
Abstract
Purpose: We investigated whether a tool using patient-entered wellness data to generate tailored electronic recommendations improved preventive care delivery.
Methods: We conducted a mixed-methods retrospective study of primary care encounters utilizing an Integrated Wellness Tool with a matched-comparison before-and-after study design. Encounters took place at a single clinic within the Cleveland Clinic Health System. The primary outcome was preventive orders placed. Index patients were matched, based on propensity scores, with comparison patients seen in the same clinic several months earlier.
Results: Five providers conducted 863 patient encounters using the tool during the study period. During encounters using the tool, providers placed more orders for smoking cessation programs (2.4 vs 0.5%, P < .01), lifestyle medicine (2.4 vs 0%, P < .01) and psychology (2.3 vs 1.0%, P = .04) consults, online nutrition (2.4 vs 1.4%, P = .04) and stress management (5.5 vs 0.9%, P < .01) programs, spirometry (5.9 vs 1.7%, P < .01) and polysomnography (6.3 vs 1.3%, P < .01) tests, and antidepressant (7.2 vs 3.9%, P = .01) and hypnotic (2.2 vs 0.7%, P = .01) medications when compared with matched encounters.
Conclusions: Patients are willing to enter lifestyle data, and these data influence provider orders.
- Counseling
- Life Style
- Preventive Medicine
- Primary Health Care
- Quality of Health Care
- Retrospective Studies
Modifiable behavioral factors confer the greatest risk for chronic disability and account for the leading causes of mortality in the United States.1,2 A primary care visit provides an opportunity to promote behavior change, and a majority of patients expect their primary care providers to help with lifestyle behaviors.3 Despite this, recommended counseling and education is delivered only 18% of the time.4 One often-cited barrier is the lack of organized systems to support the delivery of preventive services.5⇓⇓–8 With improved insurance coverage for preventive services, systems to efficiently identify patients' needs and facilitate delivery of the appropriate education, support, and follow-up resources are necessary.8,9 The collection of patient-entered lifestyle risk data could facilitate targeted lifestyle discussions between caregiver and patient, and link to order sets to expedite appropriate management and/or behavior change.10
