
Abstract
Background: Because of the Coronavirus disease 2019 (COVID 19) pandemic, many primary care practices have transitioned to telehealth visits to keep patients at home and decrease the transmission of the disease. Yet, little is known about the nationwide capacity for delivering primary care services via telehealth.
Methods: Using the 2016 National Ambulatory Medical Survey we estimated the number and proportion of reported visits and services that could be provided via telehealth. We also performed cross-tabulations to calculate the number and proportion of physicians providing telephone visits and e-mail/internet encounters.
Results: Of the total visits (nearly 400 million) to primary care physicians, 42% were amenable to telehealth and 73% of the total services rendered could be delivered through telehealth modalities. Of the primary care physicians, 44% provided telephone consults and 19% provided e-consults.
Discussion: This study underscores how and where primary care services could be delivered. It provides the first estimates of the capacity of primary care to provide telehealth services for COVID-19 related illness, and for several other acute and chronic medical conditions. It also highlights the fact that, as of 2016, most outpatient telehealth visits were done via telephone.
Conclusions: This study provides an estimate of the primary care capacity to deliver telehealth and can guide practices and payers as care delivery models change in a post-COVID 19 environment.
- Child Health
- COVID-19
- Family Medicine
- Mental Health
- Pandemics
- Primary Care Physicians
- Primary Health Care
- Rural Health
- Social Determinants of Health
- Telemedicine
Background
The Coronavirus disease 2019 (COVID 19) pandemic has rapidly and dramatically changed the delivery of primary care in the short term, shifting many visits from traditional face-to-face encounters to telehealth only encounters. This shift has many clinicians, payers and policy makers questioning the feasibility of telehealth long-term. Despite limited incorporation before March 2020, a number of essential primary care services may be delivered by the spectrum of telehealth modalities.1 For instance, many studies indicate the feasibility of using telehealth modalities to provide examinations and screenings, mental and behavioral health counseling, health education, and preventive care.2⇓⇓⇓–6 Other studies suggest some primary care services may be effectively provided via telehealth.7⇓⇓–10 A limited number of studies indicate telehealth may be comparatively effective vs traditional face-to-face care and may also save money.11⇓⇓⇓⇓⇓–17
The slow uptake of telehealth before the COVID-19 pandemic had many causes, from poor reimbursement to lack of infrastructure to burdensome rules and regulations to patient and provider preferences. The need to slow the spread of COVID-19 and keep patients at home has resulted in rapid changes in care delivery followed by significant changes in payment and regulation that have supported a rapid transition to telehealth.18
Despite current transitions to telehealth-based practice and evidence that many primary care services may be effectively delivered via telehealth, little is known about the nationwide capacity for delivering primary care services via telehealth. The purpose of this study was to analyze the primary care capacity to deliver services and clinical care through telehealth mechanisms. We explored this topic using the National Ambulatory Medical Survey 2016 (NAMCS) data.
We used 2 approaches to explore telehealth: (1) a broader definition of telehealth visit that includes patient-physician encounters that are telephone or internet/e-mail consults, and (2) a visit where provision of at least 1 service requires physical presence of a physician was defined as not amenable to telehealth. All those visits that did not require physical presence of a physician were termed as amenable to telehealth.
Study Data and Methods
Data Sources
NAMCS is an annual survey administered by the Division of Health Statistics, National Center for Health Statistics. Data are collected using a national multistage probability sample of visits to non-federally employed physicians. The sampling frame for the NAMCS 2016 was derived from databases maintained by the American Medical Association (AMA) or the American Osteopathic Association (AOA) though membership in these organizations is not required for listing. The patient-physician encounter in an office-based setting is the primary sampling unit. Each physician is assigned a 1-week reporting period; the physician reports data on all the ambulatory care visits that may have occurred during that period. We used the 2016 NAMCS data to explore the telehealth capacity of primary care physicians. The response rate was 39.3% for physicians who provided data for at least 1 encounter.
