
Abstract
Objective: Review and examine existing research, current strategies, and directions for future research on smoking cessation relapse and relapse prevention in pregnancy and postpartum.
Methods: A MEDLINE/PubMed search in 2002 and 2003 for articles containing the key words “smoking,” “pregnancy,” “cessation,” and “cessation relapse prevention” and references of retrieved papers yielded a review of more than 500 articles. Only 14 of these addressed program-based strategies to increase cessation among pregnant women through relapse prevention programs.
Conclusion: Although there is much information on the rationale and strategies for smoking cessation for pregnant women, fewer studies exist on how to prevent relapse. Maintaining and accelerating progress in cessation during pregnancy and postpartum requires more research that focuses on relapse prevention and cessation. Programs should incorporate stresses particular to postpartum women, should be part of routine health care, and should involve the woman’s social support network, including her partner, to maximize effectiveness.
Throughout the past decade, tobacco use has remained the single most important modifiable cause of poor pregnancy outcome in the United States. Smoking accounts for 20% of deliveries of infants with low birth weights, 8% of preterm births, and 5% of all perinatal deaths. Smoking during pregnancy and in postpartum contributes to sudden infant death syndrome and changes in brain and nervous system development. The direct medical costs of a complicated birth for a smoker are 66% higher than for nonsmokers.1
Relapse rates range from 70% to 85% among women who smoke but quit at some time during their pregnancy. A recent 10-year study (1987 to 1996) of 8808 pregnant women and 178,499 nonpregnant women of childbearing age indicated that the prevalence of current smoking has decreased significantly among both pregnant (16.3% to 11.8%) and nonpregnant women (26.7% to 23.6%).2 This drop in smoking over time among pregnant women was primarily caused by the overall decline in smoking initiation rates among women of childbearing age, not by an increased rate of smoking cessation related to pregnancy.
Although one fifth of pregnant smokers spontaneously quit by the time of their first antenatal visit,3 and pregnant women are half as likely as nonpregnant women to be smokers,2 an estimated 20.4% of women smokers continue smoking throughout their pregnancies.4 For women who do quit during pregnancy and who received a planned intervention, between 6.2% and 37.2% remained smoke-free. The range of relapse rates is broad because of the varying success of the cessation intervention strategy. Between 29% and 85% of women who get a planned intervention relapse after delivery.5–16
Although there is much information on why and how pregnant women should quit, fewer data exist on how to prevent relapse. This article is a literature review on relapse and relapse prevention in pregnancy; we looked at existing research, current strategies, and directions for future research.
Methods
A MEDLINE/PubMed search was performed in 2002 and 2003 for articles containing the key words “smoking,” “pregnancy,” “cessation,” and “cessation relapse prevention.” As of October 28, 2003, MEDLINE/PubMed indexed 4132 biomedical and life sciences journals. This search yielded a review of more than 500 articles. In addition, references of retrieved articles were reviewed to identify additional sources. All relevant articles were reviewed, with a closer examination of postpartum smoking cessation and relapse. To be included in this review, articles had to address pre- or postnatal relapse prevention or treatment. Articles were also included if they allowed comparisons of women who relapsed versus those who remained smoke free. Of the 146 articles that contained references to postpartum relapse, only 14 specifically described strategies to increase cessation among pregnant women through relapse prevention programs (2 of these 14 articles discussed the same program). Four of the investigators systematically reviewed and analyzed these articles.
Results
Profiles of Women Who Smoke and Are Pregnant
Researchers have reported that specific events, factors, or decisions precipitate a pregnant woman’s resolution to quit (Table 1). Important factors include planned pregnancy,17 morning sickness,2,18 becoming visibly pregnant,2 decision to breastfeed,2,19 personal health reasons,2,3,18 baby’s health,2,3,18 children with asthma or other respiratory problems,17 social pressures,2 guilt,2 advice from a physician or other health care provider,14 participation in a cessation program,9,10,14,15 and a good opportunity to quit.18
Factors Related to Smoking Cessation and Relapse in Pregnancy
According to DiClemente et al,20 pregnant women and their smoking status can be categorized into 3 types: those who quit because they are trying to get pregnant (pregnancy quitters), women who quit immediately after learning they are pregnant (spontaneous quitters), and women who smoke throughout pregnancy (pregnant smokers). Little is known about pregnancy quitters; they are generally labeled as nonsmokers because they quit before their first prenatal assessment, and they are not offered cessation counseling or support. In theory, pregnancy quitters might be more conscientious of their own health and their baby’s health than spontaneous quitters and pregnant smokers and might be dedicated to remaining smoke-free not only for pregnancy but also for life. DiClemente et al20 found that these women typically sustain cessation throughout the prenatal and postpartum period and that cessation rates on follow-up are dependent on their addiction (measured by number of cigarettes smoked per day, length of time between waking and smoking the first cigarette, etc) and motivation to quit.
