
Abstract
Background: Many persons use botanicals and dietary supplements for chronic conditions that do not respond to traditional Western medications. Tricyclic antidepressants, a common treatment option for diabetic neuropathy, can have many side effects and are a poor choice in certain populations (eg, the elderly). As such, patients might turn to botanicals and dietary supplements, not realizing that these products are not well regulated.
Methods: This article reviews botanicals and dietary supplements that have been involved in randomized controlled trials (RCTs) for diabetic neuropathy. We searched MEDLINE for English-language literature dating from 1966 to April 2001 using the following subject headings: (1) diabetes and botanical, herb, and supplement, (2) neuropathy and botanical, herb, and supplement, and (3) diabetic neuropathy and botanical, herb, and supplement.
Results: Our search found agents that might improve symptoms of neuropathy (eg, evening primrose oil, alpha-lipoic acid, capsaicin) without affecting glucose control. Botanicals and dietary supplements involved in only one RCT or associated with little clinical benefit were reviewed in brief.
Conclusions: Evening primrose oil, alpha-lipoic acid, and capsaicin have received the greatest attention for their use in diabetic neuropathy, but further studies are needed to confirm their efficacy. Patients using these products need to be informed of potential drug interactions and side effects.
Peripheral neuropathy is a complication of both insulin dependent (type 1) and non–insulin-dependent (type 2) diabetes mellitus. It is characterized by a progressive loss of nerve fibers that predisposes the patient to painful or insensitive extremities, neuropathic ulceration, and amputation. Affected nerve functions include reduced nerve conduction velocity, decreased temperature sensation, decreased tendon reflex response, and a decreased ability to detect vibration and touch.
Long-term elevation of plasma glucose levels has been established as the definitive cause for diabetic peripheral neuropathy.1 With time, elevated plasma and nerve glucose levels contribute to nerve degeneration by a number of proposed mechanisms. These mechanisms include metabolic changes, such as increased polyol pathway flux, increased formation of oxygen free radicals, and the formation of advanced glycosylation end products.2 Reduced nerve perfusion and decreased production of prostaglandin vasodilators has also been proposed as contributing factors.3 ,4 Although tight glycemic control is the best way to avoid developing neuropathy, not all patients achieve this goal.
In 1994, the Dietary Supplement Health and Education Act, defined a dietary supplement as a vitamin, mineral, herb or other botanical, amino acid, or substance, such as a coenzyme, organ tissue, glandular, or metabolite.5 This article will review some of the botanicals and dietary supplements that might relieve symptoms associated with diabetic neuropathy but do not affect blood glucose control. Currently, these botanicals and supplements for neuropathy are being advertised to patients through various media and over the Internet. The purpose of this article is to review the scientific evidence for products that might benefit neuropathy or its pathologic features, rather than to recommend a particular product.
Methods
We searched MEDLINE for English-language literature dating from 1966 to April 2001 using the following subject headings: (1) diabetes and botanical, herb, and supplement; (2) neuropathy and botanical, herb, and supplement; and (3) diabetic neuropathy and botanical, herb, and supplement. The bibliographies of pertinent articles and reviews on diabetic neuropathy that discussed alternative therapies were searched to find additional references. Randomized controlled trials (RCTs) conducted in humans and involving an herb, botanical, or supplement for diabetic neuropathy were included. Once a product was found, a separate MEDLINE search was performed using the name of that supplement to find additional RCTs.
Dietary supplements and botanicals having more than one RCT for diabetic neuropathy and reporting some favorable outcome were reviewed more extensively. These products included evening primrose oil, alpha-lipoic acid, and capsaicin. Dietary supplements and botanicals having only one RCT or associated with little clinical benefit were reviewed in brief. These products included acetyl-𝓁-carnitine, pyridoxine (vitamin B6), vitamin E, and St. John’s wort.
Evening Primrose Oil
History
Evening primrose oil is extracted from the seeds of Oenothera biennis. Evening primrose oil is a rich source of omega-6 essential fatty acids, primarily gamma-linolenic acid (GLA) and linoleic acid, both essential components of myelin and the neuronal cell membrane. Commercial preparations of evening primrose oil are typically standardized to 8% GLA and 72% linoleic acid.6
Pharmacology
Linoleic acid forms GLA by means of an enzymatic reaction involving Δ-6-desaturase(Figure 1). GLA forms di-homo-gamma-linolenic acid (DGLA), which can be converted to prostaglandin E1 (PGE1) or to arachidonic acid byproducts (eg, series 2 prostaglandins [PGE2], leukotrienes, and thromboxane). PGE1 is preferentially formed, however, because the conversion from DGLA to arachidonic acid is slower.7 PGE1 has anti-inflammatory, antiplatelet, and vasodilating properties. PGE2, leukotrienes, and thromboxane tend to promote inflammation, vasoconstriction, and platelet aggregation.