The main data collection includes computer-assisted automated tools accessible through the Web portal or a laptop computer provided by the data collection staff. Two forms, the Patient Record Form and the Physician Induction Interview Form, are used to record the data. The Physician Induction Interview Form is used to collect information about the characteristics of the physician practices. The Patient Record Forms are used to measure data on socio-demographic characteristics, expected source of payment, the reason for visit, diagnosis for the current visit, continuity of care information, existing chronic conditions, diagnostic and screening tests ordered or provided in the office, procedures, medication therapy, types of providers seen, and provision of preventive health education during the targeted study period. Either the physician or their staff report the data or the Census field representative abstracts the data from the medical charts. The survey methodology including sampling design, data instruments, and data collection procedures are described in detail elsewhere.19 All the services provided by the physician were divided into categories: (1) examinations/screening, (2) lab tests, (3) imaging, (4) procedures, (5) treatment, and (6) health education/counseling (complete list of services found at https://www.cdc.gov/nchs/data/ahcd/2016_namcs_prf_sample_card.pdf).20
Methods
We used 2 approaches to quantify the telehealth capacity of the primary care physicians: (1) examine distribution of e-consults and telephone consults and (2) all the encounters amenable to telehealth in a primary care office-based setting. Primary care specialty included general practice, family practice, internal medicine, and pediatrics.
We used the following question to calculate the proportion of physicians providing the following types of visits *“During the last typical week of practice, did you make encounters of the following types with patients: (1) telephone consults, (2) internet/e-mail encounters with patients, (3) nursing home visits, (4) home visits, and (5) hospital visits. Each of these options was recorded as ‘1’ if the physician answered “yes,” ‘0’ and if they answered “no.” Blank, unknown, and refused answers were set to missing.
To determine which services were amenable to delivery through telehealth, we first conducted an environmental scan of peer-reviewed telehealth literature and created a list of services amenable to telehealth. This list was then shared with a group of primary care physicians who either had use telehealth in the past or were currently using video-enabled or telephone only telehealth during the COVID pandemic. (See Appendix Table 1 & Table 2) Each of the services was recoded as a dichotomous measure (0/1). The patient-physician encounters where the physical presence of the physician was required to conduct at least 1 service were deemed as not amenable to telehealth and were coded as ‘0’. All the encounters where the physical presence of the physician was not required were considered amenable to telehealth and coded as ‘1’.
Distribution of Patient-Physician Encounters by Patient Characteristics and Telehealth Amenability
Proportion of Patient-Physician Encounters Amenable to Telehealth
We calculated the total number and percentage of physicians and visits in the study sample. We used univariate statistics to examine the number and proportion of physicians who provided e-consults and telephone consults. We also calculated the number and proportion of patient-physician encounters that were amenable to telehealth. Distribution of patient socio-demographic characteristics by telehealth capacity was also examined. We also looked at the distribution of practice characteristics of the physician sample. All data were weighted to obtain nationally representative estimates of the patient-physician interactions and physicians using patient and physician weights. We used survey variables to account for the complex NAMCS survey designs.
The current study was approved by the Institution Review Board, American Academy of Family Medicine.
Results
There were 677 physicians (weighted n = 330,605) in the 2016 and 13,615 patient-physician encounters (weighted n = 883,725,178) in the NAMCS 2016. Of the total physicians 41% were primary care and 59% subspecialists. Greater proportion of physician practices were in MSA than non-MSA (unweighted 93.4% vs 6.6%), were owned by physicians or physician group (unweighted 74.7%) and located in the South (40.2%) (Appendix Table 3).
Proportion of Services Amenable to Telehealth
Nearly 30% of visits in patients 65 years and older were telehealth amenable compared with 42% in patients aged 18 to 34 years. (Table 1) A third of the patient-physician encounters related to hypertension (31% vs 69.0%, P < .021) and almost a quarter of the visits to coronary artery disease (24.7% vs 75.3%, P < .010) were amenable to telehealth. About 45% of the visits for depression were amenable to telehealth (44.9% vs 55.1%, P < .001).
