
Abstract
Purpose: The goal of this study was to determine which approach to assessing understanding of medical information patients most prefer and perceive to be most effective.
Methods: Two videos were shown to participants: (1) a physician explaining a medical condition and its treatment and (2) a physician inquiring about patient understanding of the medical information the patient had been given using 3 different types of inquiry: Yes-No, Tell Back-Collaborative, and Tell Back-Directive.
Results: The Tell Back-Collaborative inquiry was significantly preferred over the other 2 approaches.
Conclusions: Patients strongly prefer the Tell Back-Collaborative inquiry when assessing their understanding. We recommend that physicians ask patients to restate what they understand using their own words and that they use a patient-centered approach.
There is considerable evidence that many patients leave medical encounters with a poor understanding of their disease and the recommended treatment. Hewson1 found that, when patients were asked to explain what had been told them, their explanations included so many gaps and errors that half of the information they had been given was lost. Several early studies substantiated poor understanding of medical information, with reports of lost information ranging from 46% to 63%.2–7 More recently, a study of 20 general practices in England reported that misunderstandings associated with actual or potential adverse outcomes occurred in 80% of consultations.8 A study of patient retention of information given during consent for mammoplasty found that patients were able to recollect on average 3 of 12 pieces of the information given them, or only 25%.9 In another study, patients were asked immediately after discharge from the emergency department about diagnosis and treatment recommendations; although 79% of patients gave the correct diagnosis, correct treatment information was given by only 49% of patients.10
There is a high cost for inadequate understanding of medical information for the patient, the physician, and society as a whole. For patients, misunderstanding can lead to a lack of adherence to treatment recommendations with concomitant adverse health outcomes, as well as decreased satisfaction with the clinician and the medical encounter.8,11,12 Physicians who fail to check for patient understanding of medical information may increase their risk of malpractice claims.13 Finally, the society as a whole absorbs an estimated $73 billion annually because of misunderstood medical information.14
Despite the prevalence of inadequate understanding of medical information and the value of well-understood medical information, physicians do not typically check for patient understanding. A study of audiotaped patient encounters with primary care physicians showed that patient understanding was assessed only 2% of the time.15 The infrequency of checking for understanding was further documented by the findings of Campion et al16 in a large study about communication skills of physicians completing 3 years of post graduate training. Campion and his colleagues analyzed data from over 10,000 videotapes submitted by 2,094 physicians as part of their certification examination and found that 44.9% of these physicians failed to confirm understanding in 1 of 5 videotapes. Furthermore, 99.7% failed to confirm understanding consistently across all 5 tapes they submitted. These findings are particularly salient because this was a high-stakes examination and because applicants themselves selected these 5 tapes as their “best” work.
Given the importance of patient understanding of medical information, surprisingly few specific recommendations are available in the literature regarding how to approach this task. The Kalamazoo Consensus Statement, developed in 1999 by 21 communication experts representing medical education organizations in North America, identified checking for understanding as part of the core communication skill of “sharing information”, but it did not specify a method for doing so.17 Although many of the communications assessment tools currently used in medical education include an assessment of whether the interviewer checks for patient understanding, none describe in specific detail how that assessment should occur.18
A search of the literature in PubMed using the words “check for patient understanding” yielded 44 articles, none directly related to this study. An exhaustive search of several databases yielded one article, published before the advent of the patient-centered model, with recommendations for checking patient understanding of medical information. In this article, Bertakis11 reported that patients who were “asked to repeat in their own words the information which they had just been given” showed a significant increase in retention of information and satisfaction with their physicians. Based on this finding, the author provided a general recommendation that this method be used across health care settings. However, no specific recommendations were made regarding how the physician should inquire about patient understanding.
Several authors have suggested an “Ask-Tell-Ask” method to improve patient understanding.19–21 This approach entails the following: Ask patients to describe their understanding of their disorders and treatments; Tell them additional needed information in a way that incorporates their perspective; and then Ask what they understand and feel about the information given.
The most recent recommendation was formulated by Weiss22 as a result of insights gained in his personal practice. He recommended having patients reiterate their understanding of medical information rather than simply asking whether they have any questions. He also emphasized the importance of creating a “shame-free” environment by normalizing the difficulty of understanding medical information and specifically inviting patients to ask questions about anything they do not understand.