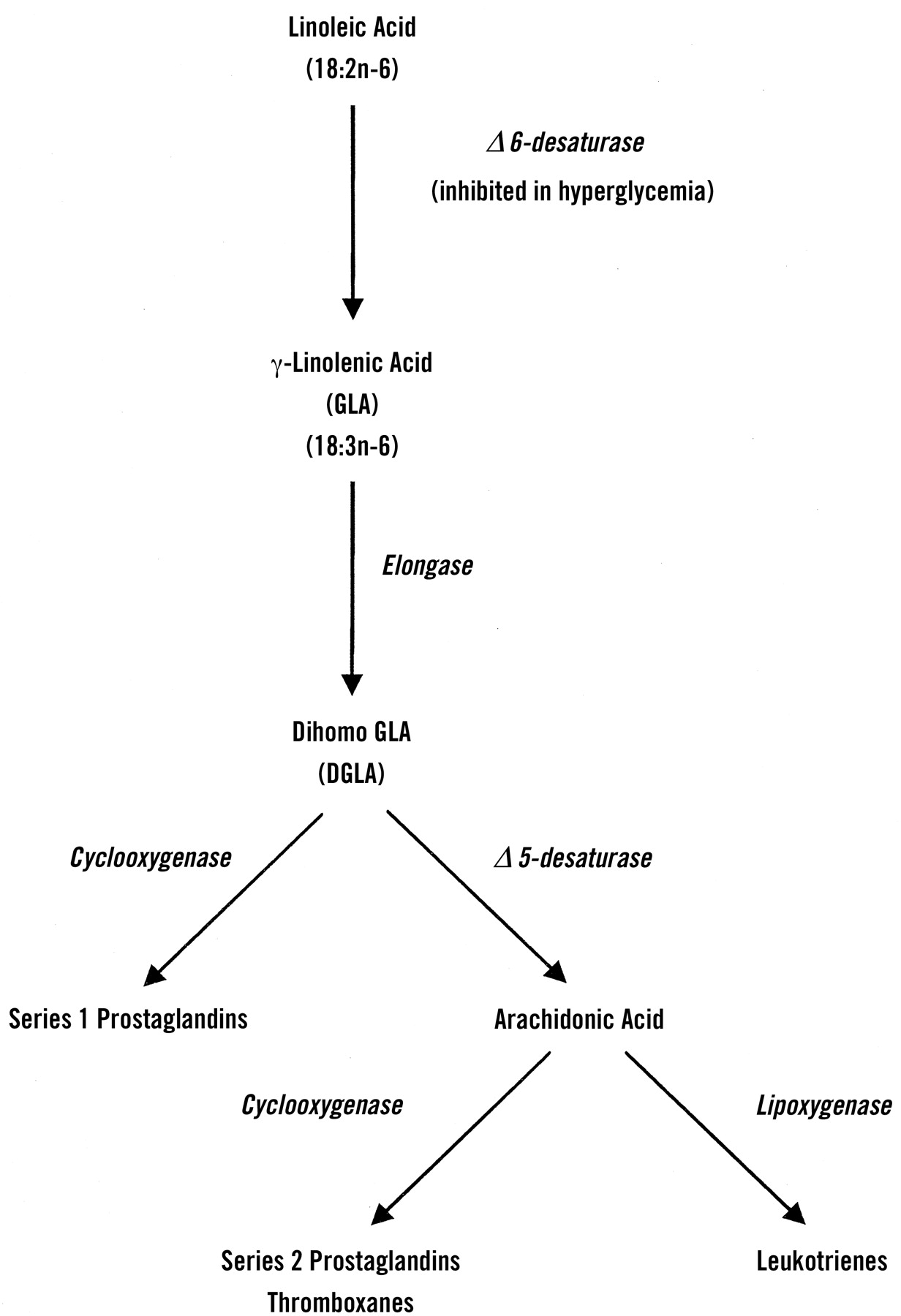
Production of series 1 and 2 prostaglandins from linoleic acid.
