
Abstract
Background: Although treatment for new back pain is heavily guideline driven, deviations occur frequently. Neighborhood socioeconomic status (nSES) may contribute to these deviations.
Objective: Determine whether nSES is associated with type of treatment provided for patients seeking treatment for new back pain in primary care clinics.
Methods: This retrospective cohort was conducted in academic internal and family medicine practices. Data were examined from the Primary Care Patient Data Registry. Eligibility criteria included age ≥18 years, free of HIV and cancer, and presenting to primary care with a new diagnosis of back pain, resulting in1646 patients included. Patients’ nSES was determined using ZIP code and calculating a validated index of 7 census-tract variables. Multinomial logistic regression was used to measure the association between nSES and 3 treatment outcomes compared with no pharmacologic management. Outcomes included opioid prescription, nonsteroidal anti-inflammatory (NSAID)/muscle relaxant prescription, or combined opioid/nonopioid treatment within 90 days of initial presentation. Covariates included age, sex, race, high clinic utilization (HCU), depression, anxiety, substance use, obesity, comorbidities, smoking, number of pain conditions, and physical therapy (PT) referral.
Results: The cohort was 67.9% female with an average age of 55.72 years (Standard Error [SE] = 0.387). Compared with no pharmacologic treatment, individuals in the low nSES group had 63% higher odds of receiving an opioid only compared with the high nSES group (odds ratio [OR], 1.63; 95% confidence interval [CI], 1.01 to 2.62). There was no significant association between nSES and odds of nonopioid or combined treatment compared with no pharmacotherapy (OR, 1.17; 95% CI, 0.97 to 1.50), (OR, 1.09; 95% CI, 0.67 to 1.78), respectively. Covariates associated with increased odds of opioid only included HCU, ever smoker, and increasing comorbidity index. PT referral was associated with NSAID/muscle relaxant only, and increasing age and comorbidity index were inversely associated with odds of NSAID/muscle relaxant only. Finally, covariates associated with increased odds of receiving both therapies included high clinic utilizusation, ever smoking, and PT referral.
Conclusions: These data characterize a possible association between low nSES and increased risk of receiving an opioid only when being treated for new back pain. This may be evidence that patients of low nSES are at increased risk of receiving guideline-noncompliant treatment for new back pain.
Primary care physicians are the most common source of opioid prescriptions in the United States.1⇓–3 Among painful conditions in primary care, back pain is the diagnosis most commonly prompting opioid prescription.4 Opioid prescriptions are written despite multiple recommendations against the use of opioids, especially in acute back pain, given that their use is associated with worse pain and functioning in the long term.5⇓⇓–8 Studies have also demonstrated that although guidelines for the management of acute back pain are freely available, physicians frequently deviate.9⇓–11
There is little robust data to explain why physicians deviate from guidelines. Data do suggest that the social determinants of health may play a role in decision making. Specifically, patient characteristics such as sex, insurance status, and race are associated with differences in opioid prescriptions given for painful diagnoses.12⇓–14 In emergency department (ER) and primary care visits for pain, studies have demonstrated that African Americans and women are less likely to receive opioids for acute pain.12,15⇓–17 These racial differences are thought to contribute to the disproportionate effect of the opioid epidemic on the white population.18
The influence of the social determinants of health cannot be fully explored without addressing socioeconomic status (SES). However, SES has been difficult to quantify as a meaningful contributor to patient outcomes. In light of this challenge, several proxies have been used, including individual income, level of education, and neighborhood socioeconomic status (nSES). nSES is a particularly attractive proxy as it describes the milieu in which a patient resides, which may drive patient expectations and behaviors. For instance, low nSES is associated with multiple high-risk health behaviors such as smoking, drug abuse, and alcoholism.19 Low nSES is also associated with poor health outcomes, including obesity, heart disease, renal disease, and increased cancer mortality.20⇓⇓⇓–24 Finally, nSES has been associated with differences in nonpharmacologic management of medical problems.25
To further characterize the influence of nSES, studies have been conducted that suggest nSES may influence pain treatment modality. Joynt et al15 examined how race and a measure of nSES may influence treatment of pain. In particular, lower nSES was associated with a lower likelihood of patient’s receiving an opioid prescription, independent of race. In contrast, Ndlovu et al26 found the opposite effect; that higher levels of neighborhood deprivation was associated with higher likelihood of strong analgesic (mostly opioid) therapy. Thus, patients living in postal codes with more poverty were more likely to receive an opioid.26 Given the conflicting nature of the evidence available, the frequency of back pain and the potential poor prognostic implications of early opioid use, we sought to determine whether nSES, independent of race, is associated with type of pain treatment provided for new back pain visits in primary care.
