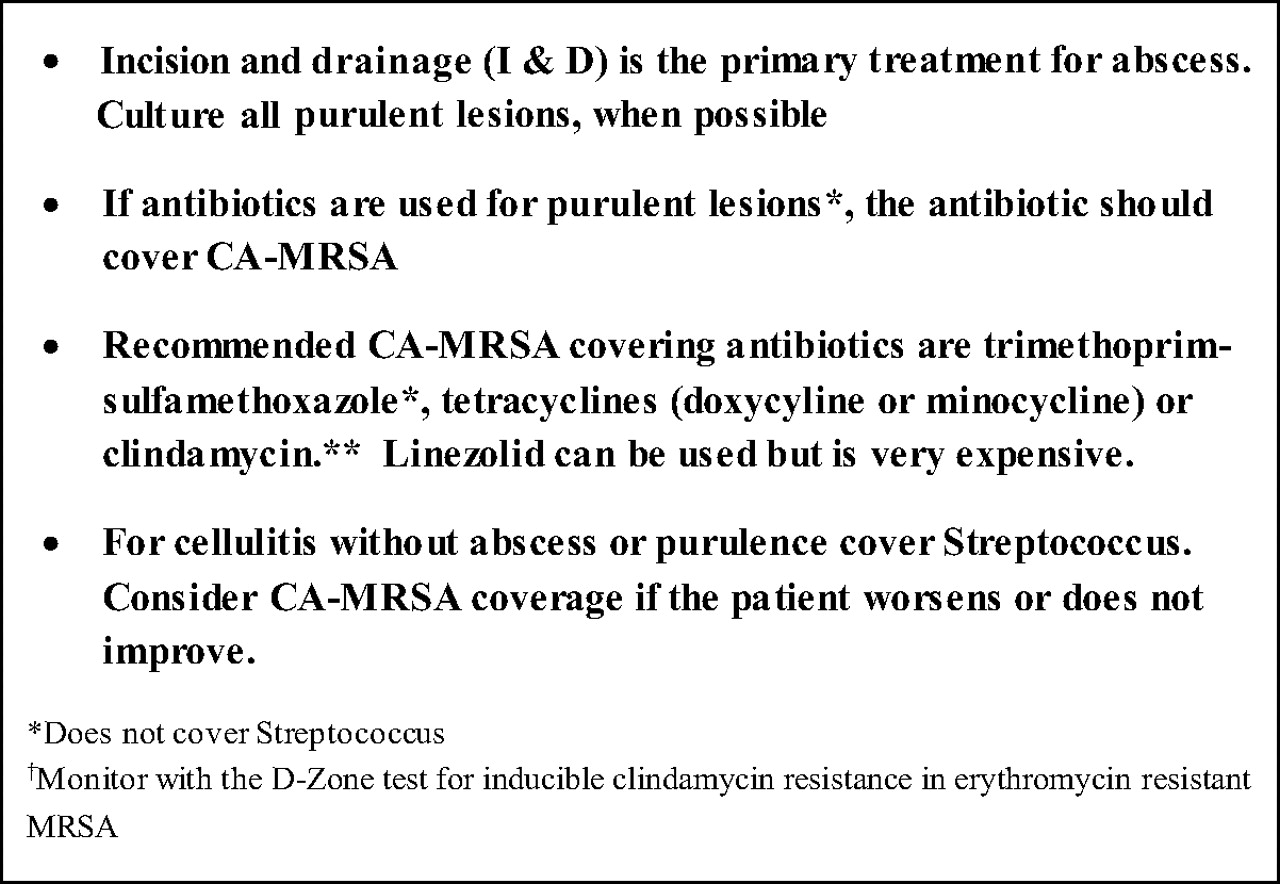
In response to this growing public health problem, the Centers for Disease Control and Prevention (CDC) convened an expert panel and published recommendations and a clinical flow sheet for outpatient management of CA-MRSA.9,10 The guideline recommends, alone or in combination: incision and drainage (I & D), culture of the purulent material, and use of systemic antibiotics when indicated (Figure 1). These CDC recommendations are the same as the recently released Infectious Disease Society of America MRSA guideline recommendations.11 Although the CDC report is widely available, its feasibility and its uptake in busy primary care settings are unknown. A project designed to assess the prevalence of CA-MRSA using an electronic chart audit and then evaluate strategies to manage CA-MRSA consistent with the CDC guidelines was implemented in two health care systems. This article describes the prevalence of CA-MRSA and an intervention to manage it.