The enzymatic activity of Δ-6-desaturase, which is compromised in patients with type 1 and type 2 diabetes mellitus, can decrease the production of PGE1.8 Decreased production of PGE1 has been proposed to enhance the formation of PGE2 and thromboxane.9 As a result, levels of PGE1 are decreased, and levels of PGE2 and thromboxane are increased in patients with diabetes.10
Supplementing the diet with GLA has been shown to augment the production of PGE1 by bypassing the blocked enzymatic step.11 ,12 Supplementation with products rich in linoleic acid (eg, corn oil) is unlikely to be beneficial, as this action precedes the blocked step.13 Levels of PGE2, leukotrienes, and thromboxane are not increased in the presence of GLA. Although the exact mechanism is unclear, feedback inhibition from increased PGE1 synthesis might be responsible.9
Clinical Studies
Because GLA is an essential component of the neuronal membrane and has been shown to increase the production of PGE1, dietary supplementation with products rich in GLA (eg, evening primrose oil) has been suggested.9 ,14 Three RCTs have examined the effect of GLA in diabetic neuropathy; results from all three trials are detailed in Table 1. The first randomized, double-blind placebo-controlled study involved 22 patients with type 1 and type 2 diabetes mellitus and mild distal diabetic neuropathy for a mean of 3 years.15 Patients received 360 mg/d of GLA or an indistinguishable placebo for 6 months. Patients receiving GLA had statistically significant improvements in 6 of 6 nerve function measurements, wrist and ankle heat threshold values, and overall symptom scores. Glycohemoglobin (HbA1C) was not significantly different between treatment groups, indicating that GLA had no effect on glucose control. Side effects were similar for patients receiving evening primrose oil and placebo.
Clinical Trials of Evening Primrose Oil and Diabetic Neuropathy.
The second trial was a larger randomized, double-blind placebo-controlled study involving 111 patients with type 1 and type 2 diabetes and mild or moderate neuropathy, 84 of whom completed the study.16 Patients with severe neuropathy were excluded. Patients received either a placebo (liquid paraffin) or 480 mg/d of GLA for 1 year. At 1 year, patients who received GLA had a statistically significant increase in 13 of 16 neural function measurements compared with placebo. Sex, age, and type of diabetes had no effect on the results. Side effects were similar in both groups. Improvements were significantly greater in patients with glycohemoglobin values of less than 10%, defined as relatively well-controlled diabetes in this study, as compared with those with glycohemoglobin values of 10% or greater. Interestingly, the definition of relatively well-controlled diabetes used in this trial exceeds the current standard of HbA1C < 7% set by the American Diabetic Association (ADA).18
Results from the third trial examined vibratory perception threshold, a measurement different from those of previous trials.17 This randomized, double-blind, placebo-controlled study examined 51 patients with type 1 and type 2 diabetes and autonomic peripheral neuropathy who received 480 mg or GLA a day or placebo for 1 year. At the study endpoint, patients receiving evening primrose oil showed no improvements in vibratory perception threshold compared with placebo.
Adverse Effects, Cautions, and Drug Interactions
In clinical trials, the side effect profile for evening primrose oil was generally mild and similar to placebo. Evening primrose oil might interact with certain prescription and nonprescription medications, however. By decreasing the formation of thromboxane and increasing the formation PGE1, evening primrose oil can inhibit platelet aggregation. Patients taking antiplatelet or anticoagulant medications should use evening primrose oil cautiously or not at all. Theoretically, the effects of evening primrose oil could also be diminished by nonsteroidal anti-inflammatory medications that block prostaglandin formation. There have been case reports of seizures in patients taking evening primrose oil for schizophrenia19 and in a patient using a combination evening primrose oil, black cohosh, and chasteberry product for premenstrual symptoms.20 Product analysis, however, was not performed, so the causative agent could not be confirmed. Caution is advised for patients with preexisting seizure disorders.
Formulation and Dosage
In trials reporting positive results, a treatment duration of 6 to 12 months was generally required. Efamol, the most common formulation used, is available in the United States as 500-mg capsules. The recommended dose of evening primrose oil is 8 to 12, 500-mg capsules each day. Each capsule has 40 mg of GLA, so a dose of 360 to 480 mg of GLA requires 9 to 12 capsules. Given this large quantity of capsules, patient compliance could be a problem. Furthermore, the oil content of the recommended dose could potentially contribute to weight gain, an already undesirable effect in overweight diabetics.
