
Abstract
Background: We previously found that an intervention involving electronic algorithms to detect delays in follow-up of cancer-related abnormal or “red-flag” findings and communicating this information to primary care providers (PCPs) led to more timely diagnostic evaluation. In this study, we examined the effectiveness of various communication strategies to inform PCPs about the delayed follow-up.
Methods: After identifying follow-up delays through electronic health record–based algorithms and record reviews, we communicated this information to PCPs using 3 escalating steps. First, we sent secure E-mails. If no evidence of follow-up was found in a medical record review after 1 week, we made up to 3 attempts to reach the PCPs or their nurses via telephone. If they could not be reached, we informed clinic directors as the third and final step. In this analysis, we evaluate PCPs' follow-up in response to these methods of communication.
Results: A total of 733 patients with follow-up delays were identified (369 patients in the intervention group and 364 patients in the control group). Communicating information to PCPs about possible follow-up delays led to decreased times to diagnostic evaluation, but communication related to delays did not always lead to follow-up for the patients in the intervention group. Specifically, secure E-mails led to follow-up in 11.1% of cases (41 of 369), telephone calls led to follow-up in 68.6% of cases (225 of 328), and contacting clinic directors led to follow-up in 5 of 11 cases in which communication escalated to this level.
Conclusion: Strategies to communicate to PCPs information on delayed follow-up of findings suspicious for cancer were useful, but not fail-safe. Additional back-up strategies, such as using case coordinators, might be needed.
- Algorithms
- Ambulatory Care Facilities
- Communication
- Control Groups
- Electronic Health Records
- Electronic Mail
- Follow-Up Studies
- Humans
- Neoplasms
- Primary Care Providers
- Telephone
Failure to follow-up abnormal or “red-flag” clinical findings (test results, signs, and symptoms) can lead to delays in diagnostic evaluation and poor clinical outcomes.1⇓⇓–4 To our knowledge, no studies have explored how to effectively communicate information about these delays, once identified, to frontline providers in near real time.
In a recent randomized control trial (RCT), we found that an intervention using electronic algorithms to find delays in follow-up of cancer-related “red-flag” findings and communicating this information to primary care providers (PCPs) led to more timely diagnostic evaluation.5 The communication strategy involved escalating steps, progressing from sending secure E-mails to making telephone calls to informing clinic directors if phone calls did not result in successful contact. In this analysis, we examine the effectiveness of these communication strategies to understand each method's effect on PCP responsiveness to communication. The knowledge gained could inform future interventions to prompt provider follow-up when such follow-up is needed.
Methods
Participants
In the RCT, 72 PCPs (physicians, physician assistants, and nurse practitioners) from 2 sites (a large, urban Veterans Affairs facility and a private health system) were recruited and randomly assigned to each of the control (usual care) and intervention groups in equal number. Electronic algorithms designed to identify patients with potential delays in diagnostic evaluation for lung, colorectal, or prostate cancer were applied to the electronic health records (EHRs) of all patients seen by these PCPs from April 20, 2011, to July 19, 2012 (approximately 118,400 unique patients). Algorithms included “red-flag” findings to identify patients with possible cancer, clinical exclusion criteria to eliminate patients for whom further evaluation was not warranted, and expected follow-up criteria to eliminate patients who already had follow-up (see Table 1; additional details are described elsewhere2,5,6). The electronic algorithms identified 1,256 patients with possible delays in diagnostic evaluation. Manual chart review (which was done to verify that follow-up was not missed by the algorithm) indicated that 749 indeed needed follow-up. Excluding 16 patients whose providers left during the intervention, this left 733 patients (364 patients in the control group and 369 patients in the intervention group). The intervention group of 369 patients is the focus of this additional analysis. Institutional review boards at both sites approved the study, with waivers for patient consent. Written consent was obtained from providers upon enrollment in the study.
“Red-Flag,” Clinical Exclusion, and Expected Follow-up Criteria by Cancer Type Used in Electronic Algorithms Applied to the Electronic Health Records of 118,400 Patients from April 20, 2011, to July 19, 2012
Procedure
Upon recruitment for the RCT, PCPs specified communication preferences, including preferred E-mail addresses/telephone numbers, times of day to call, and whether telephone calls should be made to PCPs or their nurses. After confirming delays, we communicated the information to PCPs via secure E-mail. This communication included the patient's name, medical record number, test name, and test date. The goal of the communication was to convey that a patient might be experiencing a delay in follow-up for a diagnostic evaluation. If the PCP did not follow-up within 1 week, we made up to 3 telephone calls containing the same information that was conveyed in the secure E-mail to PCPs or their nurses. Follow-up was defined as following through with appropriate diagnostic evaluation or documenting intentionally delayed follow-up (eg, documenting watchful waiting of elevated prostate-specific antigen). Lastly, if no one could be reached, we informed clinic directors. Final patient outcomes regarding follow-up and the presence of cancer were assessed by chart review 7 months after the initial “red-flag” findings.