Methods
Subjects
Clinical data were obtained from the Department of Family and Community Medicine’s Primary Care Patient Data Registry (PCPD). The PCPD consists of 33,661 patients who had at least 1 family medicine or general internal medicine encounter between July 1, 2008 and June 30, 2015 at any of 3 academic primary care practices in St. Louis. Practices are located in both urban and suburban regions of St. Louis, including high and low income neighborhoods. The PCPD contains ICD-9-CM codes, prescription orders, CPT codes, social history, family history, demographics, laboratory orders, referrals, and vital signs. The protocol for creating this database and its use in numerous clinical epidemiologic and health services research studies has been previously described.27⇓⇓⇓⇓⇓⇓–34 The study procedures were reviewed and approved by the university Institutional Review Board (IRB).
Eligibility Criteria
For this retrospective cohort design, eligible patients had to be 18 years or older and free of human immunodeficiency virus (HIV) and cancer diagnoses (n = 30,431). Because we modeled treatments for new back pain encounters, eligible patients must have had at least 1 clinic encounter and have no back pain diagnosis in the 18-month “washout period” from July 1, 2008 to December 31, 2009 (n = 9194). Following the washout period, eligible patients must have had at least 1 visit with a back pain diagnosis (ICD-9 codes:720.1, 720.2, 720.8x, 720.9, 721 to 722 (all), 723.0 to 723.3, 723.5 to 723.7, 723.9, 724 (all), 756.1x) between January 1, 2010 to June 30, 2015 (n = 1652) and have a minimum of 90 days of follow-up time. Patients with missing demographic data were excluded leaving a final analytic sample size of 1646. The sample selection is shown in Figure 1.
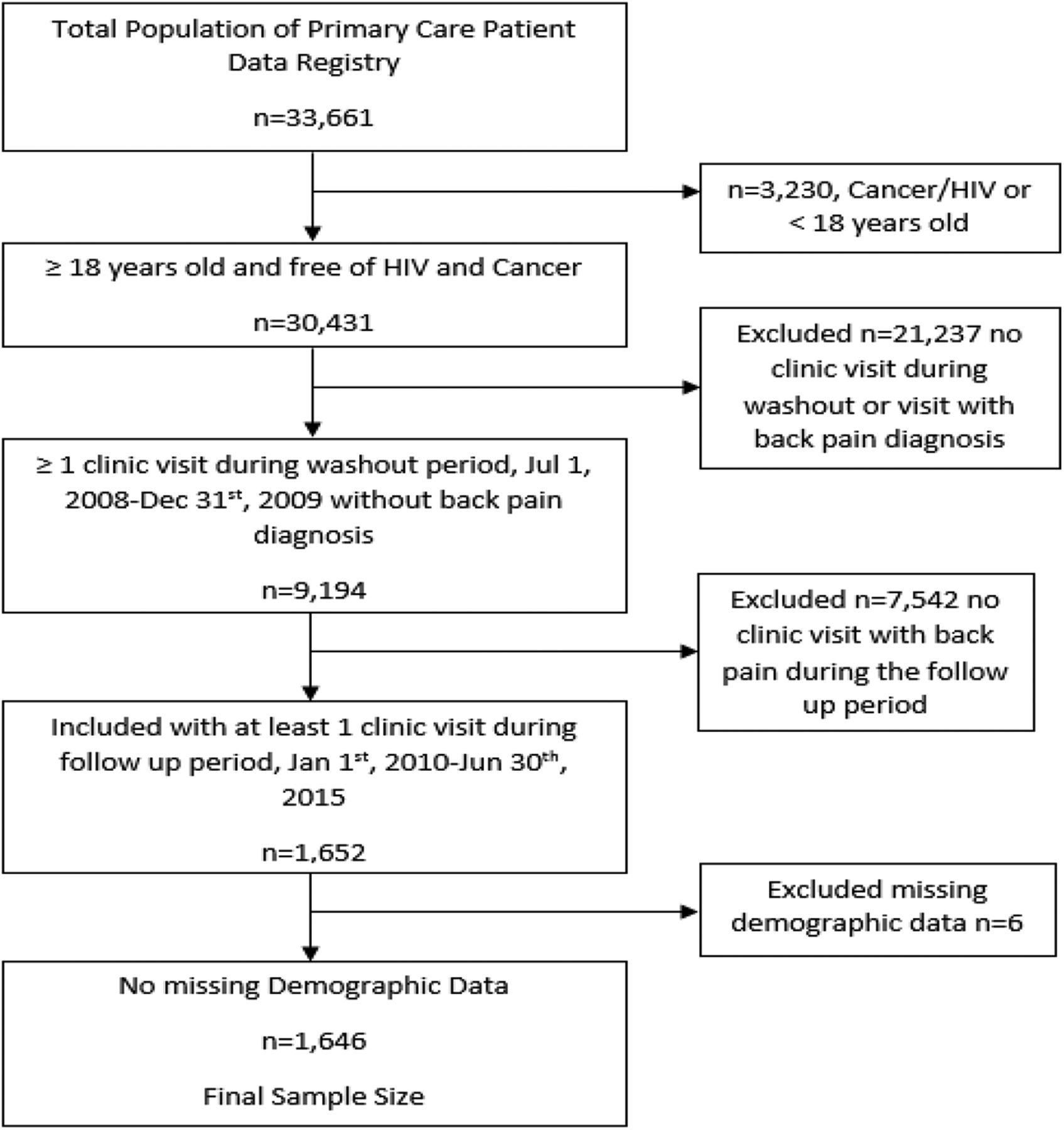
Flow of patient inclusion in final sample.
Exposure