Clinical Recommendation
At the present time, the body of knowledge concerning evening primrose oil and diabetic neuropathy is limited and inconclusive. Beneficial results from two clinical trials and a mild side-effect profile, however, suggest that evening primrose oil might be useful in cases of mild diabetic neuropathy. It might also be useful as an add-on therapy for patients with mild to moderate neuropathy who achieve only partial relief from prescription drug therapy. In such cases, patients need to be educated about proper dosage, potential drug interactions, and side effects.
Alpha-Lipoic Acid
History
Alpha-lipoic acid, also known as thioctic acid, is approved for clinical use in the management of diabetic neuropathy in Germany.21 Treatment with alpha-lipoic acid improves nerve blood flow and distal nerve conduction and increases endoneurial glucose uptake and energy metabolism in animals.22 ,23 Alpha-lipoic acid has also been used to reduce oxidative damage associated with mushroom poisoning, radiation, and alcoholic hepatitis.21
Pharmacology
Alpha-lipoic acid is an endogenous, sulfur-containing, free radical scavenger found in mitochondria. Free radicals can reduce nitric-oxide-mediated vasodilation and damage to the vascular endothelium.2 Alpha-lipoic acid also recycles other antioxidants, such as vitamins E and C, but can chelate with transition metals, such as iron and copper. Because it is both fat- and water-soluble, alpha-lipoic acid reduces oxidation throughout the body.21
Clinical Trials
A systematic review of 15 trials concluded that short-term treatment with parenteral alpha-lipoic acid, 600 mg/d, reduced neuropathic symptoms and deficits.24 These conclusions were primarily based on the results of four randomized, double-blind, placebo-controlled studies entitled ALADIN (Alpha Lipoic Acid in Diabetic Neuropathy), ALADIN II, ALADIN III, and ORPIL (Oral Pilot), the results of which are detailed inTable 2. Problems with sample size, study design, and the way in which neuropathic symptoms were scored made results from the previous 10 trials inconclusive. An additional trial that assessed cardiac autonomic neuropathy will not be discussed.
Clinical Trials of Alpha-Lipoic Acid (ALA) and Diabetic Neuropathy.
In the ALADIN study, 328 patients with type 2 diabetes mellitus and symptomatic peripheral neuropathy were randomly assigned to 100, 600, or 1,200 mg/d of parenteral alpha-lipoic acid or placebo.25 At 3 weeks, of the 260 patients that completed the study, those receiving the 600 and 1,200 mg/d doses of alpha-lipoic acid had statistically significant improvements in pain, paresthesias, and numbness compared with placebo. Improvements at the 1,200 mg/d dose were greater, but this group also reported more adverse effects (eg, gastrointestinal upset and headache). Glycohemoglobin levels were similar among treatment groups at 3 weeks, indicating that alpha-lipoic acid did not affect glucose control.
The ALADIN II study examined the effects of oral alpha-lipoic acid, 600 or 1,200 mg/d, in 65 patients with type 1 and type 2 diabetes and symptomatic polyneuropathy.26 At 2 years, both doses of alpha-lipoic acid showed a statistically significant increase in nerve conduction velocity compared with placebo. Severity of symptoms was not improved, however, based on the Neuropathy Disability Score. The Neuropathy Disability Score measures ankle reflexes, vibration, pinprick, and temperature sensation at the great toe and was developed to screen large populations of patients in epidemiologic studies.29 As a result, the sample size in the ALADIN II study might have been too small to detect significant changes in the Neuropathy Disability Score. Glycohemoglobin levels were similar between groups at the study endpoint.
ALADIN III examined the effects of short-term treatment with parenteral alpha-lipoic acid followed by extended treatment with oral alpha-lipoic acid.27 In this multicenter trial, 503 patients with type 2 diabetes and symptomatic peripheral neuropathy were placed in one of three treatment groups: (1) 600 mg/d parenteral alpha-lipoic acid for 3 weeks, then 1,800 mg/d of oral alpha-lipoic acid for 6 months; (2) 600 mg/d parenteral alpha-lipoic acid for 3 weeks, then an indistinguishable oral placebo for 6 months; or (3) parenteral placebo for 3 weeks, then oral placebo for 3 months. Neuropathic deficits were significantly reduced in patients receiving parenteral alpha-lipoic acid at 3 weeks. After 6 months of treatment with oral alpha-lipoic acid, a decrease in neuropathy impairment scores was observed; however, this difference was not significant. At the study endpoint, no significant differences were detected in glycohemoglobin levels or adverse side effects between the treatment groups.