Spontaneous quitters generally have high cessation rates throughout the pregnancy (80% to 85%). Panjari et al3 found that spontaneous quitters are different from other smokers in a range of demographic variables (ie, race, educational level, income, and employment status), their contented addiction, and beliefs about the risks. However, more than 70% of spontaneous quitters will relapse within 6 months after delivery. High relapse rates occur, in part, because the motivation to quit is fueled by a desire to protect an unborn baby. Many women might not appreciate or be aware of the adverse health effects on children of exposure to environmental tobacco smoke.5,21 Preparing women to move from an awareness of smoking on the developing baby to an effect on themselves is fundamental in maintaining cessation.20,21
Pregnant smokers are more likely to come from the subgroup of women with lower socioeconomic status.20 These women tend to have more psychological and emotional problems, less support and financial resources, more family problems, and less residential security.20,22–30 Low-income pregnant women report “… more stressful events, more perceived stress, more negative appraisal from family, less social support of all types, lower scores on mental health measures, and more addiction to cigarettes. These conditions lower motivation to stop smoking and also self-confidence in an ability to stop.”31
Profiles of Women Who Relapse Postpartum
Those who relapse postpartum tend to be young women who were heavy smokers before pregnancy and women who quit smoking late during pregnancy (in the third trimester).5 Successful quitters tend to be light to moderate smokers,5,6 white, married, young, and educated.32,33 When Edwards and Sims-Jones34 interviewed 22 women who smoked before pregnancy and had relapsed postpartum, 3 themes emerged: pregnancy as a context for stopping smoking, specific events and stressors that precipitated a return to smoking, and social influences on smoking behavior. For those who relapsed, relationship troubles, medical problems, and other stressful events triggered a return to smoking. Other contributors included returning to a nonpregnant state, social pressures, and high-risk situations. Hospitalization after delivery prolonged the smoke-free state, and this period might be a time to reinforce maintenance. Others have found that women with partners who smoke find it more difficult to quit and not relapse (Table 1).9,19,35,36
Some research shows that advantages for smoking cessation focus on the baby whereas disadvantages for stopping are related to the mother.34 The specific events, factors, or decisions that precipitate a woman’s resolution to quit are not necessarily the same as those that trigger a woman to smoke again.
Interventions that Maintain Smoking Cessation during Pregnancy
Most research on smoking cessation and pregnancy has attempted to maintain cessation during pregnancy (Table 2). Programs that support women during this time protect the health of the unborn baby as well as the pregnant mother. Several programs keep high-risk women from smoking during pregnancy but do not track whether the women remain smoke-free after the baby is born.32,37,38 Although factors that cause women to return to smoking after pregnancy are not identical to those causing women to return to smoking while pregnant, it is useful to look at studies of programs that encourage women to quit smoking while pregnant.