A nSES index was adapted from a previously verified measure composed of 7 measures obtained from the 2008 to 2013 5-year census estimates from the American Community Survey.35 Each patient’s 5-digit ZIP code was linked to each of the 7 variables of the index, including: 1) Percent of households with income below the poverty level, 2) percent of households receiving public assistance, 3) percent of households with an annual income below $35,000, 4) percent of adult males age 20 to 64 years not in the labor force, 5) percent of adults 25 and older with less than high school education, 6) log of median household income, and 7) log of median value of single family homes. The index was then standardized to represent the 33,120 ZIP codes in the United States, where lower index score indicated higher nSES. The distribution of the scores of the 1326 ZIP codes represented in our overall patient population was used to assign patients to either low nSES and high nSES groups based on a median split.
Outcomes
The composite outcome of interest for management options offered during the 90 days following the index back pain diagnosis was based on prescriptions for any opioids and any nonopioids, defined as any nonsteroidal anti-inflammatory (NSAID) or muscle relaxant. Opioid prescriptions included any of the following medications: codeine, oxycodone, fentanyl, hydrocodone, hydromorphone, morphine, oxymorphone, pentazocine, levorphanol, and meperidine. NSAIDs/Muscle relaxants included celecoxib, diclofenac, diflunisal, etodolac, fenoprofen, flurbiprofen, ibuprofen, indomethacin, ketoprofen, ketorolac, meclofenamate, mefenamic acid, meloxicam, naproxen, nabumetone, oxaprozin, piroxicam, sulindac, and tolmetin for NSAIDs and carisoprodol, cyclobenzaprine, baclofen, dantrolene, metaxalone, methocarbamol, chlorzoxazone, tizanidine, and orphenadrine for muscle relaxants. The outcome variable was coded into quartiles: a) no medication management (none); b) opioid only; c) NSAID or muscle relaxant only; and d) both opioid and NSAID/muscle relaxant.