Contrary to the results from ALADIN III, the ORPIL study found that oral administration of 1,800 mg/d of alpha-lipoic acid reduced neuropathic deficits and symptoms in patients with type 2 diabetes and symptomatic polyneuropathy during a 3-week period.28 The sample size in this trial, however, was substantially smaller; only 22 patients completed the trial.
Two additional studies entitled NATHAN (Neurological Assessment of Thioctic Acid in Neuropathy) I and II are currently underway.24 NATHAN I is a randomized, 4-year, double-blind, placebo-controlled investigation to examine the effect of oral alpha-lipoic acid on diabetic polyneuropathy. NATHAN II, like the ALADIN studies, examines the effect of short-term (3-week) parenteral alpha-lipoic acid. Both studies are likely to provide further insight into questions regarding formulation, treatment duration, and clinical efficacy.
Adverse Effects, Cautions, and Drug Interactions
Clinical and postmarketing surveillance studies have indicated that alpha-lipoic acid has a favorable side effect profile.24 Adverse effects are mild and include headache, skin rash, stomach upset at high doses (>600 mg/d) and possible hypoglycemia.21 ,26 Patients and physicians need to be aware that alpha-lipoic acid is a chelating agent and might cause mineral shortages in the body. As a result, iron levels should be monitored in patients taking alpha-lipoic acid. In addition, a vitamin B supplement should be taken if alpha-lipoic acid is given to patients who are thiamine-deficient (eg, alcoholics). Patients taking other medications that chelate with alpha-lipoic acid (eg, antacids) should space the dosing of these products by at least 2 hours.
Formulation and Dosing
In clinical trials, symptomatic improvements were more likely to be observed after short-term parenteral use than after long-term use of oral alpha-lipoic acid. It is not available in the United States as a parenteral formulation, but tablet strengths ranging from 30 to 100 mg are available. Some clinical trials report significant improvements in nerve conduction velocity with oral doses of 600 to 1,200 mg/d for 2 years.26 Symptom improvement was also observed using 1,800 mg/d for 3 weeks.28 The optimal dose for oral dosing is currently unknown, but a minimum treatment duration of 3 weeks is likely required.
Clinical Recommendation
As more research on the long-term benefits of alpha-lipoic acid become available, statements concerning the long-term safety and clinical effectiveness can be made. At this time, because alpha-lipoic acid has a limited side effect profile and is already approved in Germany for diabetic neuropathy, it should be considered as a treatment option for diabetic patients with mild to moderate neuropathy. In such cases, patients should be educated about the potential side effects and vitamin and mineral deficiencies associated with alpha-lipoic acid use.
Capsaicin
History
Capsaicin, an ingredient in chili pepper, has been used for centuries both orally for dyspepsia and topically as a counterirritant.30 Today, capsaicin is most often used for its analgesic properties for a variety of disorders, including osteoarthritis, postmastectomy pain, cluster headache, psoriasis, postherpectic neuralgia, and diabetic neuropathy.30 ,31 Unlike many other botanical-based products, capsaicin is regulated as an over-the-counter product by the Food and Drug Administration and therefore meets manufacturing, safety, and clinical efficacy standards for over-the-counter products.
