
Abstract
Purpose: Examine use of office resources by primary care patients who were initially evaluated through telehealth, telephone, or in-person encounters.
Methods: Retrospective electronic health record review on patients seen in March 2020 for evaluation of potential COVID-19 symptoms, to assess the total number of interactions with physicians and office staff.
Results: Of 202 patients, 89 (44%) had initial telehealth, 55 (27%) telephone, and 52 (26%) in-person encounters. Patients initially evaluated through telehealth, telephone, and in-person encounters had a mean of 6.1 (S.D. = 3.7), 5.2 (S.D. = 3.6), and 4.5 (S.D. = 3.0) total interactions with the office, respectively (P = .03), and 9%, 12.7%, and 19.2%, respectively, had a subsequent in-person or emergency department visit (P = .22). Multivariable analysis showed no differences in number of office interactions based on initial visit type; older patients (95% CI = 0.00-0.07) and those with subjective fevers (95% CI = 1.01–3.01) or shortness of breath (95% CI = 0.23-2.28) had more interactions with the office.
Conclusion: Primary care providers used virtual visits to care for most patients presenting with potential COVID-19 symptoms, with many patients choosing telephone over telehealth visits. Virtual visits can successfully limit patient exposure to other people, and consideration could be given to increasing its use for patients with potential symptoms of COVID-19.
- California, Cough
- COVID-19
- Dyspnea
- Family Medicnie
- Fever
- Primary Health Care
- Retrospective Studies
- Telemedicine
Background
The Centers for Disease Control has recommended limiting face-to-face contact with others “social distancing” to prevent the spread of coronavirus disease 2019 (COVID-19).1 Outpatient virtual visits allow patients with potential infectious symptoms to remain at home, thus reducing contact with health care providers and other patients. Virtual visits include face-to-face telehealth (video) visits, telephone visits, and online messaging (such as through a patient portal).2 Many health systems offered telehealth visits before the emergence of COVID-19,3 but the use of virtual visits by patients with COVID-19 symptoms is not represented in the literature. Knowledge on how these patients engage with health care practices is important for understanding the safety and feasibility of caring virtually for patients with COVID-19 symptoms. The objective of this study was to examine use of telehealth, telephone, and in-person encounters by primary care patients presenting with acute infectious symptoms.
Methods
Data Collection and Analysis
A retrospective electronic health record (EHR) review was performed to examine records of patients presenting to a community-based academic family medicine practice between March 3 and 31, 2020, with symptoms associated with COVID-19. This practice cares for a racially/ethnically diverse population of patients with insurance plans that include private indemnity insurance and government plans (ie, Medicaid and Medicare). Patients were identified in 2 ways: (1) staff kept detailed lists of patients whom they screened for fever, cough, or shortness of breath; and (2) 2 reviewers assessed scheduling notes describing the reason for a patient’s visit to identify those with other potential COVID-19 symptoms (ie, sore throat, nasal congestion, headache, fatigue, myalgias, nausea, vomiting, diarrhea, loss of taste or smell).4 Data abstractions were performed through April 20, 2020, to assess patient follow-up encounters.
Patients were characterized by demographics; health; type of initial visit (telehealth, telephone, in person); subsequent in-person encounter, emergency department visit, or hospitalization; symptoms reported; and outpatient testing and treatment. The “initial visit” is defined as the first encounter with a physician, whether by telehealth, telephone, or in person. The total number of patient interactions with the office regarding patient presenting symptoms was quantified. These represented the entirety of patients’ subsequent primary care interactions. Interactions included electronic messages, telephone calls, and physician telehealth, telephone, or in-person encounters. Telephone calls and electronic messages included both physician and staff interactions and included exchanges about accessing and using telehealth visits. Communication with staff before the initial visit with the physician was not used for classification of the initial visit type but contributed to the total number of interactions with the practice. The University of California, Los Angeles (UCLA) Institutional Review Board deemed this study exempt from review.
Stata 16.1 (StataCorp) was used for analyses. Chi-squared statistics and analysis of variance were used to assess differences (in patient characteristics, number of interactions with the office, outpatient testing, and medications prescribed) among patients receiving telehealth, telephone, and in-person visits.