Covariates
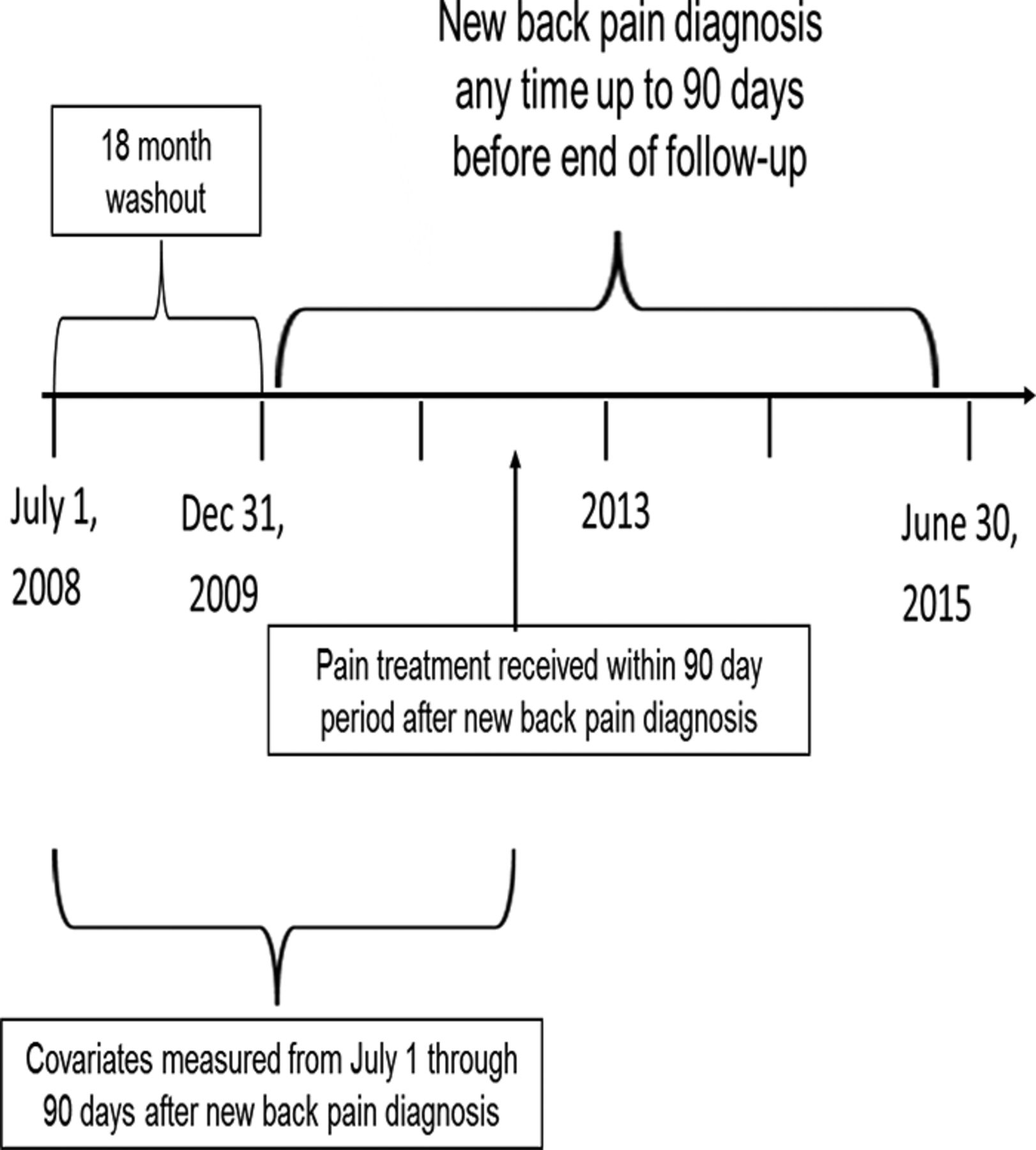
Other variables assessed for inclusion in analyses were patient age, race, sex, high clinic utilization, smoking status, any substance abuse/dependence, depression, any anxiety, obesity, comorbidity index (CMI), self-reported use of over the counter (OTC) medications before index visit, and physical therapy referral. These covariates were selected based on previous literature identifying them as influencing treatment offered for pain.13,16,17 Age was coded as a continuous variable in years. Race was coded as a bivariate variable, white and nonwhite. Clinic utilization was computed by generating the distribution of the average number of clinic encounters per month. The top 25th percentile of the distribution were defined as high clinic utilization and the bottom 75% of the distribution was considered not high clinic utilization. Smoking status was obtained from social history or ICD-9-CM code for nicotine dependence, and defined as ever (former or current smoker) or never. Any substance abuse/dependence was ascertained through ICD-9-CM codes for alcohol or drug abuse or dependence. Depression and any anxiety (posttraumatic stress disorder, generalized anxiety disorder, panic disorder, obsessive compulsive disorder, social phobia, or anxiety disorder unspecified) were determined by the presence of at least 2 ICD-9-CM codes in the chart within the same 12-month period. Two diagnoses in the same 12-month period for depression is known to have excellent agreement with written medical record.36 Obesity was assigned as yes or no based on vital signs documentation of Body Mass Index (BMI) ≥30.00 or ICD-9-CM code for obesity. Continuous Comorbidity Index (CMI) score was determined using a previously verified protocol composed of 17 health conditions associated with increased morbidity and mortality.37 Comorbidities were ascertained any time before and up to 90 days post back-pain diagnosis. Use of OTC medications, such as naproxen and ibuprofen, was ascertained from the self-reported medication list. A diagram of the study design is shown in Figure 2.