Among all physicians in the 2016 analysis sample, 44% reported making a telehealth encounter, 16% made e-consults and 42% telephone consults. (Figure 1) Of the primary care physicians in the 2016 sample, 47% made any telehealth encounter, 19% provided e-consults, and 44% provided telephone consults. In total, of the 850 million patient-physician office-based encounters (all specialties), 35% were amenable to telehealth using the guidelines outlined above. Among all the patient-physician interactions in ambulatory primary care settings (n = 394 million), 42% were amenable to telehealth. (Table 2). Of all the office-based visits, 70% of services rendered at the visit were telehealth amenable (Table 3), as were 73% of services provided by primary care physicians.
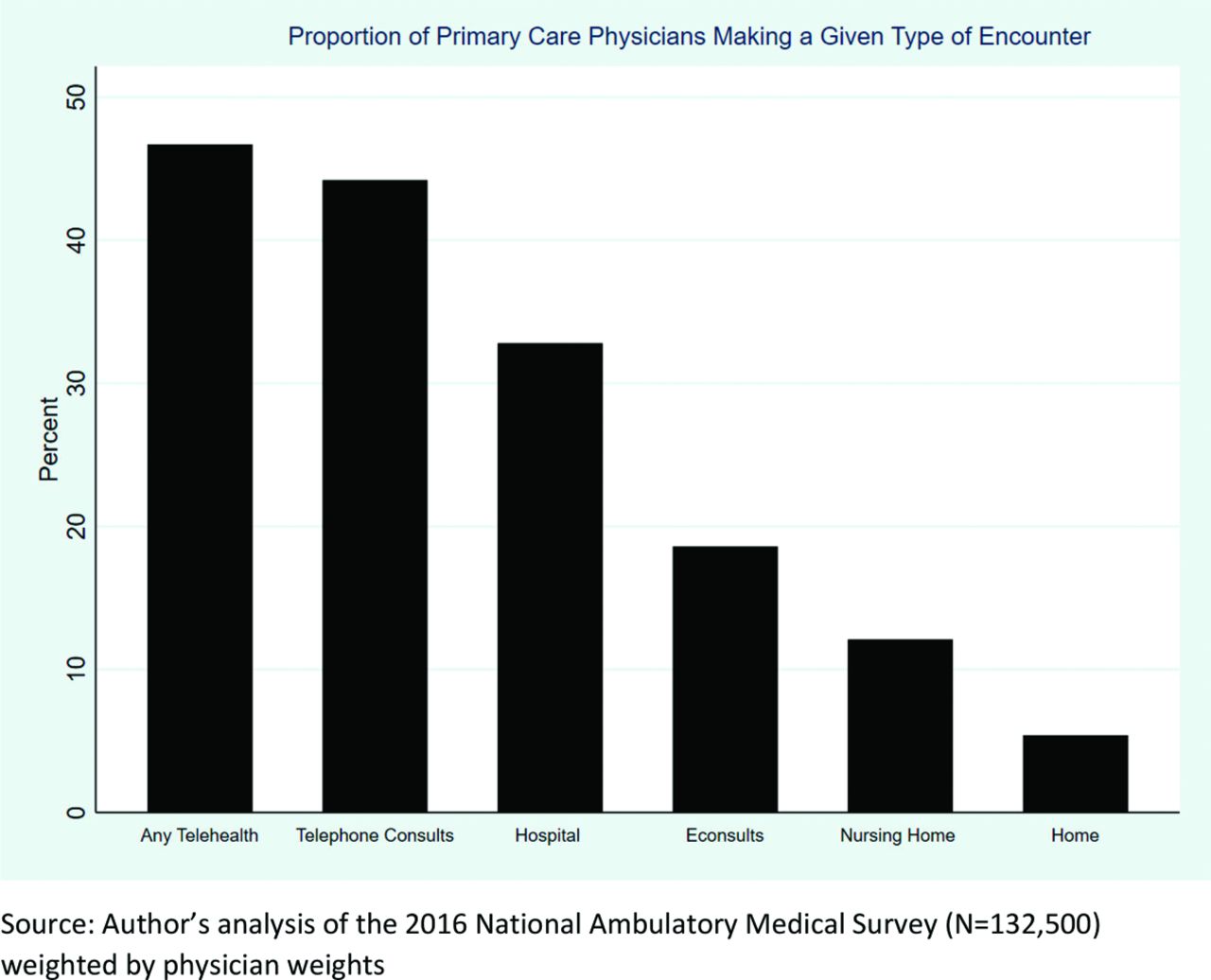
Proportion of primary care physicians making a given type of encounter (weighted) (NAMCS 2016).