Practice Change during Data Collection Period
In response to reports of local COVID-19 infections, the practice implemented a process on March 3, 2020, to convert selected scheduled office visits to either telehealth or telephone encounters. Staff phoned patients before scheduled office visits and administered a brief screening instrument to assess the presence of fever, cough, or shortness of breath. Patients exhibiting one or more symptoms were encouraged to have a telehealth or telephone visit with a provider, but those who desired kept their in-person visits. From March 23 through March 31, after a mandatory stay-at-home order went into effect, the office converted almost all visits to telehealth or telephone encounters. A physician had to approve in-person visits. Patients were given the choice of a telehealth versus a telephone encounter. Telehealth visits required downloading of a smartphone application to access a patient portal for the visit. If needed, staff assisted patients with these procedures. Virtual visits increased from 0.85% of total visits in February 2020 to 23.3% of visits in March 2020.
Results
Health Care System Interactions by Type of Initial Physician Visit
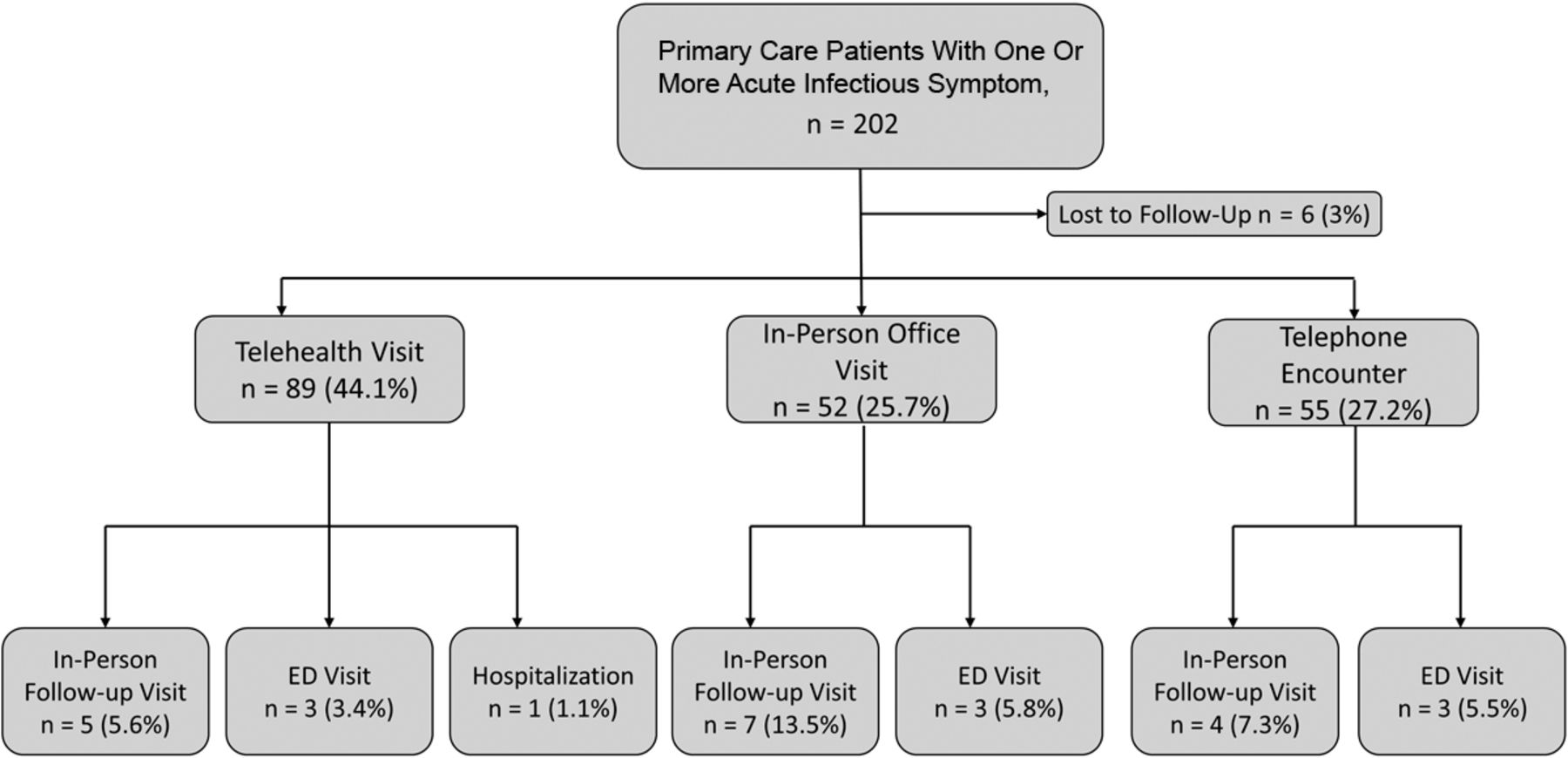
Of 202 patients presenting with at least 1 potential COVID-19 symptom assessed for study inclusion, 89 (44%) initially saw a physician by telehealth, 55 (27%) by telephone, and 52 (26%) in person. Six patients with scheduled appointments were lost to follow-up. Of patients whose first physician encounter was by telehealth, telephone, or in person, 9%, 12.7%, and 19.2%, respectively (P = .22), had subsequent in-person or emergency department visits. All 5 patients in the study who tested positive for COVID-19 were initially seen via telehealth. Only 1 required a subsequent in-person visit and hospitalization (Figure 1).