The Integrated Wellness Tool (IWT) combines patient-entered wellness data with clinical data from the electronic medical record to provide risk scores and clinical decision support in the areas of nutrition, stress, exercise, depression, sleep, and breathing. This tool was designed and piloted in a single primary care clinic during the fall of 2013, and we conducted a retrospective cohort study of encounters using the tool during this period. Specifically, we examined the effects of the IWT on providers' preventive care order placement and on patient and provider perceptions of the tool.
Methods
We conducted a mixed-methods study including a retrospective chart review of primary care encounters using a matched-comparison, before-and-after study design. We also performed qualitative interviews with providers. The study was approved by the Cleveland Clinic Institutional Review Board. Informed consent was obtained before conducting interviews with providers.
The Integrated Wellness Tool
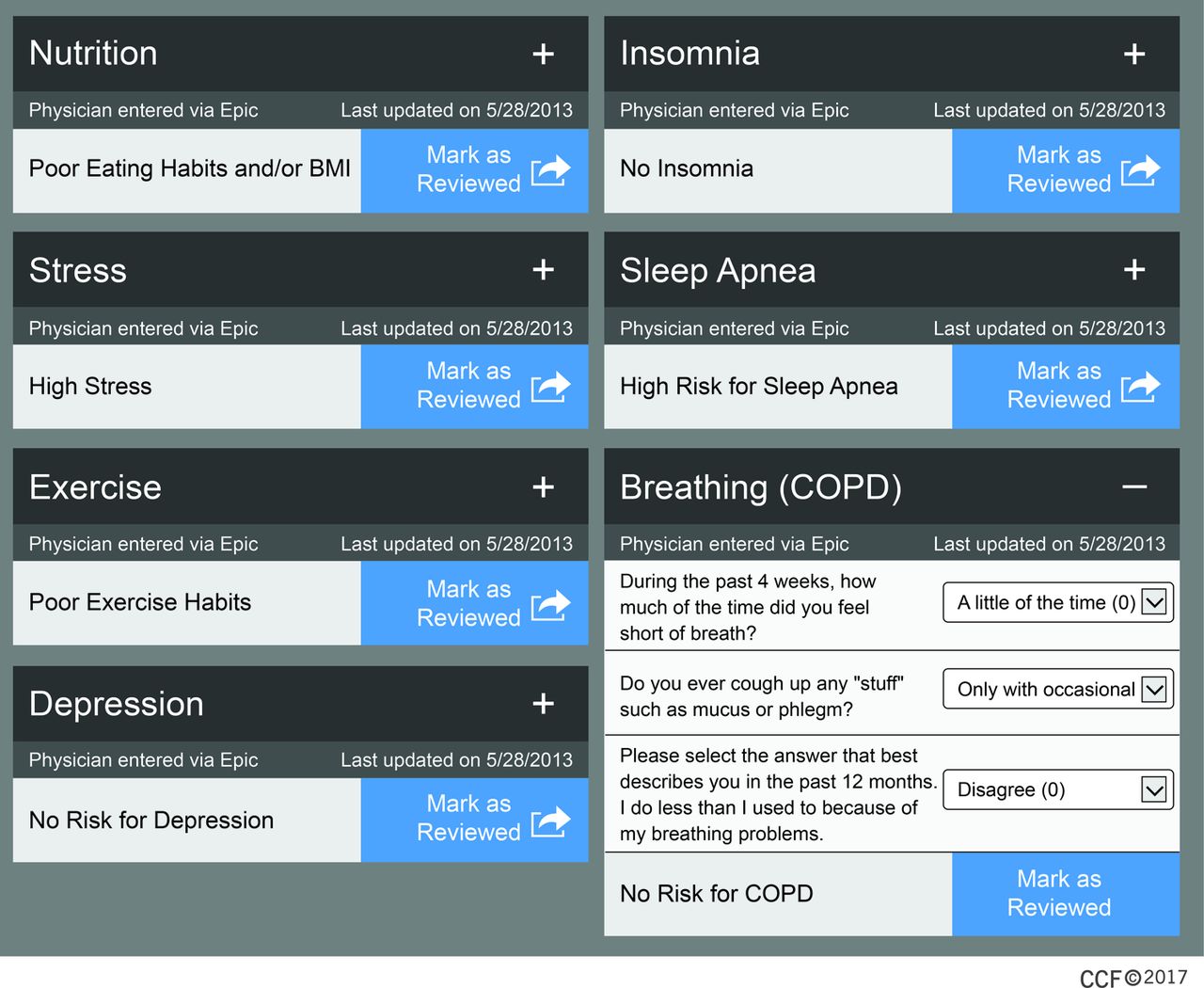
The IWT collects patient-entered data electronically and synthesizes it with data (age, smoking status, and body mass index) from the electronic medical record (EPIC Systems, Verona, WI) to provide clinical decision support at the point of care. Using a tablet device, patients complete brief questionnaires in the waiting room, and the IWT generates a risk score for each of the following areas: nutrition, stress,11,12 exercise,13 depression,14 insomnia,15 sleep apnea,16 and breathing.17 When providers open a patient's electronic chart, they are prompted to review these risk scores (Figure 1), clarify them during discussion with the patient, and mark them as “reviewed.” The questions and order sets that comprise the IWT were constructed by a group of caregivers from 10 specialties, with experience in questionnaire design, behavior modification, patient education, laboratory data extraction, risk analysis, and order set design. Based on the risk scores, the provider may be prompted to order a screening test, consult, or treatment. The questionnaire, risk score calculations, and recommendations for nutrition are included in Appendix 1. All patients who use the IWT receive printed informational handouts tailored to their individual risk scores after the visit.

Integrated Wellness Tool (IWT) provider electronic medical record interface. This interface may be viewed in the electronic medical record by providers after patients have completed the IWT. Risk scores are displayed for each wellness area, allowing providers to focus on those areas with the highest risk during the patient encounter. Providers may review and adjust patients' individual answers to the questionnaires and mark each area as “reviewed” using this interface. All patients automatically receive informational handouts tailored to their risk score in each wellness area. BMI, body mass index; COPD, Chronic Obstructive Pulmonary Disease.