Discussion
This study estimates the capacity of primary care to provide telehealth services for COVID-19 related illness, and several other acute and chronic medical conditions.
By our estimates, before COVID-19, 41% of physicians and 47% of primary care physicians report using some sort of telehealth in their office, with telephone encounters being the most frequently cited type of telehealth visit. While many primary care physicians report the capacity to provide telehealth, few of the visits coded in NAMCS were delivered via telehealth. We found that a number of services provided (73%) and a smaller but significant number of encounters (42%) could have been delivered via telehealth.
The predominant form of telehealth provided in our sample was via telephone. This makes sense given that the telephone is available in 100% of practices and nearly 100% of patient homes.21 Yet, telephone only visits are reimbursable by some payers, they are currently reimbursed at a fraction of the rate of video visits. This has grave financial implications for practices without the infrastructure to support video visits or those that serve patient populations without access to broadband, smartphones or computers.
There is substantial evidence that medically underserved populations, particularly in rural communities, have a lower likelihood of having access to the technology needed to sustain video virtual visits.22 Previous studies cited multitude of reasons for demographic disparities in telehealth use including mistrust in use of technology for obtaining care, poor health or technology literacy in seeking health care.23,24 A Kaiser Permanente survey demonstrated fewer older and minority patients owned digital devices and had lower ability or were less willing to use internet or email.25 Likewise our study also shows patients aged 65 or more and those with chronic conditions less likely to engage in telehealth, which underscores the importance of patient education and training in promoting the use of telehealth services in these subpopulations. Without either a change to value-based payments or much higher reimbursement rates for telephone visits, we may end up disproportionately adversely affecting practices that support patients with the highest medical and social needs.
This study highlights the need to understand how and where primary care might be delivered. With the advances in virtual care available through telephone, smart phone, desk top cameras, and text, e-mail, and patient portals it is essential to understand the benefits and risks to these care options. While synchronous communication via in-person, face-to-face encounters has been the dominant model, other opportunities for communication have been developed, but under deployed. Meaningful medical encounters may be provided by other synchronous communication through video and audio-only methods. Asynchronous communication may also be a robust method for delivering primary care. Symptom review, feedback, prescription refills, chronic disease management, education, and counseling may all be done via e-mail, text, and other asynchronous methods. It is crucial to provide funding to all forms of quality patient interaction and service provision. The COVID-19 pandemic has led to a realization that some important elements of primary care can be delivered by a patient’s local primary care clinician using a host of virtual telehealth methods.
The activities included as amenable to telehealth are a group of general activities included in the NAMCS data collection. As such, they are not specific, diagnosis-related, and do not include a variety of other clinical activities that might be conducted by telehealth. Because NAMCS includes just a small set of general activities, not every encounter with a specific service would be amenable to a virtual visit. For example, while there is evidence that many dermatologic conditions can be amenable to telehealth,10 not all dermatologic conditions could be fully managed without a skin scraping or direct treatment. While some visits would not require a patient to be physically in the office, the visit may necessitate the patient travel to another site for lab or imaging. This could be a virtual visit combined with a potential need for lab tests, therefore amenable to telehealth. Emerging digital devices such as home blood pressure machines, home spirometers, and pulse oximetry may provide additional care that can be provided without an in-person visit. However, many of these newer devices are not widely available and represent an area of research and evaluation. We recognize that our estimates may be conservative given the lack of a standard definition of telehealth. Nevertheless, these data provide an important glimpse into the potential to expand telehealth for many common acute and chronic conditions.