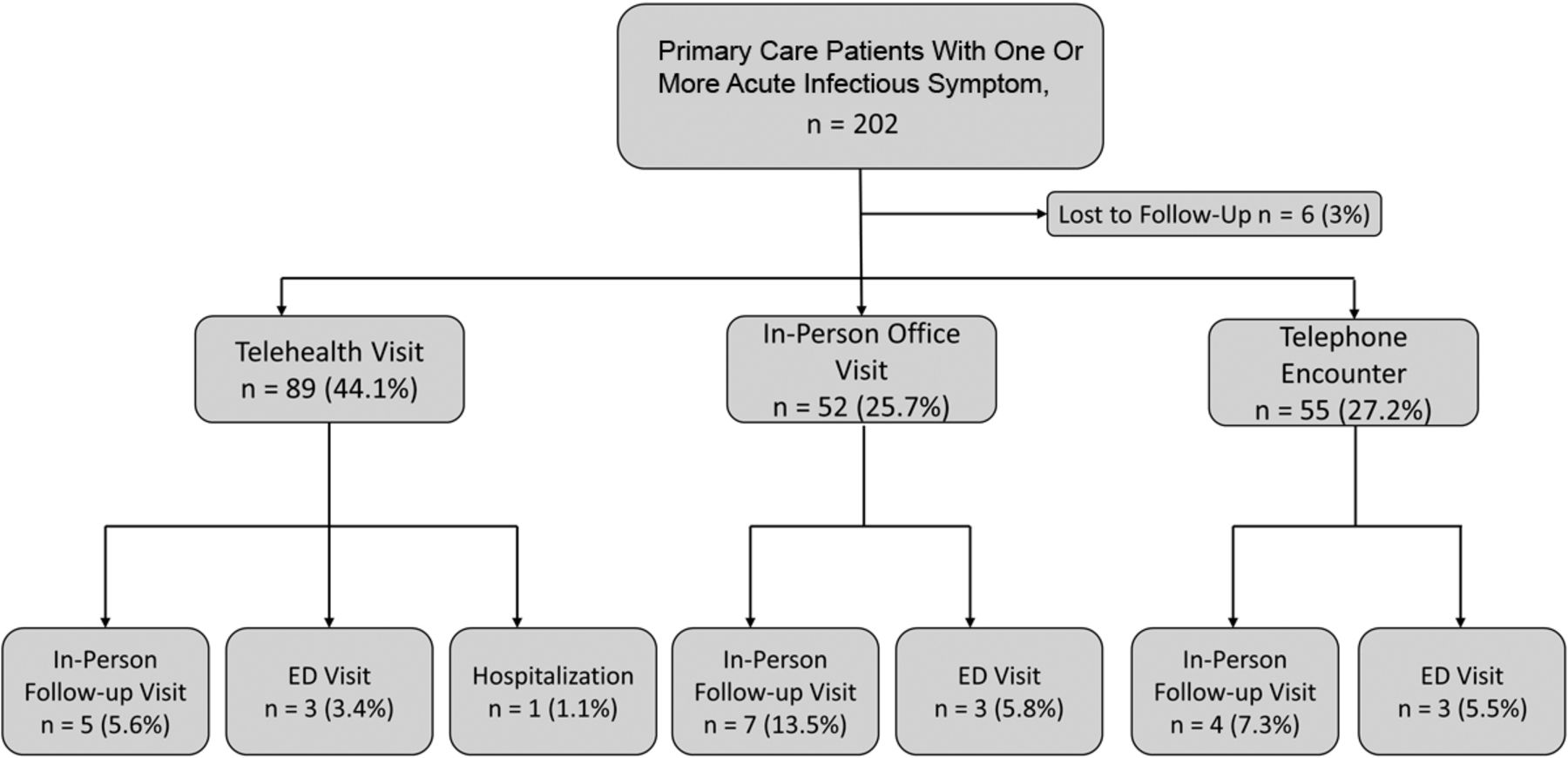
Distribution of initial and follow-up visits. Abbreviations: ED, emergency department.