Pharmacology
Diabetic sensory neuropathy involves both large and small sensory fibers. While large-fiber involvement is often painless, small-fiber loss can manifest as symptoms of shooting, burning, or sharp pain and aching.32 Capsaicin directly affects sensory fibers, especially C-fibers.31 The capsaicin receptor that is located only on small, slow-conducting, unmyelinated C-fibers regulates calcium flux.31 Initial application of capsaicin stimulates these fibers and depletes endogenous neurotransmitter stores associated with pain transmission, such as substance P, vasoactive intestinal peptide, cholecystokinin, and somatostatin.33 The result can be a burning sensation within the first few weeks of use. Successive application, however, results in a dose-dependent degeneration and desensitization of afferent fibers, blocking further action potential conduction.31 By maintaining afferent sensations for touch, temperature, and vibration and by blocking those for pain, patients with neuropathy who use capsaicin can continue to monitor for signs of possible foot ulceration.34
Clinical Studies
Only one trial has compared topical capsaicin to tricyclic antidepressants for diabetic neuropathy.35 This randomized, double-blind trial enrolled 250 patients with type 1 and type 2 diabetes mellitus and painful chronic neuropathy. Patients received topical capsaicin 0.075% four times a day and oral placebo or topical placebo and oral amitriptyline titrated up from 25 mg/d to a maximum of 125 mg/d (mean dose not stated). Methyl nicotinate was used as the topical placebo for the first 2 weeks to simulate the burning associated with capsaicin. After 8 weeks, equivalent, statistically significant improvements in pain severity, pain relief, and activities of daily living were observed in both groups compared with baseline. The differences were not significantly different between groups, indicating an equivalent clinical response. Systemic adverse effects were significantly more frequent in patients receiving amitriptyline (eg, sedation, anticholinergic effects), while topical skin reactions were significantly more frequent in patients receiving capsaicin. The latter might have compromised blinding. In addition, given the lack of a topical and oral placebo arm, the magnitude of a placebo response is unknown.
Other randomized, double-blind trials have compared topical capsaicin 0.075% with topical placebo for 4 to 12 weeks in patients with diabetic neuropathy.32 ,36–39 These trials are described in detail in Table 3. All trials assessed pain based on three scales: the Physician’s Global Evaluation scale (PGE), which rates patient’s pain as completely gone (+3), much better (+2), better (+1), no change (0), worse (−1), or much worse (−2), a 100-mm visual analog scale for severity (VAS-P), and a similar scale for relief (VAS-R). Four trials enrolled 22 to 277 patients with types 1 and 2 diabetes and moderate to severe neuropathy.32 ,36–38 Two reported significant improvements in all three outcome measures at 8 weeks,32 ,37 whereas two reported significant improvements in only one outcome measure at 4 to 8 weeks.36 ,38
Clinical Trials of Capsaicin and Diabetic Neuropathy.
In most trials, patients were more likely to experience burning after application with capsaicin (60% to 63%) compared with placebo (17% to 20%), which could have affected blinding. The largest trial also had a significantly higher dropout rate for patients using capsaicin.37 When the results of this trial were analyzed again using an intention-to-treat analysis, all three outcome measures became insignificant. Meta-analysis of these four trials, however, still showed a significant benefit for capsaicin compared with placebo, with an odds ratio of 2.74 (95% confidence interval 1.73–4.32).30 In a fifth trial, 40 patients with moderate distal neuropathy, of which 7 (12%) had diabetes, experienced no improvement in any outcome measure at 12 weeks.39 This trial also used a methyl nicotinate placebo to simulate the initial burning sensation from capsaicin.
Adverse Effects, Cautions, and Drug Interactions
Capsaicin is commonly associated with a burning sensation at the site of application that lasts 2 to 14 days. This sensation might affect patient compliance, and patients should be advised to continue use, if the pain is tolerable, because up to 4 to 6 weeks can pass before benefits are appreciated. Application with gloves is recommended to avoid contact with the eyes and other mucous membranes. Patients with open wounds or broken skin should avoid contact with capsaicin in these areas. There are no drug-drug interactions reported for capsaicin.
Formulation and Dosing
Capsaicin is available without a prescription in two strengths, 0.025% and 0.075%, but the higher strength has typically been used for diabetic neuropathy. It is important that both patients and health care providers know that capsaicin used on a daily, twice daily, or as-needed basis is likely ineffective. Clinical trials show that application must take place three to four times a day for improvement.
Clinical Recommendation
The clinical usefulness of capsaicin is not conclusive. It could be effective as monotherapy in cases of mild to moderate diabetic neuropathy. It might also be useful as an adjunctive agent in combination with prescription drug therapy. The appropriate dosing of capsaicin is essential for symptomatic improvement. Unfortunately, many patients and providers often prescribe this product at too low dosages.
Other Dietary Supplements
A number of other dietary supplements have been promoted as treatments for diabetic neuropathy. These supplements include acetyl-𝓁-carnitine, pyridoxine (vitamin B6), vitamin E, and St. John’s wort. In general, these products have been less well researched or have reported negative findings for diabetic neuropathy.