Study Setting and Participants
Between June 25 and September 4, 2013, the IWT was pilot-tested in a primary care clinic within the Cleveland Clinic Health System. The IWT was offered once to all patients presenting to the clinic during this time period, except those who made urgent appointments or who arrived late for their appointments. Front desk staff asked patients whether they would be willing to complete a wellness questionnaire on an iPad at check-in, and questions were answered in the waiting room. Six iPad devices were available to enable multiple patients to complete the questionnaire simultaneously. All encounters in which the IWT was used during this time were included in our study and comprised the “post-IWT” group. Matched comparison patients were selected from the same clinic several months before, forming the “pre-IWT” group. All encounters occurring at this clinic between February and April 2013 were included in the pre-IWT group. Urgent encounters, encounters without a recorded height and weight, and repeat visits during the study period were excluded. To control for temporal changes in the health system, we performed the same analysis at 2 similar clinics that did not use the IWT during either of these time periods (“comparison pre” and “comparison post” groups). Encounters were matched sequentially to the encounters in the post-IWT group using propensity scores. Patient follow-through with selected orders was measured and defined as screening test completion (spirometry, polysomnography) or attendance for at least 1 session with a consultant. All providers at the intervention practice were included and participated in the qualitative interviews.
Data Collection
Patient demographics and order placement were extracted from the electronic medical record (EPIC Systems). Orders included spirometry and polysomnography, consults (smoking cessation, nutrition therapy, psychology, psychiatry, sleep medicine, integrative medicine, lifestyle medicine), online programs available for purchase through the Cleveland Clinic Wellness website (Go! Foods for You, Stress Free Now, Go! To Sleep), and prescriptions (smoking cessation drugs, albuterol, antidepressants, and insomnia drugs). Orders placed within 1 week of the index encounter were included. Medication orders included those for new medications and those changing the dose of an existing medication.
Data from the IWT were stored outside the electronic medical record and collected separately. These included answers to the IWT questionnaires and an ease-of-use survey, as well as whether the provider had marked responses as “reviewed.” Chart reviews were conducted by a single investigator (JF-U) to assess patient follow-through with selected orders.
Provider perceptions were obtained through qualitative semistructured interviews. Interviews were audio-recorded, transcribed, and coded by the interviewer (JF-U).
Data Analysis
Descriptive statistics were used to summarize patient characteristics, and 2-group comparisons were performed using a t test or χ2 test, as appropriate. Comparison groups of patient encounters were matched with those from the experimental group in a 1:1 ratio using propensity scores. Propensity scores were based on age, sex, race, smoking status, and comorbid diagnoses (type 2 diabetes, hypertension, chronic obstructive pulmonary disease, sleep apnea, depression, and cardiovascular disease). The pre-IWT and comparison post groups were each matched to the post-IWT group, and then the comparison pre group was matched to the comparison post group. A χ2 test for proportions or the Fisher exact test (in the case of a small sample size) was used to assess differences in order placement from the before to after periods for all orders in the comparison and IWT groups. Logistic regression was used to adjust the comparisons for patient characteristics that differed between groups after matching. All analyses were conducted using JMP Pro (version 10.0), and statistical significance was established with a 2-sided P value <.05.
Qualitative data were reviewed and coded using NVivo (version 10.1.3) by a single investigator (JF-U) in order to identify emerging themes in an iterative manner. Potential themes and supporting quotations were discussed with a second investigator (MR), who suggested additional classification until consensus was reached. Final themes were shared with 4 of the interviewees, who confirmed their accuracy and that nothing important was missed. Representative quotations were chosen by both investigators to demonstrate themes.
Results
Patient and Provider Characteristics
Five providers (4 physicians and 1 nurse practitioner) participated in 863 patient encounters during the IWT pilot period. They were 48.6 ± 6.6 years old, on average, mostly women (80%), and had spent an average of 19.8 ± 8.8 years in practice. Three providers reviewed >90% of their patients' IWT results, whereas the other 2 providers reviewed these results <50% of the time. The comparison pre (n = 4006), comparison post (n = 5019), and pre-IWT (N = 1065) groups each had 863 encounters after propensity score matching. Patient characteristics are shown in Table 1. A few variables had small but statistically significant differences after matching.