Analyses
In this analysis, we descriptively examined PCP follow-up to each communication method for the 369 cases of delayed diagnostic evaluation in the intervention group. In addition, χ2 analyses compared follow-up resulting from contact with a PCP versus a nurse for telephone calls and for each communication method by site.
Results
Brief Summary of the RCT
For the 733 patients identified as having delays in diagnostic evaluation in the RCT, times to diagnostic evaluation were significantly shorter for patients in the intervention group than they were for patients in the control group identified by the colorectal cancer algorithm (median, 104 vs 200 days, respectively; n = 557; P < .001) and the prostate cancer algorithm (40% received evaluation at 144 vs 192 days, respectively; n = 157; P < .001), but not the lung cancer algorithm (median, 65 vs 93 days, respectively; n = 19; P = .59).5 More intervention patients than control patients received diagnostic evaluation by final review (73.4% vs 52.2%, respectively; relative risk, 1.41; 95% confidence interval, 1.25–1.58). Lastly, cancer diagnoses were confirmed in 23 patients during the 7-month follow-up period (10 in the control group and 13 in the intervention group; P = .66). Additional results have been described previously.5
Follow-up Resulting from Intervention Communication
Communicating information to PCPs about possible delays in diagnostic evaluation did not always result in follow-up (see Figure 1). Specifically, secure E-mails led to follow-up in 11.1% of cases (41 of 369). Telephone calls led to follow-up in 68.6% of cases where this escalation occurred (225 of 328) or in 71.0% of cases in which a provider could be reached (225 of 317). Lastly, contacting clinic directors led to follow-up in 5 of the 11 cases where communication escalated to the highest level. Cumulatively, this led to 11.1%, 72.1%, and 73.4% response rates for the various communication attempts. Whether PCPs or nurses were the designated telephone call recipients made no difference in resultant follow-up (P = .82): calling PCPs led to follow-up in 67.9% of cases (133 of 223) and calling nurses led to follow-up in 69.7% of cases (92 of 146). However, PCPs at the Veterans Affairs facility followed up in response to 73.6% of telephone calls (204 of 277), whereas PCPs at the private health system followed up in response to fewer calls (52.5%; 21 of 40; P = .006). Follow-up after secure E-mails, however, was comparable across sites: PCPs at the Veterans Affairs facility followed up in response to 11.4% of E-mails (37 of 324) and PCPs at the private health system followed up in response to 8.9% of E-mails (4 of 45; P = .61).
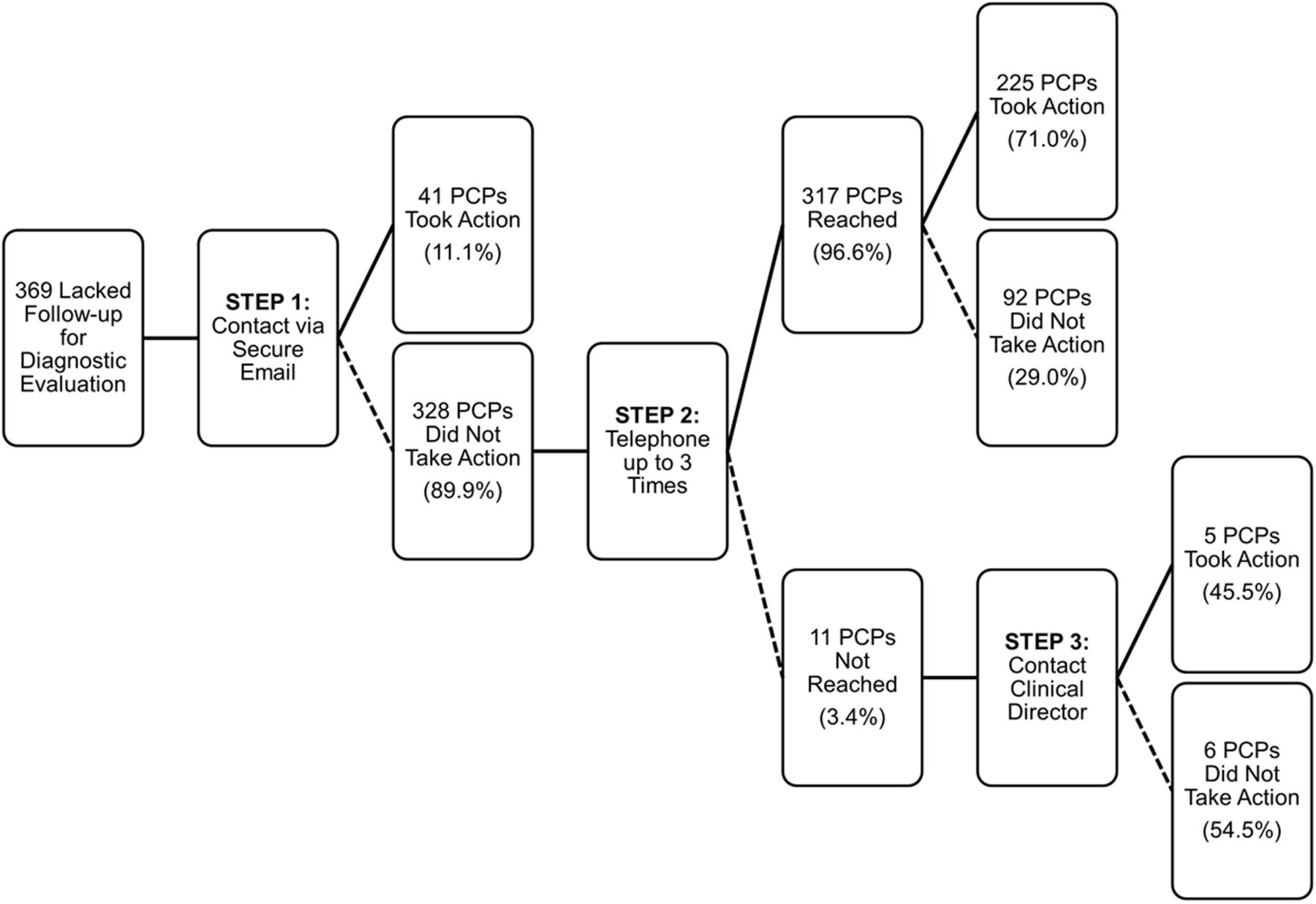
Diagram of primary care provider (PCP) follow-up by type of communication. Percentages total 100 at each branching point.
