
Abstract
Adderall, consisting of a mixture of amphetamine salts and dextroamphetamine salts, is a prescription drug for attention deficit/hyperactivity disorder (ADHD) and narcolepsy. Labeled or unlabeled use of Adderall is gaining popularity among young children and college students. Although it is rare, Adderall use is associated with myocardial infarction and even sudden death. We report a case of a young man with acute myocardial infarction after taking 2 15-mg tablets of Adderall XR with alcohol and discuss the clinical features, diagnosis, and management of the cardiovascular effect of amphetamine-containing drugs.
Adderall is a prescription drug for attention deficit/hyperactivity disorder (ADHD) and narcolepsy. Adderall XR is an extended-release form of Adderall. It consists of a mixture of amphetamine salts and dextroamphetamine salts, and both are central nervous system stimulants. Although it is rare, Adderall use is associated with myocardial infarction (MI) and even sudden death. We report a case of a young man with acute myocardial infarction after taking 2 15-mg tablets of Adderall XR.
Case Reports
A 20-year-old African American college freshman presented to the emergency department (ED) with chest pain of 2 days’ duration. He stated he was diagnosed with ADHD 2 years prior and was prescribed 15 mg of Adderall XR orally daily. He admitted to not taking it regularly and had not taken it for weeks before this event. In the preceding 3 nights before admission, he reported drinking (whiskey) after studying and before going to bed every night. Two nights before admission, he drank until the early morning hours and instead of going to bed he took 2 tablets of Adderall XR (total 30 mg) to keep himself awake to prepare for an examination that day. Later that afternoon he developed retrosternal chest pain, which was nonradiating, pressure-like in nature, and 4 to 5/10 (0–10 pain scale) in severity. It was accompanied by light headache but not associated with diaphoresis, nausea, or palpitations. After 30 minutes, he took 1 tablet of Tylenol, which relieved the pain a little but never eliminated it completely until 24 hours later when his parent picked him up at the campus and brought him to the ED.
His past medical history was unremarkable except for ADHD, and family history revealed only diabetes in his mother. There was no family history of cardiovascular diseases. He admitted to occasional smoking of cigarettes and marijuana several months ago and alcohol drinking, but denied any other illicit drug use. He had not been sexually active for the last year. He had no known drug allergy and took no other medications other than Adderall XR.