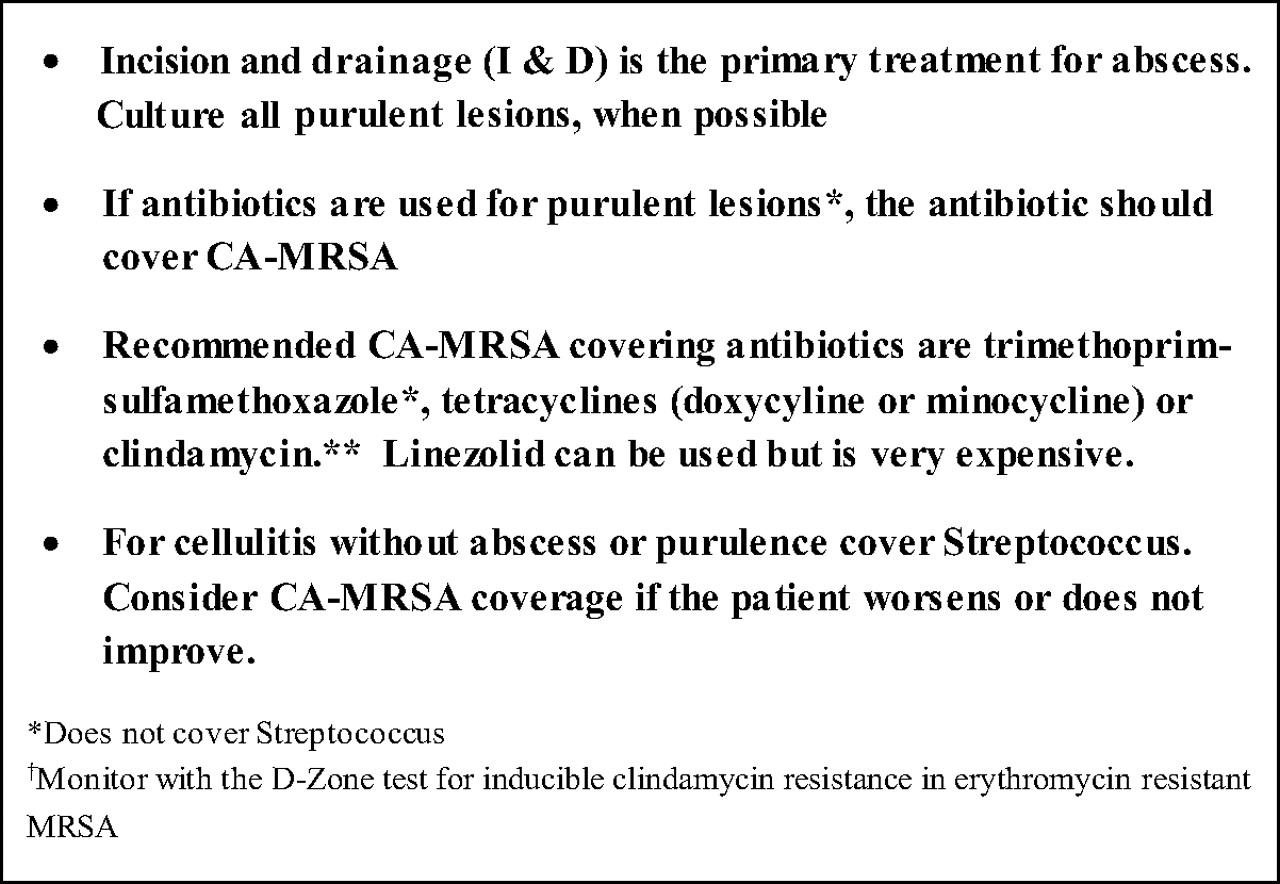
Summary of Centers for Disease Control and Prevention (CDC) community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA).