Diagram of time line of study design.
Analysis
Data were analyzed using IBM SPSS 23. Differences in the distribution of covariates and the treatment outcome variable by nSES group were assessed using independent samples t test for continuous variables and a χ2 test for categorical variables. All covariates were then assessed for associations with the 4-level treatment outcome variable using a 1-way ANOVA and χ2 test for continuous and categorical variables, respectively. Odds ratios and 95% confidence intervals (CIs) were computed using unadjusted and adjusted multinomial logistic regression models to measure the association between nSES and treatment received before and after adjusting for covariates, with no treatment as the common referent category. Covariates identified as statistically significantly associated with the type of pain treatment received (P < .05) were included in adjusted multinomial logistic regression models. All statistical significance was determined at a significance level P < .05.
Results
Among the cohort of 1646 patients with acute back pain, 54.7% were white, 67.9% were female, and the mean age was 55.7 years. Bivariate associations between nSES, covariates, and treatment outcome are shown in Table 1. Distribution of treatment outcomes was significantly (P = .032) associated with nSES, with 8.1% of low-nSES patients receiving an opioid prescription compared with 5.0% of high-nSES patients. NSAID/muscle relaxant therapy prescription occurred in 32.7% of low-nSES patients compared with 31.0% of high-nSES patients. Among low-nSES patients, 5.9% received both pharmacologic treatments compared with 5.5% of high nSES. Finally, 53.3% of low-nSES patients received no treatment, whereas 58.5% of high-nSES received no treatment. Other covariates significantly associated with nSES included age, race, high clinic utilization, smoking status, anxiety, substance abuse, obesity, and CMI (P < .05 for all).
