
Abstract
Introduction: Many primary care clinics screen patients for their unmet social needs, such as food insecurity and housing instability, and refer them to community-based organizations (CBOs). However, the ability for patients to have their needs met is difficult to evaluate and address. This study explores patient-reported barriers to accessing referred resources using a conceptual framework that identifies opportunities for intervening to optimize success.
Methods: Patients who participated in a social needs screening and referral intervention at a Federally Qualified Health Center (FQHC) were called 2 weeks after the clinic encounter. We conducted a directed content analysis across 6 domains of access to examine responses from patients who reported barriers.
Results: Of the 462 patients that were reached for follow-up, 366 patients reported 537 total barriers. The most frequent challenges related to resource availability (24.6%, eg, patients waiting for submitted application to process) and approachability (23.8%, eg, patients lacking information needed to contact or access resources). Barriers in the domains of acceptability (21.6%, eg, competing life priorities such as medical issues, major life events, or caretaking responsibilities) and appropriateness (17.9%, eg, resource no longer needed) largely represented patient constraints expressed only after the clinical encounter. It was less common for patients to identify accommodation (eg, physical limitations, language barriers, transportation barriers, administrative complexity) or affordability of community resources as barriers (11.2% and 0.9%, respectively).
Conclusion: Findings suggest opportunities for improvement across the access continuum, from initial referrals from primary care staff during the clinical encounter to patients' attempts to accessing services in the community. Future efforts should consider increased collaboration between health and social service organizations, and advocacy for structural changes that mitigate system-level barriers related to resource availability and administrative complexity.
- Communication Barriers
- Community Health Centers
- Follow-Up Studies
- Food Insecurity
- Health Services Accessibility
- Housing Instability
- Patient Navigation
- Patient Reported Outcome Measures
- Population Health
- Referral and Consultation
- Social Determinants of Health
- Social Problems
Introduction
Compelling research has demonstrated the strong link between adverse social determinants of health and poor health outcomes.1⇓⇓–4 This large body of evidence, coupled with recent value-based payment reforms, has resulted in growing interest to address individual-level, social needs in health care settings.5,6 Multiple medical professional associations across specialties, including the National Academies of Sciences, Engineering and Medicine, have recommended screening for social needs as part of routine clinical care.7⇓⇓–10 A cross-sectional survey found that 15% of primary care clinics and 30% of Federally Qualified Health Centers (FQHCs) nationwide assess patients for multiple social needs, including food insecurity, housing instability, utility needs, transportation needs, and interpersonal violence.11 To respond to identified needs, many practices have also implemented interventions to connect patients with community-based organizations (CBOs) or government programs.12⇓⇓–15 Unfortunately, primary care clinics are often limited in their capacity to continue follow-up with patients to ensure needs are met, and patients are likely to experience barriers with receiving services once referred.14,16 This study aims to examine patient-reported barriers to accessing resources for social needs, and explore differences in barriers before and during the COVID-19 pandemic.
Methods
Program Description and Data Collection
From March 2019 to December 2020, clinic case managers at a Federally Qualified Health Center (FQHC) in North Carolina screened 1682 patients for unmet social needs using the Protocol for Responding to and Assessing Patients' Assets Risks and Experiences (PRAPARE) tool as part of routine clinical care. Example domains from the PRAPARE tool include food, utilities, transportation, housing, employment, stress, social isolation, and domestic violence.17 Among patients who screened positive for an unmet need, 756 requested to receive resource referrals from case managers. Referrals ranged from clinic-based resources (eg, transportation van), CBOs (eg, food pantries), and government programs (eg, public housing). For patients given resource referrals, case managers offered additional telephonic follow-up support from trained student volunteer community resource navigators.
Navigators attempted to reach 646 patients who agreed to follow-up support within 2 weeks of the clinical encounter when the initial referral(s) were made. Navigators were trained to remind patients about their referrals and motivate follow-through, provide specific information about accessing resources (eg, application process, resource location, hours of operation), and reconnect patients with case managers when needed per our escalation protocol. When patients reported not connecting to 1 or more resource referrals, navigators asked, “Were there any reasons you were not able to connect with [the resource(s)]”? Navigators summarized and documented responses from patients as free text notes in a secure, REDCAP electronic database.18 Program details, including the screening instrument, workflows, and navigator training, are described in detail elsewhere.19⇓⇓–22
On March 10, 2020, North Carolina declared a state of emergency for the COVID-19 pandemic. Due to pandemic safety precautions, between March 2020 and December 2020, case managers shifted from screening patients for social needs in-person to conducting proactive telephonic screening for the lowest income patients, identified through reports from the clinic's finance department. Navigators continued to follow-up with patients telephonically. During the pandemic, many CBOs closed due to stay-at-home orders or reduced capacity due to increased demand for services or inadequate staffing. New social services also emerged to meet community needs during the pandemic (eg, COVID-19 emergency financial assistance, drive-through meals at schools and food delivery programs).