Methods
Study Design, Setting, and Patients
This study tested a practical intervention in a before versus after comparison. Before the intervention, three focus groups were conducted with between six and nine primary care clinicians from two participating health systems in North Carolina and Texas and a third health system in Denver, Colorado. The focus groups aimed to (1) understand barriers to implementing the CDC guidelines for CA-MRSA, (2) develop feasible intervention strategies to treat CA-MRSA consistent with CDC guidelines in busy primary care settings, and (3) develop outcome measures to assess compliance with the developed strategy. Based on the focus group results, the intervention was developed to address: (1) time constraints, (2) failure to culture or lack of available transport media, and (3) provider concerns about I & D procedures. Such barriers have also been noted elsewhere in recent literature.12 The project team worked closely with the key contacts from the health systems to solve feasibility issues and refine the specific intervention strategies. The intervention included a ready-made tray/kit for I & D procedures with MRSA provider information and a patient information handout, provider education, and patient home care instructions. Analyses from the focus groups were used to develop the kit and patient/provider documents; the documents were also based on the CDC guidelines. Providers were invited to an educational session on CA-MRSA, either given by a local Infections Disease expert (North Carolina) or by an expert from Colorado via live interactive internet (Texas).
The study took place in 16 primary care practices in two health systems. Clinicians included family physicians, general internists, and general pediatricians. One system is a large group practice in Texas with 35 practice locations and approximately 120 clinicians. Ten primary care clinics participated from this health system. The other system is a multispecialty group practice in North Carolina, with approximately 100 total clinicians, of which approximately 35 are in primary care. Six clinics were included from this health system. Both systems used electronic health records (EHRs).
Patients included in the study were seen for an SSTI in one of the participating clinics during the 12-month historical period (November 2007 to October 2008) or the 6- to 7-month (October 2009 to April 2010) intervention period, and included patients of all ages. Our hypotheses were based on the CDC recommendations, specifically that in SSTI cases, the intervention would increase the likelihood (1) of a drainage procedure being performed, (2) of a culture being obtained, and (3) that if an antibiotic was prescribed, it would cover CA-MRSA strains in areas where CA-MRSA is prevalent.
This study was reviewed for human subjects protections and approved by the Colorado Multiple Institutional Review Board and by the American Academy of Family Physicians Institutional Review Board.
Data Collection
To assess baseline and intervention results, we used a novel electronic data collection system, the Distributed Ambulatory Research in Therapeutics Network (DARTNet). DARTNet is an electronic practice-based network designed to facilitate research and examine outcomes associated with prescription medications and devices.13 A federated network links geographically and organizationally separate databases so that a single database query can return results from multiple databases while maintaining the privacy and confidentiality of patient data. Patients' electronic health records were queried for SSTI diagnostic codes by a third party with appropriately executed business associate agreements with the participating health systems. The ICD-9 codes for infections of skin and subcutaneous tissue included 680.x (carbuncle and furuncle), 681.x (cellulitis and abscess of finger and toe), or 682.x (other cellulitis and abscess). The 680.x codes are purulent infections that can be drained (hereafter called “purulent infections”), whereas the 681.x and 682.x codes refer to cellulitis that may or may not have a purulent (abscess) component, and thus may or may not be amenable to a drainage procedure (hereafter called “cellulitis with or without purulence”). Additional data elements necessary for this study were also provided for each case and included procedure data, culture results, prescribed medications, and certain demographic data (nonidentifiable). De-identified data were provided to the research team for analysis. Because the data were abstracted electronically and were de-identified before reaching the research team, no patient consents were required.
Analyses
Descriptive statistics including frequencies and percentages characterized the historical and intervention data. For the primary outcomes, bivariate χ2, Student t tests, and Fisher exact tests were conducted to compare preintervention and intervention electronic chart audit data. Generalized Estimating Equations (GEE) with exchangeable variance-covariance structures were used to model the odds of a patient receiving a culture, a drainage procedure, an antibiotic, and an agent that typically covers MRSA strains (trimethoprim-sulfamethoxazole, doxycycline or minocycline, clindamycin, linezolid) while accounting for correlations due to clustering of patients within providers. Independent variables included in the models were sex, child or adult status, the presence of diabetes, a history of previous skin infection, the health care system through which services were received, and the specialties of the providers who delivered the services.