Unadjusted Associations between nSES and Covariates
Associations between covariates and type of treatment provided within 90 days of a new back diagnosis are shown in Table 2. Age was significantly associated with type of treatment with NSAID/muscle relaxant treatment associated with younger patients compared with any other treatment. Patients treated with NSAIDs/muscle relaxants also had the lowest health care utilization (P < .0001) and were least likely to be ever smokers (P < .0001). Opioid-only treatment was also associated with the highest CMI, followed by no treatment, and lowest CMI was associated with NSAID/muscle relaxant only treatment (P < .0001). Patients with higher CMI were more often treated with NSAID/muscle relaxants or both opioid and NSAID muscle relaxants (P < .0001). Finally, physical therapy was most often associated with both pharmacologic treatments and NSAID/muscle relaxants only.
Unadjusted Associations between Covariates and Outcomes
Unadjusted and adjusted multinomial logistic regression results are shown in Table 3. In this unadjusted model, patients in low-nSES areas have 80% higher odds of receiving an opioid only rather than no pharmacologic therapy, compared with patients in high-nSES areas (odds ratio [OR], 1.80; 95% CI, 1.19 to 2.72). Odds of receiving NSAID/muscle relaxants or both pharmacologic treatments verses no treatment were not significantly associated with nSES.
Results of Crude and Adjusted Multinomial Logistic Regression
After adjusting for covariates, patients with low nSES verses high nSES had a significantly greater odds of receiving an opioid compared with no treatment (OR, 1.63; 95% CI, 1.01 to 2.62). nSES was not associated with odds of NSAIDs/muscle relaxants or receiving both treatments compared with no treatment. Compared with no pharmacotherapy, odds of receiving an opioid within 90 days of a new back pain diagnosis were significantly greater among patients who were high health care utilizers, ever smokers, and among patients with higher CMI scores. In addition, compared with no treatment, age and CMI were negatively associated with NSAID/muscle relaxant treatment and physical therapy (PT) referral was positively related. Finally, compared with no treatment, high health care utilization, ever smokers, and PT referral were positively associated with both pharmacologic treatments.
Discussion
In a large cohort of primary care patients, we observed low nSES was significantly associated with type of treatment received in the first 90 days following a new back pain diagnosis. Patients with low nSES verses those with high nSES were significantly more likely to receive an opioid prescription relative to receiving no pharmacotherapy before and after adjusting for covariates. However, nSES was not significantly associated with receiving an NSAID/muscle relaxant or both an opioid and NSAID/muscle relaxant relative to receiving no pharmacotherapy. In fully adjusted models, ever smoking was significantly associated with both receipt of an opioid alone and in combination with NSAID/muscle relaxant, and physical therapy referral was significantly associated with receipt of NSAID/muscle relaxant alone or in combination with an opioid. Higher CMI scores were positively associated with prescription of an opioid alone and negatively associated with receipt of an NSAID/muscle relaxant alone. In this data set, race was not significantly associated with type of pharmacological pain treatment for new back pain diagnoses.
Our results suggest an nSES treatment disparity for new back pain diagnoses exists in pharmacotherapy provided in the early phase (ie, within 90 days) of treating a new back pain diagnoses. The possible association between low nSES and increased odds of opioid prescription is in agreement with Ndlovu et al’s study finding that higher neighborhood deprivation was associated with higher risk of opioid prescription.26 Ndlovu26 also found that the majority of patients received no pharmacologic therapy, much the same as this study. However, this study presents contrast with the findings of Joynt et al15, which noted low nSES was associated with a 24% decrease in odds of opioid prescription. However, the study by Joynt et al15 was based in the emergency room (ER) where approaches to care may be different. Further, the provider-patient relationship in the ER environment is likely quite different from the primary care setting as well.38 Other explanations for our results should be considered. Our findings may reflect differences in insurance status, for which we were unable to control in this data set. In a study done by Kao et al12 examining National Hospital and Ambulatory Medical Center Survey Data, patients with no insurance or Medicaid were more likely to receive an opioid prescription. Given that a component of the nSES index used in this study includes percent of households receiving public assistance, it is likely that patients living in lower nSES areas are more likely to be publically insured. The other associations characterized between covariates and odds of opioid prescription alone have been supported in the literature. Increasing CMI has been associated with increased odds of opioid prescription.39 Several studies have noted that noted that higher clinic utilization is associated with either increased odds of opioid prescription or higher doses of opioid prescription.13,39 Further, low SES has been associated with higher clinic utilization for musculoskeletal problems, which is also consistent with our findings.40