Qualitative Analysis
We conducted a directed qualitative content analysis on responses from patients who reported barriers during follow-up. Codes were based on the 6 dimensions of access (approachability, acceptability, availability, accommodation, affordability, and appropriateness) adapted from Levesque et al.'s conceptual framework,23 and subcodes were refined from the data itself (codebook with definitions in Appendix Table 1). Levesque et al.'s framework is widely-used in public and population health and can be used to operationalize determinants to access throughout the full process of obtaining health and social services. While the original framework includes both service-level (supply-side) and patient-level dimensions (demand-side) dimensions, we focused on conceptualizing barriers at the service-level. Such an approach allows researchers and practioners to identify concrete improvement opportunities for health and social services across the access continuum rather than blaming or attributing barriers to patients themselves.
Two researchers (SS and LS) independently coded responses in Microsoft Excel; a third researcher (TL) reconciled discrepencies. We used Stata (Release 16; StataCorp LLC, College Station, TX) to calculate the frequency of patient-reported reasons by access dimension and compared frequencies before and after the state of emergency declaration in North Carolina (March 10, 2020) using Fisher's exact test. This project received exempt approval from the Duke Health Institutional Review Board.
Results
Of the 462 patients that were reached for follow-up, 366 patients reported a barrier to connecting to a referred resource and were included in our analysis (Figure 1). Patients who reported barriers were middle age, 41.2% Hispanic (37.7% Spanish as primary language), 48.9% Black non-Hispanic, 70.4% unemployed, and 71.8% uninsured (Table 1). Patient demographics of our sample largely mirrored the broader population served by the FQHC as reported in 2020 to the Health Resource and Services Administration (eg, 92% minority, 75% female).24 Only 19.8% had started services with a resource within 2 weeks of the referral. Figure 2 displays the distribution of 537 barriers to accessing referred resources. The access dimensions availability (24.6%), approachability (23.8%), and acceptability (21.6%) represented the greatest number of barriers. Availability barriers included resources being unresponsive to contact attempts from patients (8.2%), and patients waiting for submitted application to process (9.1%). Approachability barriers presented when patients lacked information needed to contact or access resources (19.0%), or forgot about resources or scheduled appointments (4.8%). Acceptability barriers included competing priorities for patients (eg, medical priorities, life disruptions from hospitalization or death in the family, caretaking or childcare responsibilities) (14.2%), and patient distrust or prior negative experiences with resources (2.8%).