None of the aforementioned recommendations have provided a specific approach to physician inquiry about patient understanding, nor have any been tested to determine patient preference. The goal of this study was to determine which approach to assessing understanding of medical information patients most prefer and perceive to be most effective.
Methods
This study used the videotape stimulus technique refined in other studies to present to participants an explanation of deep vein thrombosis and its treatment, followed by 3 types of inquiry to check for patient understanding.23–25 Participants viewed videos of 3 types of physician inquiry and then rated the inquiries based on their personal preference and perception of effectiveness.
Variables and Measures
Several factors were taken into consideration during the selection of the medical scenario to be shown in the first stimulus videotape. We wanted a medical scenario that was sufficiently complex to provide a challenge to participants’ understanding. The scenario also needed to provide detailed recommendations that, in a real medical situation, would require the patient's thorough understanding and follow-through. With these requisites in mind, we selected deep vein thrombosis.
The second videotape consisted of physician inquiries about patient understanding of medical information. In developing the inquiries, consideration was given to previous research and common practice, ultimately resulting in the formulation of 3 different types of inquiry: (1) Yes-No, (2) Tell Back-Collaborative, and (3) Tell Back- Directive (see Table 1). The closed-ended question (Yes-No) was selected because it seemed to be the most commonly used. Two forms of open-ended inquiries were included for comparison: one physician-centered and one patient-centered (Tell Back-Directive and Tell Back-Collaborative). Both of the open-ended inquiries included a request for patients to reiterate their understanding of information given to them. This was based on research showing increased comprehension, recall, and patient satisfaction when patients are asked to restate their understanding of medical information they had been given.11,26 