At presentation in the ED, the patient's blood pressure was 121/72 mmHg, heart rate was 87 beats per minute, and respirations were 18 per minute. His chest pain was not relieved after he was given 325 mg of oral aspirin, but his pain did abate 2 hours later after receiving 4 mg of intravenous morphine. Physical examination of the cardiovascular, respiratory, and abdominal systems was unremarkable.
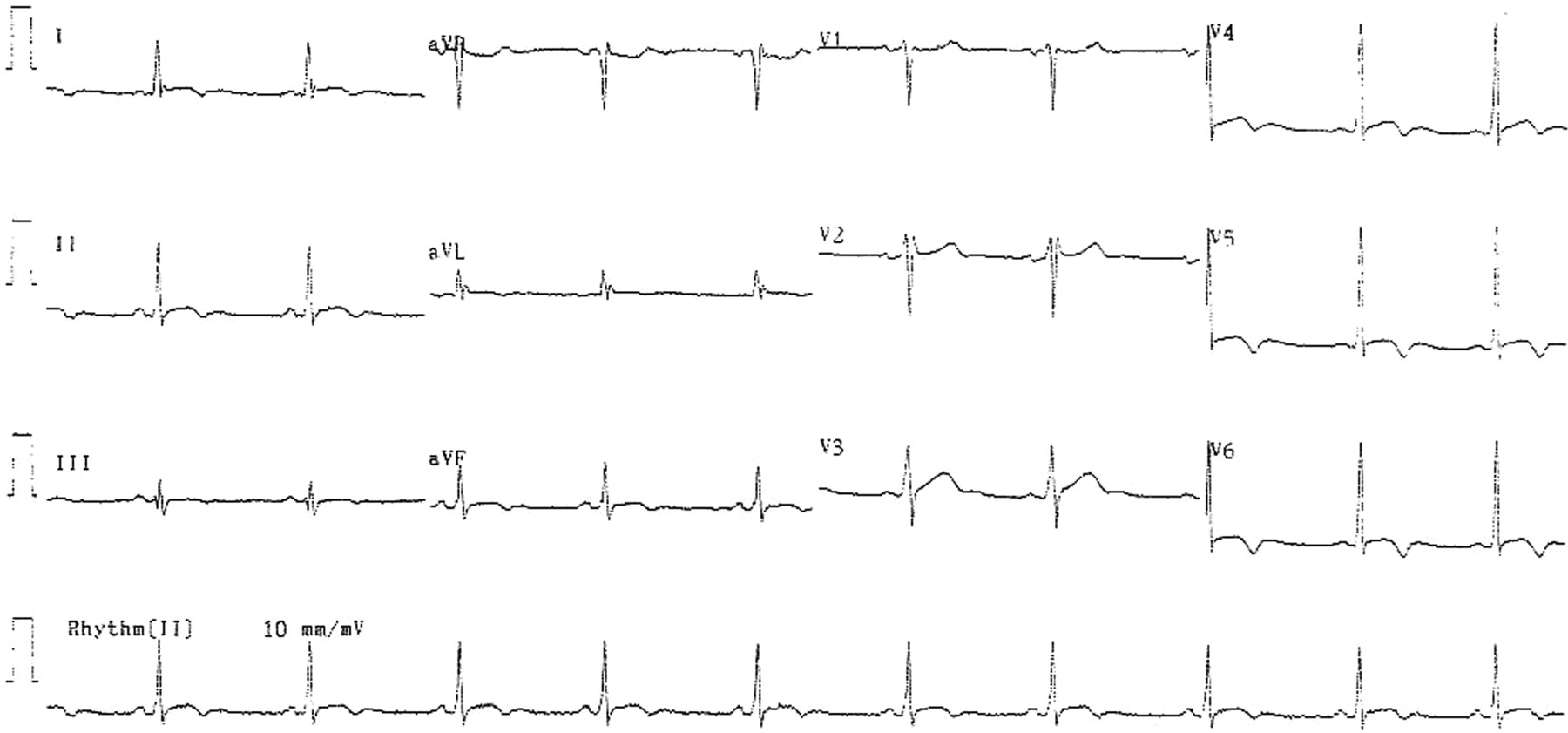
The electrocardiogram (ECG) obtained at presentation (Figure 1) demonstrated elevated ST segment in leads I, II, III, aVF, and V3 through V6. Initial labs revealed elevated CK of 455 IU/L (reference range 25–174 IU/L), Troponin I (TnI) of 3.5 ng/mL (cutoff for MI in this lab is 0.5 ng/mL), normal myoglobin of 35 ng/mL, and urine drug screening positive only for methamphetamine (cocaine, opiates, phencyclidine, methadone, propoxyphene, cannabinoids, barbiturates, and benzodiazepines all nondetectable). Patient was transferred to the intensive care unit and started on intravenous nitroglycerin drip and heparin drip. His cardiac enzyme markers continued to rise to a CK of 564 IU/L, TnI of 4.74 ng/mL, and myoglobin of 131 ng/mL at 2 hours, and the peak levels were CK of 961 IU/L, TnI of 15 ng/mL, and decreased myoglobin of 121 ng/mL at 7 hours after admission. His ESR was 3 mm/h.

A 12-lead electrocardiogram obtained at presentation to emergency department showing ST segment elevation in leads II, III, aVF, and V3 through V6.
Serial ECGs showed more prominent ST elevation in the same leads as well as ancillary leads of V7 through V9 (Figure 2) at 10 hours after admission. The ST segments moved back to baseline on the second day, and T wave inverted on the third day (Figure 3), which was consistent with the evolution of non-Q wave myocardial infarction. Coronary computed tomography angiography performed on the second day and stress echocardiography on third day demonstrated no significant coronary plaque or stenosis, normal left ventricle contractility with ejection fraction (EF) of 58%, and normal ventricular wall motion.

The electrocardiogram with ancillary leads obtained 10 hours after presentation to emergency department showing ST segment elevation in leads II, III, aVF, and V7 through V9.

A 12-lead electrocardiogram on the third day after admission showing evolution of ST segments with inverted T waves in leads II, III, aVF, and V4 through V6.
The final diagnosis was myocardial infarction most likely secondary to amphetamine- induced coronary vasospasm. Patient was discharged on the fifth day on 81 mg of oral aspirin and 2.5 mg of Norvasc daily with instruction of avoiding any drug containing amphetamine.