Characteristics of Patients Who Participated in the Integrated Wellness Tool (IWT) Pilot and Matched Comparison Encounters
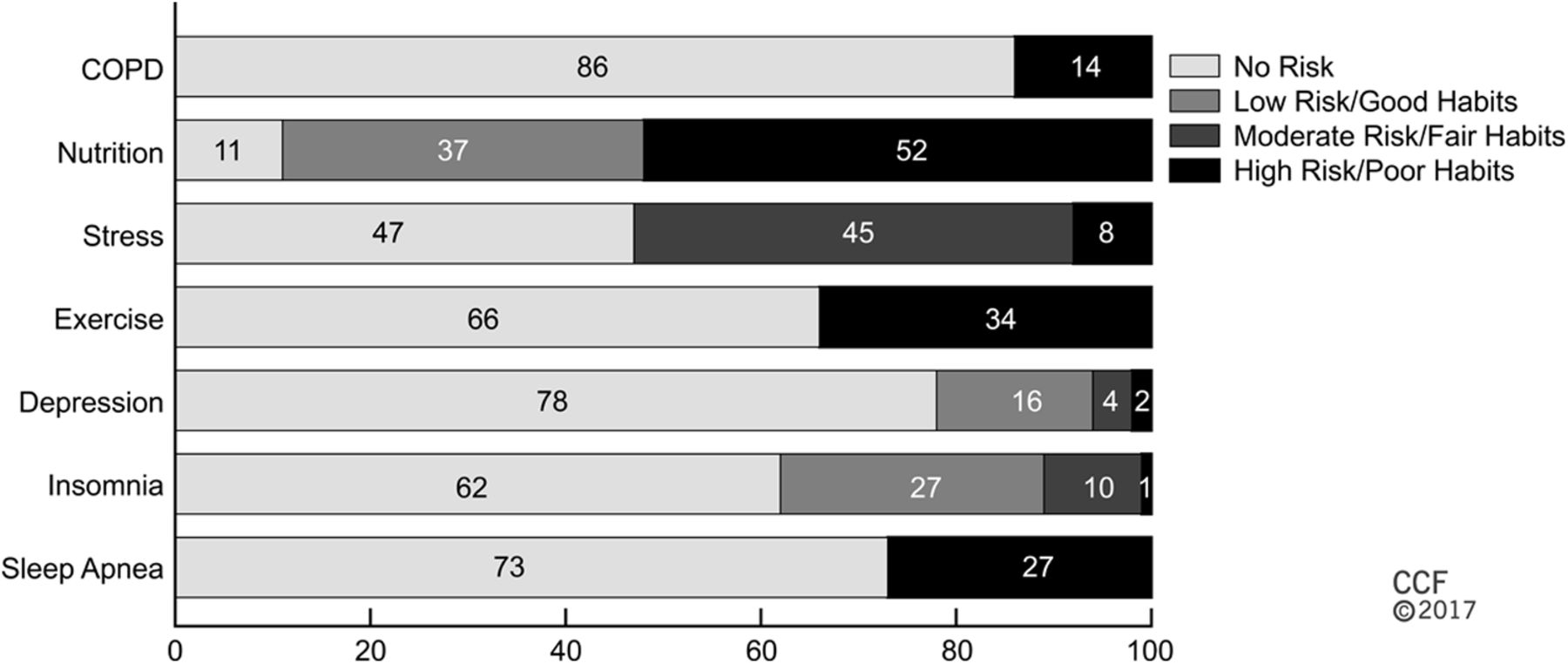
Figure 2 displays patient risk scores by wellness category. Almost all patients (97%) exhibited greater than mild risk in at least 1 category. Nutrition (89%) and stress (53%) represented the areas with the greatest percentage of scores that were “mild risk” or greater.