In addition, the Tell Back-Collaborative inquiry was specifically formulated to be patient-centered whereas the Tell Back-Directive was designed to be physician-centered. In keeping with patient-centered concepts, the Tell Back-Collaborative inquiry incorporated elements such as addressing patients’ feelings and the sharing of power and responsibility.27 The Tell Back-Collaborative inquiry also incorporated a statement acknowledging the amount of information to normalize the challenge of understanding medical information and to create a shame-free environment, as suggested by Weiss.22 The second open-ended inquiry (Tell Back-Directive) was formulated using a conventional paternalistic approach in which authority and control lie with the physician.27
Types of Physician Inquiry Developed for this Study
In creating the video examples of the 3 types of inquiry, we were cognizant of the importance of both nonverbal and verbal communication. We therefore developed a video example and showed it to a group of communications professionals, who then completed a questionnaire and provided verbal feedback about their observations regarding the equivalency of nonverbal elements of the doctor's presentation in the video. Based on feedback from these professionals regarding their observations of potentially confounding variables in the original tapes, such as inflection, speed, and voice warmth, another videotape series was developed. This version was judged by the authors and consultants to be essentially equal in nonverbal qualities across the 3 types of inquiry.
The same female actor portrayed a physician in all the videos shown to research participants. The presentation order of the 3 types of inquiry (Yes-No, Tell Back-Collaborative, and Tell Back-Directive) was systematically varied to prevent order effect.
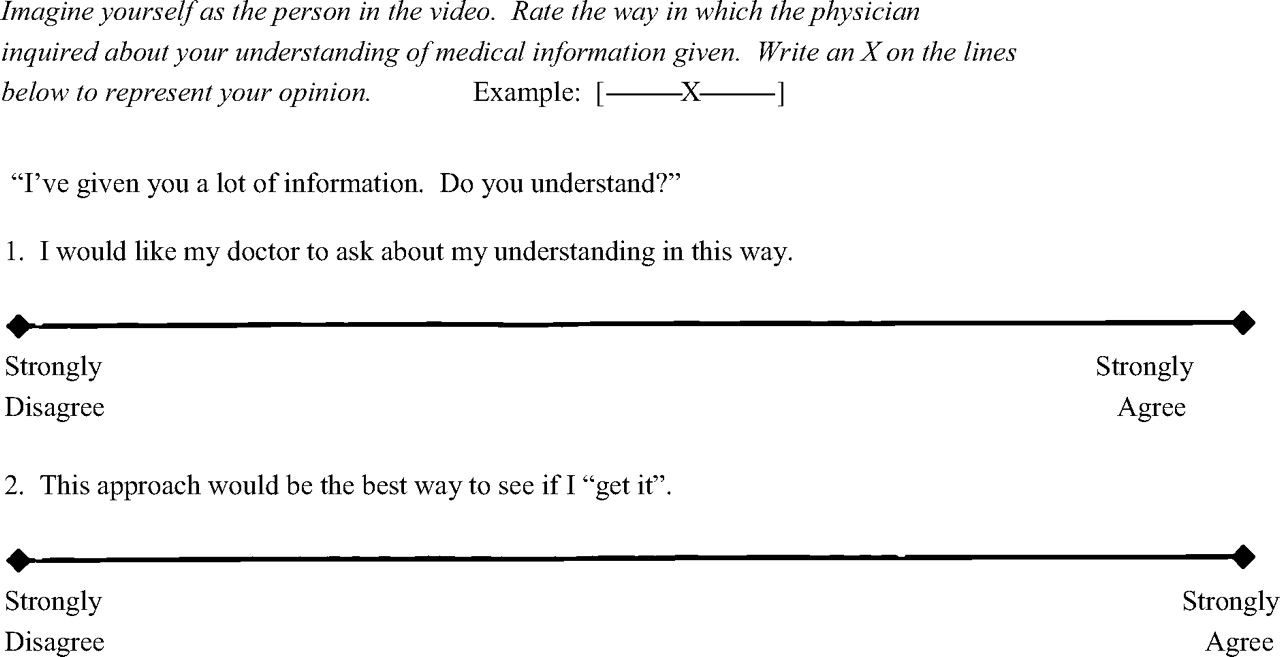