Reasons for these findings regarding odds of opioid prescription by nSES level are unclear. One aspect of treatment modality offered is the preference of the patient. Patients may express doubts as to the efficacy of nonnarcotic pain medications and reject these treatment modalities. In a study using level of education as a surrogate for SES, patients with higher levels of education were found to be less likely to receive an opioid in the ER.41 A potential explanation may be that patients with higher levels of education are more ready to accept a nonnarcotic as efficacious, compared with patients with lower levels of educational attainment. However, this study is, again, limited by its setting in the ER and the ability to translate to the primary care realm. To further this idea, reassurance and education regarding the transient nature of acute low back pain is an important part of treatment.42 Level of education may play a role in the efficacy of any educational intervention, as well as the potential avoidance of deviations from treatment guidelines. Last, past opioid receipt may increase the likelihood of opioid prescription for incident back pain. To address the concern that previous opioid prescription biased the results, a sensitivity analysis was conducted among patients with no history of opioid use. The point estimate for the logistic regression for odds of opioid verses no pharmacotherapy decreased only slightly was not statistically significantly different from the original analysis, although the 95% confidence intervals were wider and the estimate became nonsignificant due to smaller sample size. This result indicates that history of previous opioid use did not moderate the effect of nSES on odds of opioid verses no pharmacologic therapy.
This study has several strengths, including use of real-world clinic data from over 100 primary care physicians, ability to focus on incident back pain, cohort design, and the standardized nature of our nSES variable, allowing for comparison with areas throughout the United States. This study also has several limitations. Lack of insurance measures makes it difficult to distinguish between nSES influence and insurance accessibility to alternative medications as motivators for choice of therapy. This may be less of an issue with this set of treatment options as the medication options are generic, so cost may be less prohibitive. We also do not include data from other specialties or the ER. However, given that these patients have been established with primary care providers, it is highly likely they would present to their primary care provider instead of going to the ER or another specialist. This data also lacks pain scores, which may drive treatment offered to patients. However, regardless of the pain score reported by the patient, opioids remain the last line and should be avoided for the treatment of acute low back pain as per guideline recommendations outlined previously. Finally, another limitation is the nature of the outcome variable as orders and not documented filled prescriptions. We do not know whether the patients actually filled their prescriptions after their office visit.
In conclusion, we demonstrate a possible association between low nSES and increased odds of opioid prescription compared no prescription for incident back pain. These data raise the possibility that low nSES puts patients at higher risk for inappropriate narcotic medication prescription and poor adherence by physicians to guideline driven therapy. Providers should be vigilant in evaluating the driving forces behind their prescribing choices and address patient concerns and motivators that may underlie these findings. More research is needed to further investigate how physician-driven reasons, patient-driven demands, or patient insurance status may contribute to this relationship.
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: none declared.
To see this article online, please go to: http://jabfm.org/content/30/6/775.full.
- Received for publication February 17, 2017.
- Revision received April 27, 2017.
- Accepted for publication May 2, 2017.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Opioid prescribing in the Netherlands during the COVID-19 pandemic: a national register-based study
- Association between sustained opioid prescription and frequent emergency department use: a cohort study
- BeatPain Utah: study protocol for a pragmatic randomised trial examining telehealth strategies to provide non-pharmacologic pain care for persons with chronic low back pain receiving care in federally qualified health centers
- Automatic Extraction of Social Determinants of Health from Medical Notes of Chronic Lower Back Pain Patients
- Patient, Provider, and Clinic Characteristics Associated with Opioid and Non-Opioid Pain Prescriptions for Patients Receiving Low Back Imaging in Primary Care
- Opioid Overdose in Ohio: Comprehensive Analysis of Associated Socioeconomic Factors
- Multiple Practical Facts and Ideas to Improve Family Medicine Care