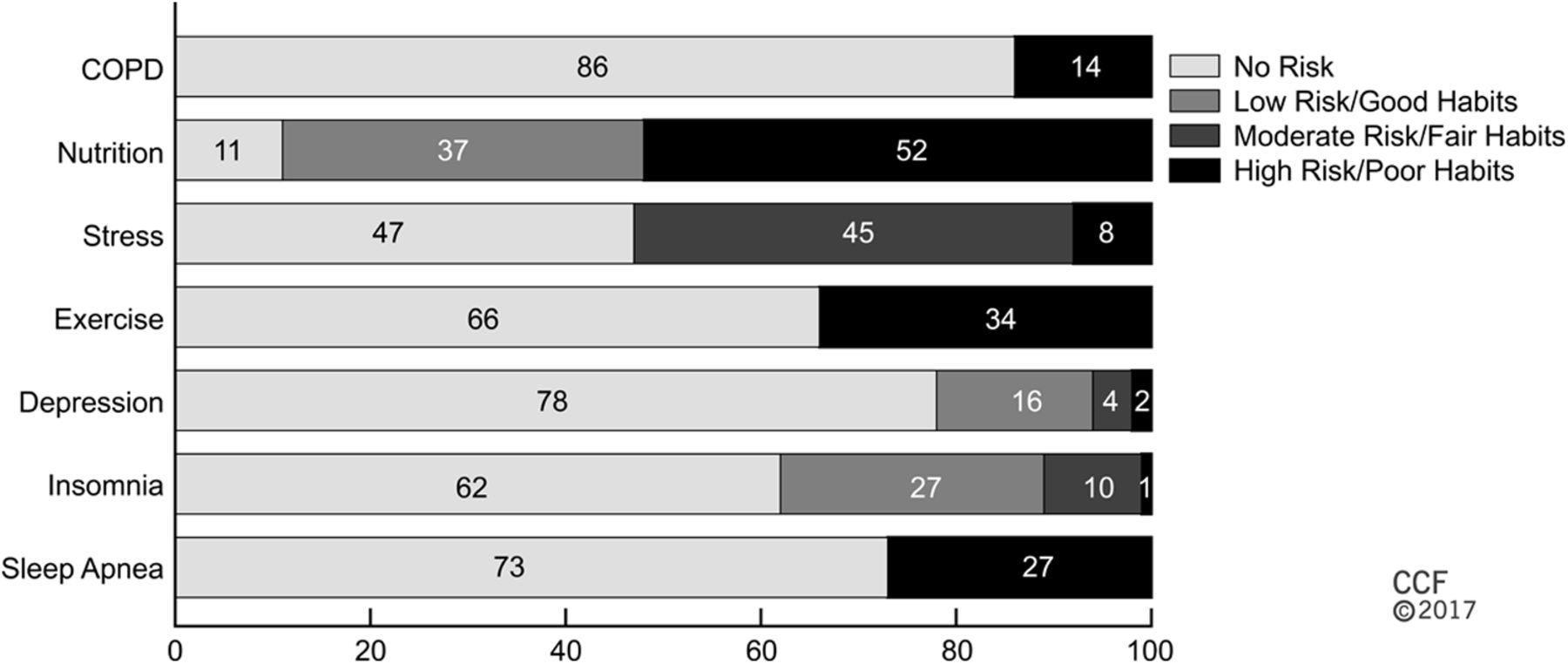
Patient risk by wellness category, captured using the Integrated Wellness Tool (IWT). Risk scores are determined by patient responses to IWT questionnaires during the pilot (June 25 to September 4, 2013). Total responses for the various questionnaires were 702 for chronic obstructive pulmonary disease (COPD), 839 for nutrition, 805 for stress, 825 for exercise, 789 for depression, 734 for insomnia, and 621 for sleep apnea.
Effect on Order Placement
Of 5134 total orders prompted by the IWT based on patients' risk scores in each of the wellness areas, 293 were placed by providers (5.7%). This increased to 7.8% (270/3455) when looking only at risk scores that had been marked as “reviewed” by providers. The specific percentages varied by order (Appendix 2). After implementation of the IWT, the placement of most orders at the intervention site increased—some, such as consult to lifestyle medicine, as much as 5-fold (Table 2). Orders with the greatest increase in placement included polysomnography, consults to Stress Free Now, and spirometry. Orders for albuterol, drugs for smoking cessation, and consults to integrative and behavioral sleep medicine did not increase. None of the target orders in the comparison group sites increased during the study period (Table 2).
Frequency of Order Placement by Primary Care Providers During the Integrated Wellness Tool Pilot and from Matched Comparison Groups
Patient Follow-Through
Patient follow-through was low overall (Table 3). Of the patients who completed spirometry, 28% had abnormal results. All patients who underwent polysomnography had an abnormal result.
