
- Centers for Medicare and Medicaid Services
- U.S.
- COVID-19
- Family Medicine, Health Policy
- Primary Health Care
- Telemedicine
The Coronavirus disease-19 (COVID-19) pandemic reaches back months on American soil and even farther globally. Though the far-reaching effects were unknown at the outset, many scholars correctly predicted that the US health care system was not prepared to effectively handle a pandemic of this magnitude.1 Although the focus of the shortcomings of our health care system has been on lack of personal protective equipment and intensive care unit capacity, the lack of support for primary care has been devastating. A primary care collaborative survey released in March showed 52% of primary care providers reporting severe or close to severe financial effects on their practices due to COVID-19.2 One week later results from the same survey reported 76% with severe or close to severe financial effects on their practices. Modeling analysts predict that this financial impact could lead to primary care shortages nationwide.3 Although the reasons for this financial impact are multifactorial and cannot be blamed on any single entity, we sought to understand how the timeline of Centers for Medicare and Medicaid Services (CMS) policy changes may have impacted primary care practices in the United States.
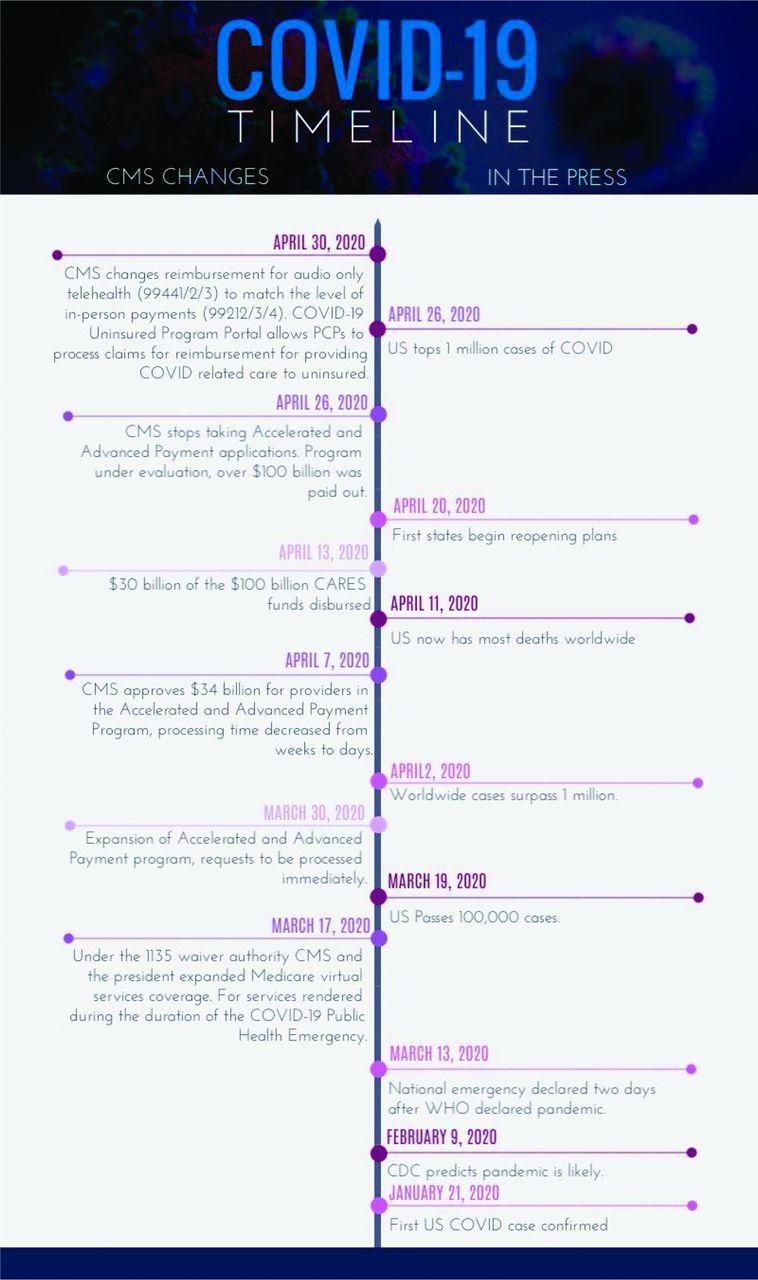
Using publicly available data on the CMS website we created a timeline of policy changes related to the COVID-19 pandemic, with a focus on reimbursement and telehealth changes. We also used publicly available data from the Centers for Disease Control and Prevention (CDC) to plot the number of COVID-19 cases against these CDC changes. Figure 1 details the timeline of some of the changes made to CMS juxtaposed with the disease progression.