Visual analog scales were used by participants to rate their preference for physician inquiry type and to rate their perception of the effectiveness of each. Each participant received a survey form with the inquiry types presented in the order in which they were viewed. Instructions were at the top of each page followed by the exact wording of the inquiry, with a visual analog scale for preference and a visual analog scale for perception of effectiveness. Participants marked the lines indicating preference for and effectiveness of each inquiry type. The segment between the left point and the mark was measured in centimeters and recorded. The lines were 15 cm in length, resulting in possible scores ranging from 0 to 15. A sample survey form follows (Figure 1).

Sample survey form.
Subjects and Procedures
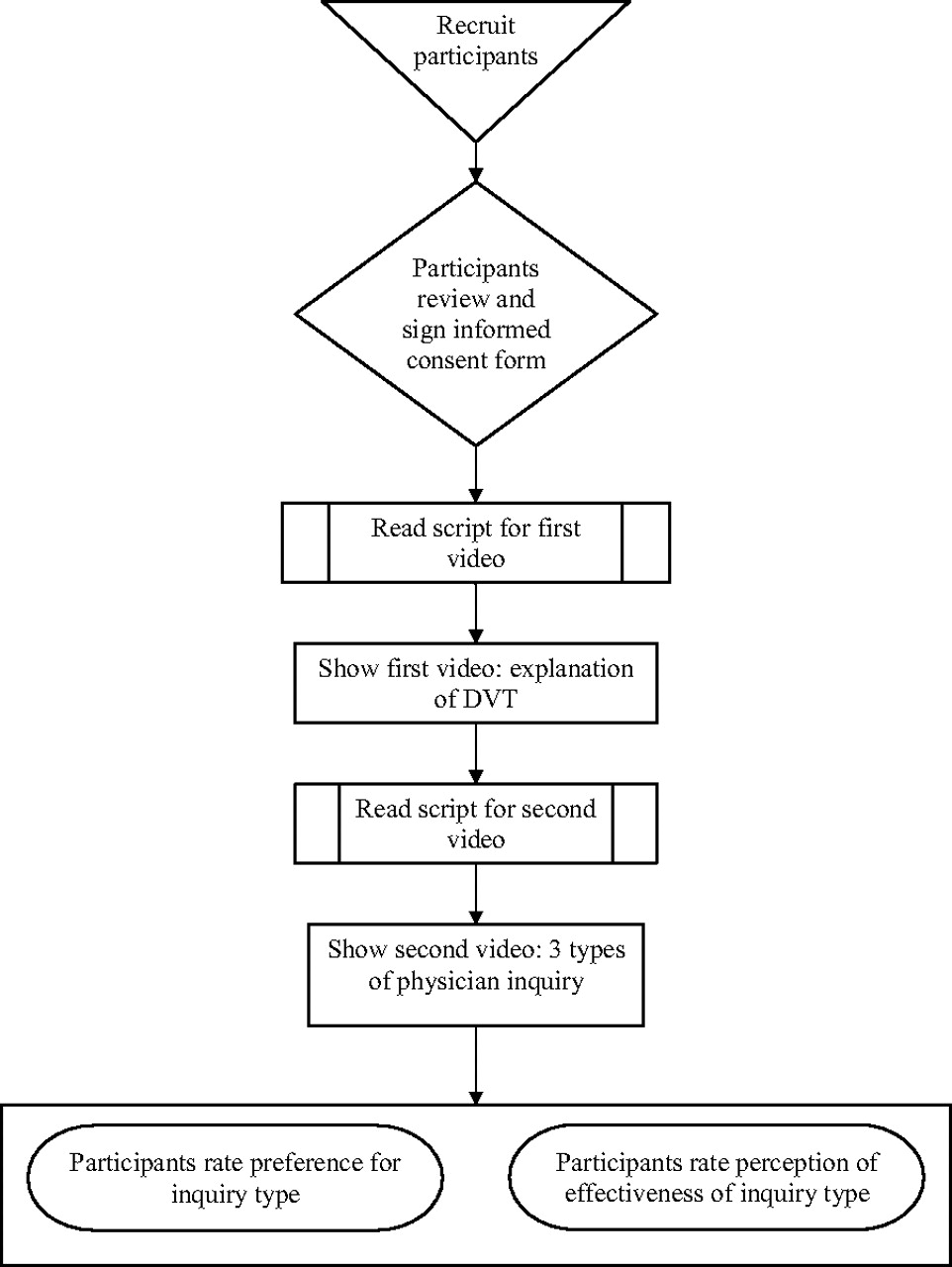
After approval by the Institutional Review Board, a convenience sample was recruited from the waiting rooms of 2 university-affiliated family practice centers in Northeast Tennessee (see Figure 2). Patients over 18 years of age and adults accompanying them were approached by a research assistant and were given basic information about the study. They were told that the nurse would be informed of their location so that participating in the study would not delay them from seeing their doctors. Consenting participants were escorted to a private room to view videotapes and complete measures related to the videos. The research assistant read an introductory script to participants: “I will be showing you a video of a doctor talking with a patient who has a leg problem. Imagine that this is your doctor. She is talking to you about pain and swelling you have been having in your legs. You are very concerned. The doctor is telling you about what she thinks the cause of your pain is, and the treatment she is prescribing.”
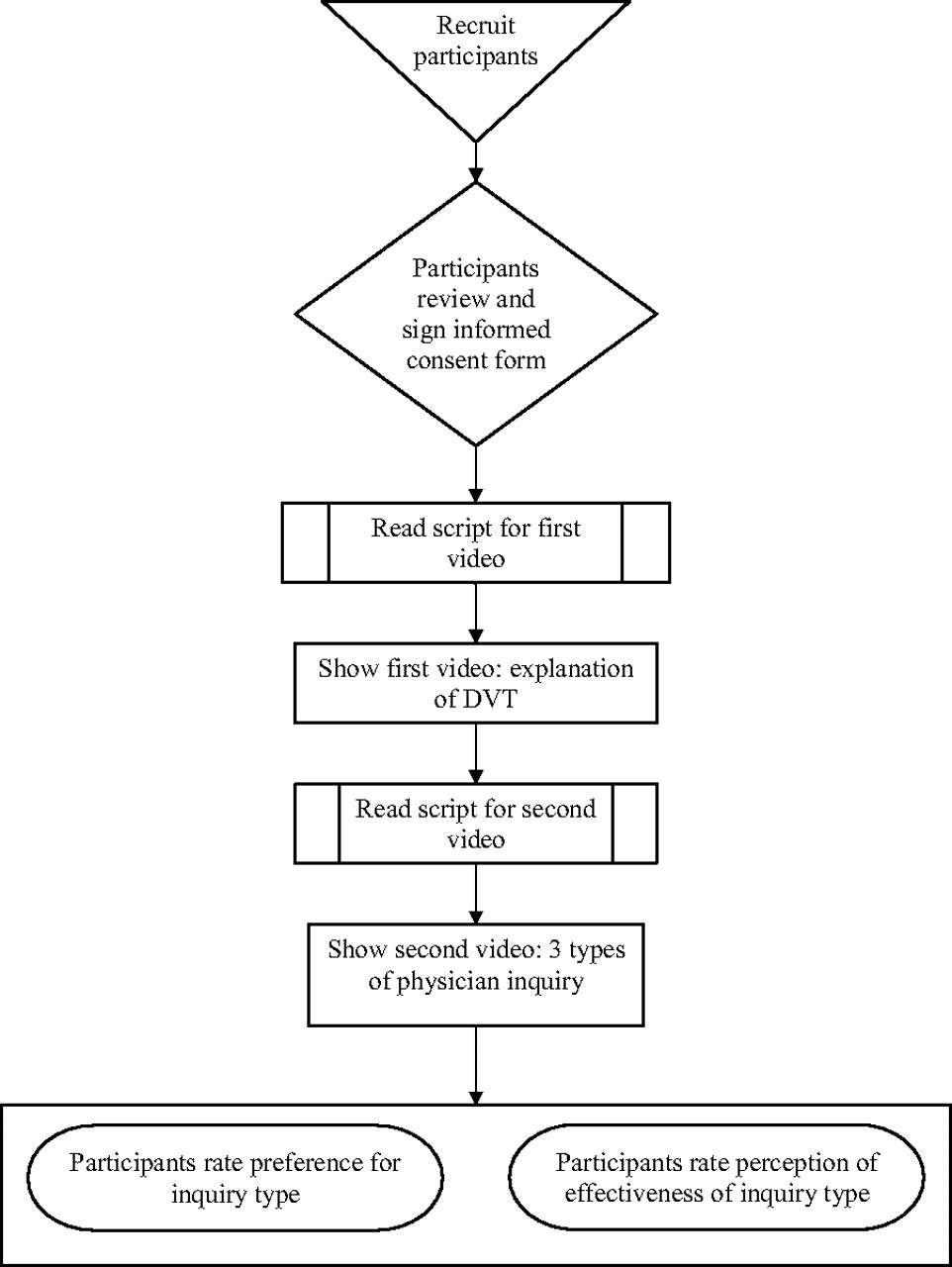
Flow chart of study methods and procedures.
After this introduction, participants were shown a short video of a physician speaking directly to the camera, explaining a medical condition (deep vein thrombosis) and its treatment (enoxaparin, warfarin, and compression stockings). The research assistant then read the following script before presenting a second video: “Now I will show you a video of 3 different ways a doctor can ask if a patient understands the medical information she gives the patient. After you watch the videos, I am going to ask you to rate them on a paper. They are numbered to help you keep them apart, and the paper I give you to fill out will have the words the doctor used in the video to help remind you what the doctor said.”