Order Placement and Follow-Through for Patients with Elevated Integrated Wellness Tool Risk Scores, By Wellness Area
Patient Perceptions
Of 699 patients who completed the ease-of-use survey, almost all patients found the IWT easy to use (n = 688 [99%]), did not require help (n = 668 [96%]), and stated that they would use the tool again (n = 658 [94%]). Similar observations were made by patients >80 years of age (n = 56). Most patients (n = 645 [92%]) indicated that the IWT would help their provider understand their current state of health to some extent.
Qualitative Assessment
Providers generally perceived wellness as important to their role in primary care. One stated “We think of ourselves as specializing in [wellness].” Before the IWT, providers used a variety of methods to assess and document wellness behaviors, and were confident in their abilities to address wellness. Though curious to see patients' reactions to the tool, providers had concerns about changing their routine, learning new technology, and increased demands on their time with the IWT.
Providers also found the IWT easy to use: “It was actually very simple to use. I had no trouble with it at all.” Providers were not surprised by their patients' risk scores, stating that the IWT “did not provide any new information.” They found the tool most useful for new patient encounters and physical exams. Providers found that the IWT generated more discussion and increased patients' involvement in their care. One provider reflected on the utility of the IWT data in addressing chronic pain and fatigue:
There's been several patient encounters where patients come in with chronic pain, chronic fatigue complaints, and their depression scores are high, their stress scores are high, and it's actually given me some objective data to turn the computer screen to them and say hey, do you think this might be contributing? So that is what I found really useful and I did not anticipate that that was going to be the case. It actually makes it easier to address what the real issues are. That way we do not have to do 10 more tests to figure out the chronic fatigue.
Providers reflected that discussing wellness required time. However, in some situations such as screening, providers found the IWT to streamline the ordering process: “For the [chronic obstructive pulmonary disease] ones that actually the screen was positive for, and I was able to order the [pulmonary function test]s … all in 1 click …. That was really helpful.”
Overall, providers did not recognize much patient follow-through with lifestyle recommendations after using the IWT: “I did not find that it changed behavior.” Because of this, they did not perceive the tool to have improved their ability to care for patients: “Personally I do not think it really enhances how I take care of them, but maybe their buy-in to wellness is enhanced with that exercise. I think that is the best aspect of it.”
Discussion
This mixed-methods retrospective cohort study of 863 patient encounters conducted by 5 providers using the IWT demonstrated that patients are willing to enter personal wellness data using standardized electronic questionnaires, and these data can influence providers' preventive care ordering patterns.
The feasibility of collecting patient-entered health data, including family history18 and lifestyle behaviors,19⇓⇓–22 in preparation for an annual wellness examination has been well documented. One study in a primary care setting found that patients were willing to complete questionnaires on mobile devices in the waiting room and this did not affect workflow.21 Although our study did not investigate the IWT's impact on workflow, patients and providers alike reported that it was easy to use.
Electronic reminders have shown promise for changing physician behavior.23 Point-of-care reminder systems generally improve adherence to processes of care by a small amount (median increase of 4%).24 Larger effects (median increase of 12%) have been noted for preventive care reminders.25,26 “Homegrown” clinical information systems have shown the largest improvements (median increase of 17%), perhaps because they are better integrated into providers' workflow.24 We saw modest increases in the rate of provider order placement (1.2%, on average); however, the majority of interventions tested here were lifestyle interventions rather than standard-of-care screening tests. Referrals to consults such as psychology and psychiatry may have been low because of the limited availability of these resources within our health care system. Orders for screening tests showed larger increases (4.2% for spirometry and 5.0% for polysomnography).
Interestingly, although providers in our study expressed that the IWT did not provide any “new information” or enhance the care they provided, they consistently placed more preventive care orders when using the tool. This behavior might be attributed to new information presented to the provider, or simply to reminding the provider of the condition when it came time to place orders. Of particular interest is the almost 400% increase in consults to smoking cessation with the IWT. Although smoking status was already documented in the electronic medical record and providers were presumably aware of it, they ordered fewer consults for tobacco treatment programs before the IWT.