Programs that Focus on Postpartum Smoking Relapse Prevention
Ershoff and his colleagues25 outlined 3 possible strategies for maintaining prenatal cessation among women who quit during pregnancy: targeting, triage, and tailoring. Targeting would maximize considerable resources in helping women with low intentions of quitting by simultaneously addressing attitudinal, addiction-related, and environmental barriers. Triage would recognize that health care providers have a finite amount of time and resources to invest in helping pregnant women stop smoking, and a better strategy is to devote more resources to those pregnant smokers with the motivation to quit. Tailoring would recognize the barriers to quitting faced by pregnant smokers with low quitting intentions, acknowledge that the goal of quitting smoking during pregnancy might be unrealistic, and help those women with a harm-reduction approach.25 Harm reduction counsels women to cut down on the number of cigarettes smoked in lieu of complete cessation. This might indeed be a useful strategy when combined with counseling about other healthy lifestyles (eg, healthy eating, daily exercise).20 The smoking status of their partner, close friends, and family affect all women who smoke and are pregnant.20,22,28,39,40
A promising strategy for assisting low-income women is to use stages of change and decisional balance constructs. Bane and her colleagues21 studied participants who completed the general 8-item decisional balance measure (4 pros and 4 cons) plus 8 additional pregnancy-related items (4 pros and 4 cons) to determine this underlying structure of pregnancy-tailored decisional balance measure. The pros addressed the perceived benefits of smoking, such as relaxation and pleasure, whereas the cons concerned the costs, health hazards, and social disapproval. Participants were categorized in the 5 stages of change regarding their smoking status (ie, precontemplation, contemplation, preparation, action, and maintenance). The research confirmed that pregnancy-tailored messages in an intervention program could be an effective way to maximize impact. Lillington9 also reported that culturally appropriate, low-literacy materials are useful in delaying relapse or maintaining cessation.
Various cessation strategies have been offered to aid women in cessation attempts, including monitoring clinical interventions,30 tracking the success of written cessation aids—distributed in clinics11 and via mail37—and training health care providers on cessation interventions.41 Many programs have piggybacked with programs such as Women, Infants, and Children; Medicaid; health maintenance organizations (HMOs), and other organized, standardized, prenatal programs.6,42,43 Some people have tried more unusual methods of reaching pregnant smokers, for example through videotape,42 digitally interactive programs,38 and peer telephone support.30 Most of these programs have combined intervention strategies, hoping to increase success rates.
The general opinion is that clinical and social intervention cessation programs that would be most effective are those that address the needs of the individual woman, address her social network, and are incorporated into routine health care. Health care providers should tailor programs to the individual woman by distinguishing between women with concrete plans to prevent relapse and those who have not considered the possible challenges.34 The programs should also include personal interaction with clinicians and/or support staff.42 Furthermore, providers should educate women about the dangers of exposure to environmental tobacco smoke,5,28 and about the risks of smoking for the woman, not just the baby.21 They should address a woman’s social sphere by increasing community awareness about why women who are pregnant should not smoke,22 encouraging a woman’s social network to support her with positive encouragement rather than negative nagging,30,34,39 and including her partner and others living in the home in any cessation effort.20,25,28,39,40 Programs must be included in routine health care,1,28 and begin as early as possible and last as long as possible, from prepregnancy,20,28 throughout pregnancy,1 immediately after delivery,20 and through breast-feeding.34 Finally, these programs must incorporate the time and financial commitment that successful cessation interventions require.25,37,43
Interventions to Prevent Postpartum Relapse
Relatively few studies have specifically examined cessation throughout pregnancy and postpartum.11,14,18,44–52 The focus of most studies was not specifically on prevention of relapse, but rather on maintaining cessation throughout pregnancy and beyond. These programs were often offered in tandem with broader social service programs.23,24
Although intervention programs that seem effective at preventing postpartum relapse are similar to those that encourage cessation, key differences exist. Programs that successfully reduce postpartum relapse rates, even though they are specifically designed to reduce prepartum smoking rates, are those that include the smoking habits of partners, others living in the home, and close friends;6,31 support women with positive encouragement rather than negative nagging;6,24 understand the time and financial commitment successful cessation interventions require;23 encourage women’s social networks to support her;31 take place throughout pregnancy31 and through early childhood care;15 and distinguish between women with concrete plans for not relapsing and those who have not thought out possible challenges.6
Several themes are elaborated on in studies focusing solely on prevention of postpartum relapse. Through interviews with 27 women, Bottorof et al44 revealed the complex factors that are part of postpartum relapse. They identified 5 general story lines that explain why a woman who had quit during pregnancy might return to smoking after delivery: 1) controlling one’s smoking (starting with one puff, restricting the amount smoked); 2) vulnerability to smoking (inability to resist); 3) nostalgia for former self (freedom and happier times); 4) smoking for relief (to manage emotions and stress); and 5) never really having quit (did not want to quit for themselves).