Discussion
With increasing EHR adoption, it is essential to leverage the wealth of EHR data and bring it to the point of care to improve health care quality. However, communicating information to PCPs about possible delays in diagnostic evaluation has not been studied thus far and it must fit within PCPs' workflow to be effective. We found that secure E-mails lead to follow-up actions in only a small percentage of cases, and additional strategies such as telephone calls and contacting clinic directors had only moderate effects on follow-up. Given the relatively modest effect of these strategies for communicating diagnostic delays, the potential of such interventions is likely to be significantly dampened. Our findings highlight the complexity of communicating important information to providers to improve patient care in near real time.
We also found that delivering the information to nurses was as effective as delivering it directly to PCPs, suggesting that team-based approaches to communication may be feasible and may avoid contributing to the “information overload” PCPs already experience.7⇓⇓–10 With increasing use of EHRs by PCPs to provide care,11 electronic data capturing clinical practice and quality of care have proliferated, allowing interventions that leverage these data to be developed and used to improve patient care at the point of care.12,13 However, implementation of such interventions faces many challenges, such as the need for resources to develop and implement algorithms to extract EHR data and administrative or clinical personnel to deliver it to the point of care.6 Additional research is needed to ensure such interventions are translated successfully into practice.14 Back-up strategies using organizational mechanisms (such as case coordinators) could also be considered to support PCPs in tracking and follow-up.
There are several limitations to this study. While communicated information was not always acted on, we did not obtain direct feedback from PCPs as to why. Thus, we were unable to determine reasons for delays in follow-up despite being notified (unless documented in the medical record). Future qualitative research on this topic should investigate these reasons in detail to help develop better implementation strategies. In addition, the work was not designed to test improvements in health outcomes, which would require much longer follow-up of patients and a much larger sample. Despite these limitations, this is the first examination of methods to communicate potential delays in diagnostic evaluation to frontline providers. Understanding the impact of communicating information to minimize care delays, however, is an important step in ultimately getting patients better care and improving health outcomes.
Conclusion
To leverage the wealth of EHR data and bring it to the point of care to improve health care quality, more robust strategies for communicating information on follow-up delays are needed. Future research in primary care should focus on how to ensure these strategies fit within the workflow of PCPs. In addition, back-up strategies using organizational mechanisms (such as case coordinators) could also be considered to support PCPs in tracking and follow-up.
Acknowledgments
The authors acknowledge Louis Wu, Eric J. Thomas, and Samuel N. Forjuoh, who played critical roles in the primary study that this report came from. Without their help on the initial study, this additional analysis would not have been possible.
Notes
This article was externally peer reviewed.
Funding: This work was supported by the Agency for Health Care Research and Quality (grant no. R18HS017820) and the Houston Veterans Affairs Health Services Research & Development Center for Innovations in Quality, Effectiveness and Safety (CIN 13–413). DRM is supported by a Mentored Career Development Award (grant K08-HS022901) from the Agency for Healthcare Research and Quality. HS is also supported by the VA Health Services Research and Development Service (CRE 12–033; Presidential Early Career Award for Scientists and Engineers USA 14–274), the VA National Center for Patient Safety, and the Agency for Health Care Research and Quality (grant R01HS022087).
Conflict of interest: none declared.
Disclaimer: The views expressed in this article are those of the authors and do not necessarily represent the views of the Department of Veterans Affairs or any other funding agency.
- Received for publication November 23, 2015.
- Revision received March 28, 2016.
- Accepted for publication April 18, 2016.




{kind=link}