Acetyl-𝓁-carnitine
Acetyl-𝓁-carnitine, an endogenous substance similar in structure to acetylcholine, is involved in the uptake and oxidation of long-chain fatty acids in mitochondria.40 Low levels of acetyl-𝓁-carnitine have been found in the sciatic nerve of diabetic rats, and acetyl-𝓁-carnitine supplementation has been shown to improve nerve function.41–43 In humans, two studies have examined the effect of acetyl-𝓁-carnitine on diabetic neuropathy. The first RCT examined 20 patients with symptomatic neuropathy for a 15-day period.40 Patients received either intramuscular acetyl-𝓁-carnitine or placebo at 1,000 mg/d. At the end of the study, patients receiving acetyl-𝓁-carnitine showed a significant decrease in neuropathic symptoms compared with placebo, but no change in vibratory perception threshold.
The second study was a much larger randomized, double-blind, placebo-controlled study that examined the effect of acetyl-𝓁-carnitine administration on neuropathic symptoms and first foot ulceration.44 In this study, 1,035 patients with type 1 and 2 diabetes and peripheral neuropathy received 1,000 mg/d of oral acetyl-𝓁-carnitine or placebo for 1 year. At the study endpoint, there were no significant differences in neurological parameters (vibratory perception threshold, muscle strength, reflexes, 10-g monofilament scores) or rate of first foot ulceration between treatment groups.
Vitamin B6
Low levels of vitamin B6 have been reported in patients with diabetic neuropathy but not in diabetic patients without neuropathy.45 Deficiencies of vitamin B6 have also been linked to peripheral neuropathy in persons consuming isoniazid.46 As such, a number of studies have evaluated the effectiveness of vitamin B6 in diabetic neuropathy. One small-scale, 6-week trial, with an open-study design evaluated the effect of 25 mg of oral vitamin B6 in 10 diabetic patients.47 Although this trial observed symptomatic improvement in all patients, three subsequent randomized, double-blind placebo-controlled studies found no benefit.48–50
Vitamin E
The effect of vitamin E on nerve function parameters was evaluated in a randomized, double-blind, placebo-controlled trial involving 21 patients with type 2 diabetes and mild-to-moderate neuropathy.51 Patients received 900 IU of vitamin E or placebo for 6 months. Although there were no changes in glycemic indices, both median and tibial motor nerve conduction velocity were significantly improved in the vitamin E group compared with placebo.
St John’s Wort
St. John’s wort has been proposed as an analgesic for painful diabetic neuropathy. Similar to the tricyclic antidepressants that are used in the management of neuropathy, St. John’s wort might also have antidepressant qualities. One study examined the effect of St. John’s wort on pain in patients with diabetic and nondiabetic neuropathy.52 In this double-blind study, 47 patients, 18 diabetic and 29 nondiabetic, randomly received 900 mg/d of oral St. John’s wort or placebo for 5 weeks. They then crossed over to the other therapy for an additional 5 weeks. At the study endpoint, diabetic patients who received St. John’s wort had a statistically significant reduction in lancinating (shooting) pain compared with placebo. There were no changes, however, in other measures of total pain score, constant pain, touch-evoked pain, or pain on pressure as compared with placebo.
Clinical Recommendation
Because of the lack of research on the effectiveness of acetyl-𝓁-carnitine, vitamin B6, vitamin E, and St. John’s wort for the treatment of diabetic neuropathy, these supplements cannot be recommended at this time. Health care providers should direct patients toward those therapies that have been better researched or have shown positive outcomes in clinical trials.
Conclusion
Although adequate glucose control is a mainstay of treatment for diabetic neuropathy, other treatments may be used by patients if symptom relief is not adequate. The accessibility of botanical and dietary supplement products, as well as direct-to-consumer advertising, makes these choices attractive for many patients. All the botanicals and dietary supplements discussed in this review, with the exception of capsaicin, have shortcomings as a result of their regulation by the Dietary Supplement Health and Education Act. Specifically, there is no guarantee of efficacy, safety, or product content. Evening primrose oil, alpha-lipoic acid, and capsaicin have received the greatest attention for their use in diabetic neuropathy, but further studies are needed to confirm their efficacy.
- Received for publication May 22, 2002.
- Revision received May 22, 2002.




{kind=link}