As noted previously, the woman’s stage of readiness to quit will determine whether she will quit and what cessation approach to use. The percentage of women who returned to postpartum smoking was highest in the precontemplation stage and decreased with each subsequent stage.50 In another study that examined stage of change and use of brief motivational interviewing techniques during prenatal and postnatal visits, Valanis et al51 found that relapse rates were significantly lower than those of women in the comparison group. Other factors that might contribute to postpartum relapse are African American race/ethnicity, multiparity, late or no prenatal care, maternal weight gain, stressful life events,45 and early weaning.49
Many women clearly require unique relapse prevention interventions. Several studies reveal that clinical interventions are the primary method of cessation counseling. A survey of community health center providers scored performance of smoking cessation counseling steps offered to mothers, based on the National Cancer Institute’s 4 A-steps of smoking cessation counseling: assessment of smoking status, advice to quit, assistance in staying quit, and arrangement for a follow-up. This composite measure of providers’ self-reported smoking intervention practices and performance found that providers in obstetrics clinics had the highest performance scores and providers in pediatric clinics had the lowest scores. Nurse practitioners and nutritionists had higher scores than other providers (eg, program staff, obstetricians, and pediatricians). Low scores for performance of steps beyond assessment and advice indicate a need for emphasis on the assistance and arrangement for follow-up steps.53
Another intervention program offered telephone support postpartum by nurses to women at the time of delivery. This program was successful in decreasing relapse rates as well as in decreasing the amount of cigarettes smoked by women who did relapse. The study also found that 4 variables were associated with relapse to daily smoking. Breast-feeding and mental health were protective factors, whereas partners who smoked and the greater amount smoked before pregnancy had adverse effects.18,48
One intervention referred women to individual behavior change counseling during prenatal care in addition to standard cessation counseling from her physician. Although additional cessation counseling did not yield significantly lowered relapse rates, researchers found that greater proportions of the intervention group reported either not smoking or reducing their consumption by 50% or more. Researchers concluded that the following would have an impact on relapse rates: physician training on how to gain a pregnant smokers’ commitment to change her smoking behavior, an office prompt system, and individualized smoking behavior change counseling.14
Not all studies show that advice from clinicians is the only way to offer relapse prevention messages. In a study of 57 low-income, multiethnic mothers and smokers, focus group discussions show that participants valued advice from friends and relatives over advice from professionals. Educational efforts might be most effective when directed at networks of women who share information.46
Although some programs did not see significant increases in postpartum relapse rates, researchers still suggested that successful relapse prevention programs should be added to cessation interventions, with increased duration and potency.11,52 These programs should include messages aimed at bolstering confidence in being able to continue not smoking,52 and be delivered throughout prenatal, postpartum,48 and early childhood care. Finally, these programs should be presented to the woman and her social network by ancillary staff (Table 2).52
Further Research and Recommendations
Based on the work published so far, we believe that clinicians and programs can improve the chances of women staying smoke-free after successful quitting during pregnancy by appropriate assessment and anticipatory guidance. Clinicians can quickly ask pregnant women about their decisions for quitting, their expectations for remaining smoke-free, their social support network, their beliefs about positive impacts of cessation, their potential for relapse, and events specific to the stresses in the postpartum period (Figure 1). For each of these constructs, current intervention research suggests possible answers to improve counseling effectiveness.