Discussion
Attention deficit/hyperactivity disorder (ADHD) is the most common neurobehavioral disorder affecting approximately 5% to 10% school-aged children. Although it was previously thought to remit largely in adolescence, a growing literature supports the persistence of the disorder and/or associated impairment into adulthood in a majority of cases.1 Methylphenidate and amphetamine-containing drugs are mainstream in ADHD therapy, and the former is more commonly prescribed than the latter because it is associated with fewer side effects.2
Amphetamine is a sympathomimetic agent that stimulates catecholamine release, particularly dopamine and norepinephrine, from the presynaptic nerve terminals. Methamphetamine (MET) and methylene 3,4 dioxymethamphetamine (MDMA) are derivatives of amphetamine with different potency. MET,3 also called “ice,” “crystal,” or “crank,” and MDMA,4 called “Ecstasy,” “XTC,” “E,” or “Adam,” are among the fastest growing illicit drug problems worldwide. Overuse or misuse of prescription drugs containing amphetamine (such as Adderall) are also gaining popularity with college students because of the benefit of these drugs in promoting wakefulness, heightening energy, and enhancing performance.
It is well known that several complications have been associated with acute and chronic illicit use of amphetamines either orally, inhaled, or intravenously. Tachycardia and hypertension are the most common acute cardiovascular effects. In addition, cardiomyopathy,5 cardiac dysrhythmias,6 cerebral infarction7 or intracranial hemorrhage,8 cor pulmonale with pulmonary hypertension,9 and necrotizing vasculitis10 have been described. Although less frequently than cocaine, amphetamine/MET/MDMA are well documented to cause myocardial infarction.3,4,11–16 Turnipseed et al11 reported a series of 33 patients who presented to their ED with chest pain and methamphetamine abuse. An acute coronary syndrome (ACS) was diagnosed in 25%. Waksman et al12 reported 1 case and reviewed 8 other cases in the literature in which amphetamine use was associated with myocardial infarction. Most of these studies used typical ECG changes with elevation of CK-MB or myoglobin as criteria for acute coronary syndrome. Recently, 4 additional reports adopted the more specific marker TnI (peak level 3.1 ng/mL, 10.68 ng/mL, 18.8 ng/mL, and 362 ng/mL, respectively) to diagnose myocardial infarction associated with amphetamine use.13–16
The mechanisms for amphetamine-induced cardiac injury are postulated to be similar to those seen with cocaine, which include coronary spasm, prothrombotic state, accelerated atherosclerosis due to endothelial injury, and direct myocardial toxicity.3 In a young, acute user without other cardiovascular risk factors, coronary vasospasm (either epicardial or microvascular) is the predominant reason for cardiac injury as in our case.3 However, in the frequent or chronic user and patients with underlying coronary pathology, thrombosis formation and coronary occlusion with or without vasospasm should be considered until proven otherwise.4,16
Management of amphetamine-induced MI should consist of serial ECGs and cardiac enzymes including TnI for early recognition of cardiac injury, early aggressive vessel dilation with intravenous nitroglycerin, and calcium channel blockers and antiplatelet agents. Beta blocker should be avoided for possible unopposed alpha receptor stimulation. Anticoagulation also should be initiated and can be discontinued when thrombotic occlusion is reasonably ruled out by subsequent imaging studies.
A single use of prescribed Adderall without intention to overdose as a cause of MI is extremely rare, and to our knowledge this is only the second report.13 In our case, concurrent alcohol use and the sudden double dose of Adderall may have contributed to its toxicity. Alcohol competes with amphetamine for the metabolizing enzymes in the liver, therefore enhancing the bioavailability of amphetamine. Dosing of Adderall should also be gradually increased from the minimal dose on starting or resuming. If discontinuation is warranted, the dose should be tapered (instead of stopped abruptly) to avoid withdrawal symptoms.
Summary
Labeled or unlabeled use of Adderall is gaining popularity among young children and college students. There are no baseline screening guidelines before prescribing Adderall, but physicians need to be aware that Adderall is contraindicated in patients with known structural heart abnormality, arrhythmia, or hypertension. Inappropriate dosing or taking with alcohol increases the risk of serious cardiovascular side effects like myocardial infarction even without underlying cardiovascular risk factors. Patients presenting with chest pain after taking amphetamine drugs need be evaluated for MI and managed by vasodilating drugs immediately.
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: none declared.
- Received for publication January 6, 2008.
- Revision received May 31, 2008.
- Accepted for publication June 3, 2008.




{kind=link}
{kind=link}
{kind=link}