Patient Characteristics by Type of Initial Physician Visit
Table 1 depicts differences in characteristics of patients who were initially evaluated by their physician via telehealth, telephone, or in person. Patients with initial in-person visits tended to be younger than those with telephone and telehealth encounters (38.5% of those initially seen in person were aged 18 and younger, compared with 18.2% and 6.7% of those with initial telephone or telehealth encounters). Of patients aged 18 and younger, 14 (70%) of those with initial in-person visits and 29 of 38 (76.3%) overall had Medicaid insurance.
Patient Characteristics, Overall and by Visit Type
Patient-Reported Symptoms
Patients most commonly presented with cough (78%), fever (39%), and shortness of breath (38%). Those reporting shortness of breath were more likely to have virtual visits than in-person visits (48.3% telehealth and 36.4% telephone vs 21.2% in-person encounters; P < .01).
Discussion
Primary care physicians in this study successfully cared for the majority of patients seen virtually for potential COVID-19 symptoms. Most patients who were initially cared for through a virtual visit did not require subsequent in-person office visits or emergency department visits to address their symptoms, even though they were more likely to experience concerning symptoms such as shortness of breath. On average, these patients used more office staff and physician resources compared with in-person visits, though they were more likely to report shortness of breath than those initially seen in person. Therefore, physicians could have asked patients to follow up more closely, as their inability to perform a physical examination may have led to more uncertainty about their assessment. Alternatively, patients could have scheduled follow-up appointments on their own if they developed shortness of breath after initial evaluation. Correspondence with office staff regarding the access and use of telehealth also likely made up many of the virtual interactions.
Given the choice, most patients in this study chose to have telephone over telehealth encounters. Future studies are needed to investigate reasons underlying this preference, which we hypothesize may include difficulty with or lack of the technology required for telehealth visits or health insurance policies requiring patient cost sharing for telehealth but not for telephone visits.
Younger patients, driven largely by those aged 18 and younger, were more likely to have in-person office visits than older patients. This finding may reflect greater parental desire to have children examined in person, because children may be unable to provide an adequate history of their symptoms. However, because the majority of our practice’s children have Medicaid insurance, these findings may reflect barriers related to socioeconomic status or social determinants of health and require future investigation.
Study limitations include underestimation of the total number of telephone calls and messages exchanged with patients, because each telephone and message encounter in our EHR system may represent multiple back-and-forth exchanges. We did not assess whether telephone calls and messages after the first visit were with physicians or office staff. Though we collected data for at least 20 days after initial patient presentations, some patients may have had ongoing illness when data collection ceased. Limited COVID-19 testing capacity existed for the majority of the data collection period.
COVID-19 has rapidly transformed physician health care delivery by increasing the use of virtual medicine in an attempt to limit patient and health care provider exposure to COVID-19 and decrease the burden on emergency departments. This increased use of virtual visits may persist beyond the current pandemic period as patients embrace the safety and flexibility that this mode of medicine offers compared with in-person office visits.5 However, as these visits require greater coordination and use of practice resources than traditional in-person office visits, future work is needed to examine the costs and financial repercussions for medical practices that incorporate virtual visits. Primary care practices implementing virtual visits to care for patients with COVID-19 symptoms should be prepared for increased patient interactions with the practice, many of which may unreimbursed.
Acknowledgments
The authors appreciate the assistance of Jessica R. Zarndt, DO, and Luis Molina Rojas, MD, for their help with data collection, and of David Bholat, PhD, for his feedback on the manuscript.
Notes
This article was externally peer reviewed.
Funding: None.
Conflicts of interest: The authors report no conflicts of interest.
To see this article online, please go to: http://jabfm.org/content/34/Supplement/S147.full.
- Received for publication May 20, 2020.
- Revision received July 6, 2020.
- Accepted for publication July 6, 2020.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Points of Concordance, Points of Discordance: A Qualitative Examination of Telemedicine Implementation
- Association of Telehealth with Short-Interval Follow-Up
- Understanding how the design and implementation of Online Consultations influence primary care outcomes: Systematic review of evidence with recommendations for designers, providers, and researchers
- Primary Care in the COVID-19 Pandemic: Essential, and Inspiring