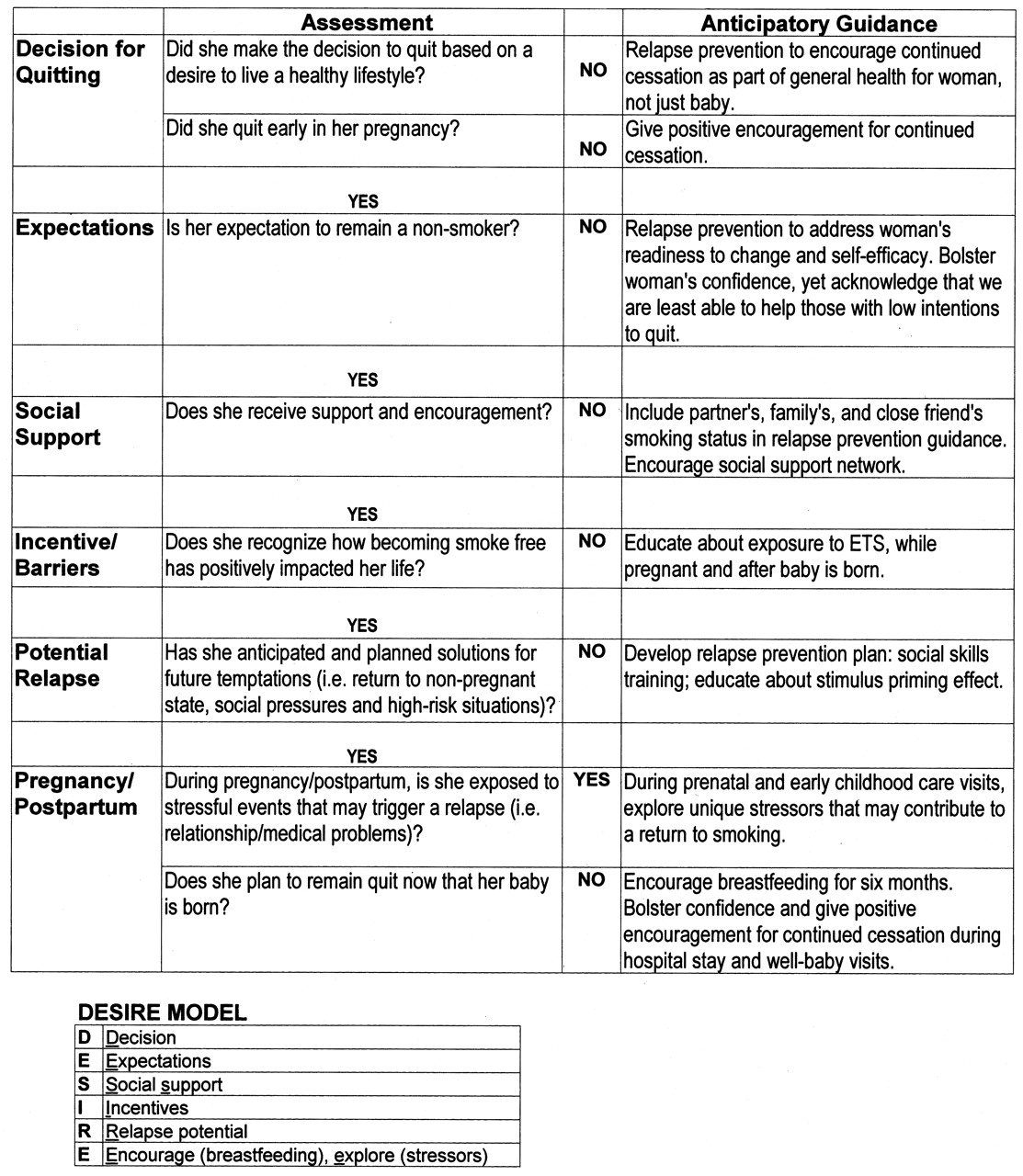
Pregnancy and postpartum smoking relapse prevention.
It is clear that additional research is needed to improve on the high relapse rates for smoking among pregnant women. For instance, research is needed that examines how the following optimally influence relapse prevention: stages of change,17 confidence level,3 perception of level of ease of quitting,3 and support systems.34,41 Interventions that involve the woman’s partner34,41 need further exploration. Some researchers propose extending smoking cessation programs into the postpartum period12,18,34 or as a part of well-baby care.11 The effects, costs, and outcomes of program extension have implications for developing a theoretic model of postpartum relapse and maintenance and for planning and implementing effective interventions.
Recent surveys of clinicians and providers have shown that providers reported low awareness of health risks of smoking to the fetus and child.54 Most providers feel they offer inadequate cessation counseling for women who smoke while pregnant. Those programs that do provide counseling do not assess smoking status before pregnancy or the smoking status of other household members,55 both of which are strong factors in postpartum relapse.
Maintaining and accelerating progress in smoking cessation during pregnancy and postpartum will require more research that focuses on relapse prevention in addition to cessation. To maximize effectiveness, programs should incorporate stresses particular to postpartum women, be part of routine health care, and involve the woman’s social support network, including her partner.
Acknowledgments
We gratefully acknowledge support of our Smoke-Free Families Program from The Robert Wood Johnson Foundation (grant 040668).
- Received for publication November 13, 2003.
- Revision received November 13, 2003.




{kind=link}