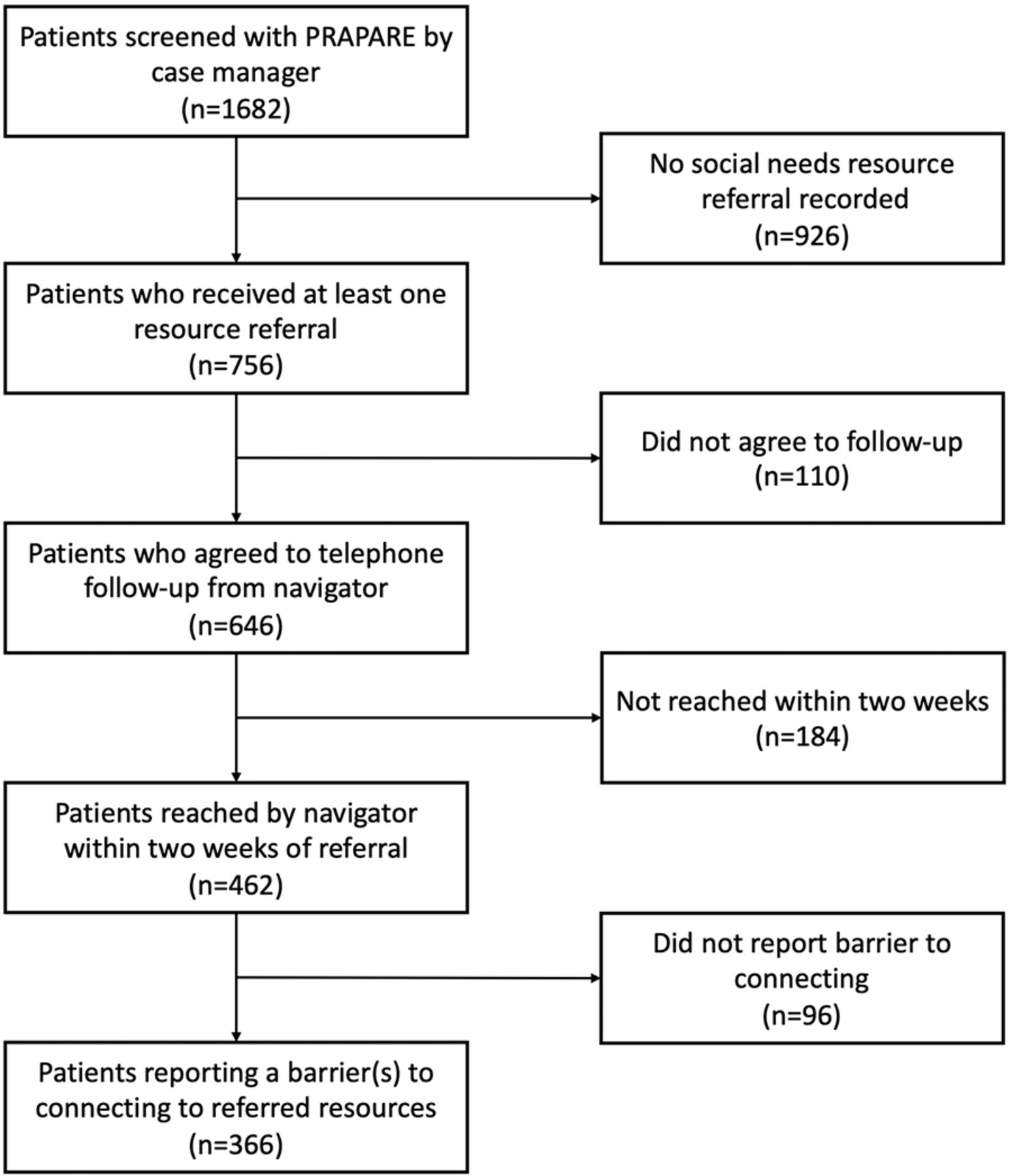
Flow diagram of patients included in qualitative analysis. Abbreviation: PRAPARE, Responding to and Assessing Patients' Assets Risks and Experiences.

Distribution of 537 patient-reported reasons for not accessing referred resources according to Levesque et al.'s conceptual framework for health care accessa,b.
Characteristics of Patients Who Reported Barriers to Access (n = 366)
Compared with before the pandemic, patients screened after March 2020 more frequently reported barriers related to resources' capacity (eg, not able to take new clients or closed altogether) (P = .004), COVID-19 related concerns (P = .049), and language access (P = .043); it was less common to report competing family or health priorities as a barrier than before the pandemic (P < .001) (Appendix Table 2).
Discussion
This study is among the first to explore barriers that primary care patients face when accessing referred resources for social needs. Patients in this study were racially and ethnically diverse, mostly uninsured, and reported high levels of social risk (eg, housing instability, food insecurity, and poor access to medicine and health care). Our findings represented all service-level dimensions of access from Levesque's conceptual framework23, and the most frequent barriers were related to resources' approachability, acceptability, and availability. Mapping strategies to these barriers can guide opportunities to intervene during the clinical encounter, between clinic providers and CBOs, and for services directly supporting patients in the community to ultimately address unmet needs and support better health.
Nearly a fifth of reported barriers related to lacking information about resources, which calls attention to how referrals are presented to patients. This type of barrier to approachability may be prevented through better-designed, literacy-sensitive resource handouts, and information provided via multiple mediums (ie, article, e-mail, text), depending on patient preferences. A recent trial comparing the effect of 2 social risk interventions on the number of self-reported social risk factors and child and caregiver health suggested that high-quality, up-to-date written handouts, that specify contact names for services and highlight most relevant resources, could increase effectiveness.25 Given that patient educational materials often do not reflect national guidelines for readability and suitability,26 communication and education specialists could provide useful expertise for designing and testing strategies to address this critical gap.