Immediately after the video showing the 3 types of physician inquiry of patient understanding, participants completed measures of preference and perception of efficacy related to this video.
Results
One hundred eleven adults were approached in the waiting rooms of family practice offices, and 100 (90%) agreed to participate. The sample consisted of 32 men and 68 women; 94 were white and 6 were African-American. Participants ranged in age from 18 to 74 years with an average age of 45 years. Education level varied widely; 12% had grade school or less, 25% had some high school, 37% had a high school education, and 26% had some college or a college degree.
Paired t tests were used to compare the visual analog scale scores of patients’ preference for and their perceived effectiveness of the 3 inquiry types. Regarding preference for physician inquiry, the Tell Back-Collaborative inquiry was significantly preferred to both the Tell Back-Directive inquiry (t = 5.08; P ≤ .001) and the Yes-No inquiry (t = 4.71; P ≤ .001). Results regarding patient perceptions of the effectiveness of inquiry style were similar to participants’ stated preference: Tell Back- Collaborative was perceived to be significantly more effective than Tell Back-Directive (t = 5.67; P ≤ .001) and Yes-No (t = 4.89; P ≤ .001). There was no significant difference between Tell Back- Directive and Yes-No (see Table 2).
Patients' Preference and Perception of Effectiveness of Inquiry Types
Discussion
Patients showed a significant preference for the Tell Back-Collaborative inquiry over all other tested inquiry types. Because of the potential for embarrassment if Tell Back exposed patients’ misunderstandings, one might anticipate that this approach would not be preferred; however, this potential was apparently outweighed by other factors. Preference for the Tell Back-Collaborative inquiry over the Yes-No inquiry might be related to patients’ perception that the Tell Back inquiry helps them remember their medical information.