A longitudinal growth model was used to determine whether evidence existed for the increasing use of antibiotics or agents that typically cover MRSA strains across the population of patients served during the November 2007 through October 2008 historical control period. To hold constant the impact of the historical data, a piecewise GEE model was used to determine whether the odds of antibiotics generally and ones that typically cover MRSA strains use were greater during the intervention period.
Results
The electronic chart audit resulted in a total of 4518 SSTI cases during this study, including 3112 during the preintervention period and 1406 cases during the intervention. The lower number of cases during the intervention was in part because the intervention period was 6 to 7 months, whereas the preintervention period was 12 months. The demographics of the cases are presented below (Table 1).
Characteristics of All Skin and Soft Tissue Infection Cases (680.x - 682.x) in Both Health Systems for the Preintervention and Intervention Periods
In total, there were 316 cultures that were positive for S. aureus in the two systems, of which 208 (65.8%) were MRSA. MRSA was highly prevalent in both systems before the intervention and did not substantially change during the intervention period.
Univariate Analysis of SSTIs
The univariate findings for procedures and cultures were performed only on purulent infections (680.x). The majority of cellulitis with or without purulence cases (681.x-682.x codes) are likely cellulitis without purulence, for which procedures and cultures would not be indicated. In the intervention period, there was a significant decrease in the procedure rate in North Carolina clinics and the combined systems, but not in Texas clinics (Table 2). Overall, the procedure and culture rates were low.
Preintervention and Intervention Rates for Procedures, Cultures, Prescribed Antibiotics, and Methicillin-resistant Staphylococcus aureus (MRSA) Covering Antibiotics of Purulent Skin and Soft Tissue Infections (680.x)
For antibiotic usage and antibiotic choice (whether MRSA was covered when antibiotics were prescribed), the univariate analysis was performed separately on purulent infections (680.x,Table 2) and cellulitis with or without purulence (681.x-682.x,Table 3) to assess rates of prescribing. (1) any antibiotic and (2) antibiotics that typically cover MRSA infections. This decision to perform separate analyses was based on the CDC recommendation to consider no antibiotics for adequately drained purulent infections, but if antibiotics are used, to select agents that cover MRSA. In contrast, the majority of cellulitis with or without purulence infections are cellulitis only for which antibiotics are clearly indicated, but coverage for MRSA is less imperative, according to the CDC guidelines. Compared with the preintervention period, during the intervention period, antibiotic use increased in the combined systems for both ICD-9 groupings (Tables 2 and 3). Interestingly, in cellulitis with or without purulence, the proportion of antibiotics that typically covered MRSA strains increased significantly in North Carolina clinics and the two systems combined, with a trend for increased MRSA coverage in Texas clinics.
Prescribed Antibiotics and Methicillin-resistant Staphylococcus aureus (MRSA) Covering Antibiotics for Cellulitis and Abscess Skin and Soft Tissue Infections (681.x - 682.x)
Multivariate Analyses
The multivariate analysis, when adjusted for patient demographic and clinical characteristics, revealed a number of patterns. The intervention had no significant effect on the number of cultures obtained or the number of drainage procedures performed, although there was a trend for a decrease in procedures. However, the intervention more than doubled the odds of a provider prescribing antibiotics, including an increase in agents to treat MRSA, for purulent infections. Other significant associations in purulent cases included that patients treated by mid-level clinicians had a higher odds of having their infection cultured compared with family physicians, men were more likely to have drainage procedures and cultures, and patients with diabetes had lower odds of having had antibiotics prescribed (Table 4). For both purulent infections and cellulitis with or without purulent infections, patients in the Texas clinics had higher odds of receiving antibiotics and these agents were more likely to cover MRSA, compared with patients in the North Carolina clinics (Tables 4 and 5). From the longitudinal growth model analysis, secular changes did not account for the increase in antibiotic use or agents that typically cover MRSA strains during the intervention in purulent cases.