Clinic staff must also consider how to increase referral appropriateness. Nearly a fifth of barriers related to patients no longer needing or being interested in a resource, indicating inadequate relevance of referrals to patients, or poor timeliness of the resources to provide assistance. Since the PRAPARE screening tool asks broadly about social needs over the past year, incorporating additional questions related to urgency, priority, and desire for assistance may result in more patient-centered referrals. More immediate follow-up and reminders, such as text messages or calls from staff and volunteers, can nudge patients to access resources closer to the clinic encounter. While our study focused on examining barriers for patients who accepted referrals, future research should also examine why many patients who screen positive for social risks are not interested in receiving assistance.27
Overcoming barriers related to resource availability, acceptability, and accommodation may require collaborative action across sectors to address delays, complexities, distrust, and physical barriers. Existing models of collaboration between health and social services organizations are likely inadequate to fully address patients' social needs. Solutions may include colocation, standardized referral processes, and community navigators.7 North Carolina is implementing a statewide technology platform that facilitates closed-loop referrals across health and social services.28 The platform can also help identify resources that meet patients' accommodation needs, such as language preferences or physical limitations. Evaluation of this technology is still needed to assess its utility and effectiveness. These and other strategies need further investment as the COVID-19 pandemic has highlighted critical gaps in the social safety net, digital equity, and trust in communities.21
In addition to strengthening collaborations with CBOs to better support individual patients, health care providers should also consider how they can partner with CBOs to advocate for upstream policy changes at the system level. For example, health providers can advocate for policies to increase investment in social care resources, or advocate for reduced administrative burden of applications to social services.29,30 This is consistent with the implications found in a recent retrospective cohort study conducted at the same FQHC that found that a simplified, ‘direct-access’, and less complicated process for applying and receiving services was associated with a statistically significant increase in the odds of successfully connecting with a referred resource.22 Additional qualitative research conducted with patients participating in the same social needs intervention at our FQHC also revealed that policy and societal level determinants related to resource availability and application processes were major barriers to referral success.29
This study has several limitations. First, while we reached 72% of patients referred to follow-up by phone, it is possible that the distribution of barriers may change when accounting for patients not reached, particularly as patients reached were more likely to be referred to resources for food, financial assistance, and medicine and health care. Second, although our patient sample is large and diverse, this study is limited by the type of data we analyzed, obtained as written notes from navigators rather than verbatim responses recorded directly from patients. While we already conducted semistructured interviews to elicit more in-depth responses29, future efforts may consider using structured surveys using our adapted framework to capture more quantitative data to test our qualitative findings and improve generalizability. Third, given our sample is limited to 1 FQHC in a midsized city, translation of our findings should be considered carefully by clinical and community contexts. Larger studies are needed to study patient barriers across more diverse primary care contexts, including non-FQHC practices serving low-income populations and clinics in rural areas.
Our findings reveal the breadth of patient-reported barriers to connecting with referred resources for unmet social needs across the access continuum. Challenges begin with how primary care staff present referrals to patients during the clinical encounter, continue when patients attempt to access services in the community, and are further compounded by patients' individual contexts and previous experiences with social services. Our findings are consistent with previous reports describing intersecting systemic and personal barriers to accessing social services.31⇓–33 While previous efforts have focused on social risk screening34,35, continued innovation and investment are needed at each stage of the downstream process of assisting patients with their social needs to overcome patient barriers and optimize social care interventions.
Appendix
Codebook for Patient-Reported Reasons for Not Connecting to a Referred Resource
Frequency of Patient-Reported Reasons for Not Accessing Referred Resource Before and During COVID-19 Pandemic
On March 10, 2020, the state of North Carolina declared a state of emergency for the COVID-19 pandemic. The “COVID-19” subsample of patients are all those who were screened on or after March 10, 2020
The association between the prevalence of a barrier and the patient's screening date (before or after the onset of the COVID-19 pandemic) were assessed using Fisher's exact test.
Notes
This article was externally peer reviewed.
Funding: Funding was provided by the Duke University Bass Connections Program (Durham, NC).
Conflicts of interest: The authors have no relevant financial or nonfinancial interests to disclose.
To see this article online, please go to: http://jabfm.org/content/35/4/791.full.
- Received for publication November 18, 2021.
- Revision received January 28, 2022.
- Revision received March 19, 2022.
- Accepted for publication March 25, 2022.




{kind=link}
{kind=link}