In contrast to the Tell Back-Directive inquiry, the Tell Back-Collaborative inquiry allows the patient to save face for misunderstandings by acknowledging the large amount of information and by suggesting the reason for assessing the patient's understanding is for the physician's benefit. In other words, part of the appeal of the Tell Back- Collaborative inquiry may be that it serves to create the “shame-free” environment recommended by Weiss.22 Furthermore, patients might view the request for restatement of their understanding as evidence of the physician's care and concern for them personally or as evidence of the physician's attention to detail and competence.
Although patients may understand part, or even most, of the medical information, physicians have no way of knowing what or how much information has been understood and retained unless they ask patients to restate what they understood using their own words (Tell Back). Some might be concerned about the increased time required for Tell Back in an actual clinical situation. A full restatement of an understanding of deep vein thrombosis and anticoagulant recommendations may take some additional time, but this would be more than offset by the time needed to manage complications resulting from a misunderstanding or the potential consequences for the patient who did not “get it straight”. The additional time needed in most clinical situations would be minimal since confirmation of understanding often requires the patient to restate only a single key fact or symptom. For example, asking a patient with strep throat to restate the required length of antibiotic treatment would not take much longer than simply asking whether the instructions were understood.
Because patients typically misunderstand or fail to recall accurately half or more of medical information given to them,1–10,15 it is critical that patient understanding be assessed. Simply asking patients whether they understand or have any questions does not seem to be sufficient. Because they may not understand the situation well enough to formulate a question, patients often answer “no” when asked if they have any questions.22 The inherent power differential between patient and physician may also result in patients being timid or hesitant to ask questions during medical encounters.5
A limiting factor in this study was the artificial nature of the scenario in which participants were not required to respond with their actual understanding. A patient having an embarrassing experience in an authentic clinical situation may express a different preference for inquiry and, potentially, a different belief about its efficacy. Furthermore, participants had not actually been diagnosed with deep vein thrombosis but were only imagining they were real patients. The degree to which they were able to envision themselves as actual patients may have affected the participants’ capacity to understand the information provided by the doctor in the video.
This study is also limited by a lack of diversity among the participants and by the setting. Most of the participants were white, and all were recruited from 2 university-based family practice centers in Southern Appalachia. To determine the generalizability of these results, the study should be repeated within more diverse demographic and geographic practices. The stimulus video portrayed a female physician. Although previous studies involving discussion of sensitive topics such as sexual preference did not demonstrate a gender-related communications preference, gender-specific communication should also be studied.23
Conclusions
Patients prefer to restate their understanding of medical information, a finding that should reassure physicians who might otherwise fear putting patients “on the spot”. Additionally, patients prefer a collaborative approach.
We encourage physicians who currently ask patients, “Do you have any questions?” or “Do you understand?”, to ask instead that patients restate what they understand using their own words. We also recommend that physicians take active steps to normalize the difficulty that patients have in understanding medical information and to take any other steps that might potentially reduce the shame patients may feel in acknowledging their limited understanding. For example, in complex medical situations, physicians could use a variation of the Tell Back-Collaborative inquiry used in this study; eg, “I imagine you're really worried about this clot. I've given you a lot of information. It would be helpful to me to hear your understanding about your clot and its treatment.” With a less complex medical problem, such as the strep throat mentioned earlier, the physician might say, “I know you're anxious to get rid of this bug, and I think we both want to do it right the first time. To make sure we're on the same page, could you tell me how long I'm recommending you take the antibiotic?” Changes based on these recommendations offer great potential to decrease one of the sources of errors in medicine and, simultaneously, to enhance patient satisfaction with the medical encounter.
Acknowledgments
The authors wish to acknowledge medical students Alyssa Turner, Ryan Petering, and Jonathan Hughes for help in data collection; Deborah Pfortmiller, MA, for statistical assistance; and Ivy Click, MA, Ruth Ann Daugherty, MFA, and Amelia Nichols, MS, for their review of the manuscript and helpful comments.
Notes
This article was externally peer reviewed.
Funding: Medical students who assisted with data collection were funded through a HRSA pre-doctoral grant.
Conflict of interest: none declared.
- Received for publication April 4, 2007.
- Revision received June 14, 2007.
- Accepted for publication June 29, 2007.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Enhancing Shared Decision Making Through Carefully Designed Interventions That Target Patient And Provider Behavior
- Focus on Clinical Practice: Improving the Quality of Care
- Comprehending Care in a Medical Home: A Usual Source of Care and Patient Perceptions about Healthcare Communication
- North American Primary Care Research Group President's Award