Among 680.x Cases, Odds Ratios for Procedure, Culture, Prescribed Antibiotics, and Prescribed Methicillin-resistant Staphylococcus aureus (MRSA) Covering Antibiotics (n = 441)
Among 681.x-682.x Cases, Odds Ratios for Prescribed Antibiotics and Prescribed Methicillin-resistant Staphylococcus aureus (MRSA) Covering Antibiotics (n = 4077)
Among cellulitis with or without purulence cases, the piecewise GEE model indicated that the intervention resulted in an increase in antibiotic and agents that typically cover MRSA strains (Table 5, “Intervention Period Monthly Change”). However, in contrast to purulent infections, a significant secular increase in antibiotics and antibiotics that cover MRSA was also found during the historical period (Table 5, “Historical Period Monthly Change”). There was a 12% per month increase in the odds of receiving an antibiotic and a 13% per month increase in the odds of receiving an agent that typically cover MRSA strains during the intervention period. These increases were only 5% and 4%, respectively, during the historical period. Despite the greater monthly increase during the intervention period, this increase was not statistically significant compared with the historical monthly increase (p = .0539 for antibiotics and p = .1220 for agents that typically cover MRSA strains). Therefore, it is possible this increase in antibiotic use may have resulted from a secular trend rather than the intervention.
Discussion
The intervention was designed to optimize treatment for SSTIs consistent with the CDC CA-MRSA guidelines. Specifically, we looked for changes in rates of I & D procedures performed, cultures obtained and use of antibiotics that covered MRSA. When 3112 preintervention SSTI cases were compared with 1406 intervention-period cases, overall procedure and culture rates were low. A trend toward a decrease in the overall procedure rate was observed. Unmeasured clinical considerations, such as lesion size, depth, and degree of fluctuance may drive decisions about drainage procedures more than the suspected etiology of the infection. If true, then an intervention aimed at increasing MRSA awareness might not be expected to increase procedure rates. It is possible that increasing awareness of MRSA across the population may have resulted in patients presenting earlier in the course of their illness over time during the intervention period, compared with the preintervention period. Because early purulent infections are less likely to need drainage procedures, this might explain the trend toward a decrease in procedure rates during the intervention. In this context, it is interesting to note that men were twice as likely to receive a drainage procedure; perhaps this is because men are less likely to see a doctor for any complaint and may present later in the course of an SSTI. Finally, based on discussions with providers regarding this quality improvement (QI) activity, we expected the procedure rate to be substantially higher, suggesting the possibility of data capture problems. Reasons for this may include: the clinician does not bill for it (this may be more common for aspiration procedures which are a more minor procedure); the patient is referred to a specialist or emergency department and a procedure is subsequently performed but not captured in the primary care office; and the intervention period coincided with the peak of the 2009 H1N1 influenza epidemic when practices reported very high patient volumes, resulting in deferred procedures whenever clinically feasible. If the majority of procedures were not captured, then the trend toward a decrease in the procedure rate may be a spurious finding. Future studies could investigate the potential discrepancy between procedures performed compared with electronic data capture, such as by using point of care data collection by the clinician or other staff as the “gold standard.”
The CDC recommends that providers culture all purulent infections, but the intervention did not increase culture rates significantly. Cultures are important for MRSA disease surveillance, yet the culture may have little impact on the care of an individual patient, especially if antibiotics that typically cover MRSA strains will be prescribed anyway. Providers may be more aware of increasing MRSA prevalence, so it may be reasonable to expect little or no change in clinician behavior on drainage procedures due to the intervention (and therefore culture rates, which are tied to drainage procedures), because that is already standard of care. Finally, similar to the discussion of procedure rates above, culture rates were unexpectedly low and likely were not fully captured in the electronic dataset, and significant changes in the culture rate could be missed. Interestingly, the culture rate was higher than the procedure rate, which suggests that in some cases, cultures may have been obtained from spontaneous drainage even though there was no procedure performed.