Few studies have integrated the collection of patient-entered data with provider reminders to improve recommendations for, discussions of, and actual preventive care delivery and patient behavior change. One study conducted in New Zealand demonstrated the feasibility of an electronic lifestyle assessment tool similar to the IWT.22 While the results of that assessment may be downloaded from a website to the electronic medical record by the provider, they do not drive automatic order prompts, thus increasing the steps required to implement a relevant care plan. Despite this difference, most patients in that study found the tool easy to use, and feedback from providers was positive.
The IWT differs from other health risk assessments in that it is focused on lifestyle information (as opposed to recommended screening), and it is generally physician-facing, meaning patients have few opportunities to interact or engage with their lifestyle data. A 5-level model for making information technology patient-centered27 proposes that an electronic tool must (1) collect patient-entered information, (2) integrate this information with existing clinical information, (3) interpret information for patients through a user-friendly interface, (4) provide individualized recommendations to patients based on risk profile and evidence-based guidelines, and (5) facilitate patient activation and engagement. While the IWT does provide individualized recommendations, it does so through the provider.
An alternative tool, MyPreventiveCare, which contains all the above-mentioned components, has been shown to improve preventive care delivery in an 8-practice pilot and is currently under investigation in a large clinical trial.28,29 Like other health risk assessments, MyPreventiveCare is focused on screening tests and immunizations rather than on lifestyle interventions.30,31 Allowing patients to access and interact directly with the IWT data may help to improve patient activation, leading to increased follow-through with orders and long-term lifestyle behavior change.
Interestingly, providers were more likely to recommend and patients more likely to complete recommended screening tests than lifestyle interventions. The reasons for this are unknown. It may relate to the 1-time nature of screening tests, or a belief that these interventions are more evidence-based or more likely to succeed.
The IWT incorporates several domains that have not previously been included in risk assessment tools. Both stress and sleep have a strong effect on health,32⇓–34 yet they are rarely addressed in the primary care setting in an actionable way.36 Nutrition and physical activity are also important contributors to health, yet standard screening methods (other than body mass index) are not routinely recommended.36 Depression screening has been covered by Medicare since 2011 and is recommended for all adults in settings with effective follow-up supports.37 The IWT provides a systematic way to implement screening in all these areas and track changes in patients over time.
Our study has limitations. Although we examined a large number of encounters, our pilot included only 5 providers, limiting the conclusions we may draw from their ordering patterns and qualitative feedback. It seems that 3 of the 5 providers were more engaged than the other 2 in using the IWT based on the rate at which IWT results were marked as “reviewed.” No differences in age, sex, years in practice, or qualitative themes were found between these 2 provider groups; however, 1 of the “less engaged” providers mentioned that she often did not know whether a patient had completed the IWT. This may further limit conclusions that may be drawn. This study focused on only preventive care delivery. Neither the appropriateness of this care, patient behavior change, nor change in health outcomes were assessed. In addition, we only measured preventive care delivery in the form of consults, screening tests, and treatments ordered. Changes in behavioral counseling may have occurred but were not measurable.
Conclusion
This pilot study demonstrates that an electronic tool can be used to routinely collect patient- entered lifestyle data, and that these data can provide meaningful decision support to increase the delivery of preventive care. Future versions should include a patient portal allowing patients to interact with their results and providing educational information. This might increase patient activation and improve follow-through with providers' recommendations. In addition, subsequent studies should investigate the long-term effect of such tools on patients' behaviors and health outcomes.
Acknowledgments
The authors thank MaryBeth Mercer, MPH, for her guidance during the qualitative portion of this study, and William Morris, MD, and the Cleveland Clinic Clinical Solutions Center for developing and allowing us to study the Integrated Wellness Tool.
Appendix 1
Nutrition Questionnaire
Nutrition Questionnaire
Appendix 2
Placement of Orders Recommended by the Integrated Wellness Tool, by Reviewed Status
Placement of Orders Recommended by the Integrated Wellness Tool, by Reviewed Status
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: none declared.
To see this article online, please go to: http://jabfm.org/content/30/3/350.full.
- Received for publication July 19, 2016.
- Revision received December 21, 2016.
- Accepted for publication January 23, 2017.




{kind=link}
{kind=link}