A descriptive timeline of the changes made by Centers for Medicare and Medicaid Services (CMS) during the COVID-19 pandemic juxtaposed against popular events in the press at the time.
Changes allowing for telehealth expansion came almost a month after the pandemic was predicted on March 17, 2020. Although these changes may have been fast by Medicare standards, the month delay between the formal World Health Organization pandemic announcement and CMS changes in the face of an unprepared system may have been too long for practices to wait. In fact, the primary care collaborative survey that showed severe financial effects on primary care practices nationwide was released just 2 days after telehealth expansion was finally announced. But perhaps more troubling was that the same survey showed that 70% of practices had no e-visit capability and 60% had no access to video visits.3 The CMS changes on March 17th focused significantly on increasing the availability of telehealth reimbursement, but practices were not technologically configured to embrace this change from the in-person visits they financially relied on. By the time the April first data of the PCC (primary care collaborative) report was released still nearly 40% of practices had no access to HIPAA-compliant video systems – the more highly reimbursed method of care delivery at that time – and only one third of practices felt they had enough cash on hand to keep their practices open for 4 weeks.3 Physicians in the survey reported increasing administrative burden with even less staff, and as noted in the timeline, efforts by CMS to ease paperwork requirements like Prior Authorizations did not go into effect until March 30th.
The Accelerated and Advanced Payment program, whereby practices could receive advanced payments based on prior claims data, went into effect on March 30th with approvals following shortly after on April 7th and payouts beginning on April 13th. This is a rapid turnaround, but even so, looking back at the survey data it is clear that for those practices unable to weather 4 weeks of financial strain it was too late. This underscores finances as one of the key reasons that Health Landscape data predicted a reduction of almost 20,000 Family Medicine Physicians and with them over 200,000 other jobs and over $20 billion in lost wages.4 This projected loss accounted for an additional 287 counties across the country with a shortfall in health care providers – an over 25% increase in just 1 month.4 Granted not every closure is financial in cause, and perhaps not every closure is permanent, but even so, these losses occur at a time when we need medical care more than ever. The timeline illustrates a relatively quick pace of response, but reality shows us that this alone was not enough to save practices. What we need in the future is a more robust plan to support primary care when in-person visits rapidly decline.
A move toward value-based payments and alternative care delivery models would free primary care practices from some documentation burdens and allow for a more agile and financially sound pivot if in-person visits become a health risk in future crises. Here we might consider a practice model like ChenMed, a multi-state medical group serving vulnerable Medicare Advantage beneficiaries that do not depend on fee-for-service revenue. Without reliance on fee-for-service revenue, practices like ChenMed were able to weather the decline of in-person visits and not only survived but continued to open practices through COVID-19 instead of closing them.5
Shifts to value-based payment would have the added benefit of allowing practices to continue to financially support the telehealth services that have grown out of this current pandemic. Value-based practices such as ChenMed were able to convert 95% of their visits to telehealth within 1 week.5 Telehealth is well received by patients with 1 study finding 95% satisfied with the care they received via a telehealth platform.6 Telehealth also represents a more efficient way to provide care for certain conditions, allowing for interval visits that are more convenient for patients and quicker for providers. Improving provider efficiency and providing primary care physicians with alternative, financially sound methods of caring for patients may even help reduce the burnout rates in primary care which are more than 50% today.7,8
Our ability to surmount health crises as they arise depends significantly on our ability to deliver effective primary care, and that means keeping practices open in the face of a dynamic economy and ensuring they are well equipped to provide care in flexible ways. The timeline presents the stark reality that crises evolve quickly. The data around primary care loss, the survey results from individual practices, and the realities of our health care system underscore the need for a more thoughtful approach to our future preparations. The future stability of primary care requires congressional changes to move us toward value-based care and investments in primary care infrastructure as well as a partnership from local and national health care systems to support these changes.9 Primary care is the backbone of our health care system and we have a responsibility to ensure we make changes to support it for the future.
Notes
This article was externally peer reviewed.
Funding: None.
Conflict of interest: None.
Disclosures: None.
To see this article online, please go to: http://jabfm.org/content/34/Supplement/S7.full.
- Received for publication June 21, 2020.
- Revision received September 25, 2020.
- Accepted for publication September 29, 2020.




{kind=link}