CDC guidelines recommend I & D as the primary treatment for purulent infections and when systemic antibiotics are used, they should cover MRSA. Antibiotics are recommended for the treatment of cellulitis; however, the CDC notes that the role of MRSA in cellulitis is uncertain. Compared with the preintervention period, during the intervention period, antibiotic use increased significantly for purulent infections, and the proportion of prescribed antibiotics that typically covered MRSA strains also increased significantly. However, for cellulitis with or without purulence infections, the increases found were possibly due to secular trends. The increasing prevalence of MRSA or increased awareness of its prevalence may have influenced clinicians to change their prescribing behaviors, including prescribing more often, as well as preferentially selecting antibiotics that typically cover MRSA strains.
Limitations
Data
Although data were extracted electronically from EHRs, there are limitations with regard to the accuracy and completeness of the data. As discussed in the Methods, there are potential inaccuracies in identifying purulent versus nonpurulent infections based on ICD-9 codes, both because the codes themselves overlap, and because clinicians may code inaccurately. Billing codes were used to determine if a procedure was done, but there may be inaccuracies in the data due to billing data being separate from EHR data. EHRs allow for manual entries of prescribed drugs and can contain misspellings, incomplete words, or non-standard entries, and thus we may have missed detecting some antibiotics. Also, handwritten prescriptions for antibiotics could have been missed. Although we do not believe these data limitations were different during the preintervention and intervention periods, it is possible, for example, that providers who were not billing as much for procedures in the historical period increased their coding during this QI project (or vice versa).
Intervention
The study team for this QI project was based in Kansas and Colorado, remote from where the intervention was conducted in North Carolina and Texas. Although there was a study advocate for each system, there was not an identified site director at each clinic. Thus, we are uncertain of the uptake of the intervention, though we regularly followed up with our study advocates regarding the uptake of the intervention components across the systems.
There was a potential ceiling effect for benefit from the intervention, since the prevalence of MRSA was already present in two-thirds of cases before the start of the intervention. This intervention may demonstrate greater benefit in clinics or systems where MRSA is less prevalent.
Finally, the intervention consisted of provider education, a ready-made I & D kit, and point of care informational materials for providers and patients. Although the intervention resulted in an increase in antibiotic use and the use of MRSA antibiotics specifically for purulent infections, we cannot state with certainty which component(s) contributed to these findings.
Study Design
This study used a before-after design. Compared with a randomized trial, secular trends could account for some of the findings. For example, antibiotic use for SSTIs may have been increasing in these clinical systems in the time interval between the historical period and the intervention period, independent of the effect of the intervention itself. However, by using the piecewise GEE model, it was determined that secular changes could account for the findings in cellulitis with or without purulence cases, but not for purulent infections. Additionally, when multiple tests on related outcomes are assessed, it is expected that a number of them could be significant. Because of this, p-values are reported rather than correcting for multiple testing.
Conclusion
For purulent infections, this intervention in the management of SSTIs, consisting of point-of-care patient and provider MRSA materials, a ready-made I & D kit, and clinician education, resulted in increased use of antibiotics, including antibiotics that typically cover MRSA strains, but did not significantly increase the use of recommended procedures and cultures. The intervention is replicable and portable, and may improve antibiotic selection for SSTIs.
Acknowledgments
The authors of this report are responsible for its content. Statements in the report should not be construed as endorsement by the Agency for Healthcare Research and Quality or the US Department of Health and Human Services.
Notes
-
This article was externally peer reviewed.
-
Funding: This project was funded under Contract No. HHSA290 2007 10008, Task Order No. 4 from the Agency for Healthcare Research and Quality, US Department of Health and Human Services as part of the Primary Care Practice-based Research Network Master Contract.
-
Conflict of interest: none.
-
Prior presentations: Portions of this manuscript were presented at the AHRQ PBRN 2010 Annual Conference, Bethesda, Maryland, June 16–18, 2010.
- Received for publication January 18, 2011.
- Revision received June 6, 2011.
- Accepted for publication June 15, 2011.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Do Professional Development Programs for Maintenance of Certification (MOC) Affect Quality of Patient Care?
- An Assessment of the Hawthorne Effect in Practice-based Research
- Journal of the American Board of Family Medicine Sixth Annual Practice-based Research Network Theme Issue -They Just Keep Getting Better and Better