Study Limitations
NAMCS is a survey of physicians and is therefore subject to bias of the respondents, although, this bias is minimized by a sophisticated data collection process that allows for validation from multiple sources. In addition, we are estimating telehealth capacity by calculating the number of visits that are amenable to telehealth. We are not commenting on the quality of these visits if done via telehealth or in person. Although there is room for more research on the quality of telehealth visits, much of the current research shows that for those visits that are amenable to telehealth, little to no difference in outcomes between visits done in person via telehealth.10⇓⇓–13,26
Physicians who participated in the survey but did not see any patients by telehealth during the reporting period and those who refused to participate in the survey were excluded from the public use data. Therefore, estimates for physicians derived from the encounter data may vary slightly from all office-based physicians. For some items the nonresponse bias exceeded 5%, although NAMCS adjusted for nonresponse bias. Finally, the decision to include a service as potentially amenable to telehealth was made by a small group of primary care physicians supported by peer-reviewed literature. While there may be some disagreement among physicians and patients as to what services can be delivered via telehealth, based on NAMCS data collection methods, the list of services assigned as telehealth amenable is a reasonable approximation of the medical services that might be delivered via telehealth.
Since our study is based on 2016 NAMCS data, it does not include CMS changes in telehealth reimbursement and state legislations made in 2019 that impact telehealth adoption rates among physicians, limiting generalizability of our study findings.
Conclusions
The current study estimates the telehealth capacity in the United States using a nationally representative data source. We found that 35% of all visits and 42% of primary care visits are amenable to any kind of telehealth. Our estimates are higher than the 14% ambulatory telehealth visits reported by Mehrotra et al. during early weeks of COVID-19 pandemic in the US.27 However, authors Mehrotra postulate that 40% of all the patient visits could be done via telehealth, which is comparable to our study estimates.28 Before the COVID-19 pandemic, it would be hard to imagine that nearly half of all visits to a primary care office could be done virtually. Yet, in a matter of weeks, health care providers nationwide have completely redesigned their practices using telehealth to sustain care capacity while maintaining social distancing and protecting patients and providers. This rapid transformation will undoubtedly change how we deliver care in the post-COVID-19 era. And although telehealth will likely not be provided at pandemic-era levels, it is likely to be provided more frequently than before. Successful practice transformation in the coming months may highlight areas in which primary care can more fully integrate telehealth modalities in the future. Whether paid for through traditional fee-for-service payment models or expanded prospective payment models, telehealth services may be a substantial component of primary care now and in the future. Our estimates of the telehealth capacity in the outpatient primary care setting may be by practices as they plan how they will deliver care by payers as they make payment model decisions in the post-COVID-19 environment.
Appendix 1. Classification of Services Amenable to Telehealth
Appendix
Appendix 2. Literature Support for Services Amenable to Telehealth (Telehealth Capacity = 1)
Appendix 3. Distribution of Patient-Physician Encounters by Physician Practice Characteristics (NAMCS 2016)
Notes
This article was externally peer reviewed.
Funding: No funding received for this study.
Conflict of interest: We have no conflicts of interest to disclose.
Author contributions: All authors collectively and independently are responsible for the content and made substantial contributions to this paper. Specifically, Anuradha Jetty, Yalda Jabbarpour, and John Westfall designed and developed the study concept. Matthew Westfall conducted the literature review and helped in drafting the introduction section. Douglas Kamerow, John Westfall, Yalda Jabbarpour and Anuradha Jetty examined all the services available in the NAMCS data and classified them into telehealth amenable and non-telehealth amenable. Anuradha Jetty analyzed the data, interpreted results, and drafted the results and methods sections. Yalda Jabbarpour drafted the discussion section and concluding remarks. Stephen Petterson interpreted the results, reviewed the manuscript for intellectual and critical content. Douglas Kamerow and John Westfall reviewed the manuscript for intellectual and critical content.
To see this article online, please go to: http://jabfm.org/content/34/Supplement/S48.full.
- Received for publication May 7, 2020.
- Revision received July 23, 2020.
- Accepted for publication July 26, 2020.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- The Impact of Telehealth on Primary Care Physician Panel Sizes: A Modeling Study
- The Impact of Telehealth on Primary Care Physician Panel Sizes: A Modeling Study
- European Respiratory Society statement on long COVID follow-up
- Points of Concordance, Points of Discordance: A Qualitative Examination of Telemedicine Implementation
- Association of Telehealth with Short-Interval Follow-Up
- Practice Adjustments Made by Family Physicians During the COVID-19 Pandemic
- Primary Care in the COVID-19 Pandemic: Essential, and Inspiring