
Abstract
Although it is known that the social determinants of health have a larger influence on health outcomes than health care, there currently is no structured way for primary care providers to identify and address nonmedical social needs experienced by patients seen in a clinic setting. We developed and piloted WellRx, an 11-question instrument used to screen 3048 patients for social determinants in 3 family medicine clinics over a 90-day period. Results showed that 46% of patients screened positive for at least 1 area of social need, and 63% of those had multiple needs. Most of these needs were previously unknown to the clinicians. Medical assistants and community health workers then offered to connect patients with appropriate services and resources to address the identified needs. The WellRx pilot demonstrated that it is feasible for a clinic to implement such an assessment system, that the assessment can reveal important information, and that having information about patients' social needs improves provider ease of practice. Demonstrated feasibility and favorable outcomes led to institutionalization of the WellRx process at a university teaching hospital and influenced the state department of health to require managed care organizations to have community health workers available to care for Medicaid patients.
Physicians recognize that a patient's socioeconomic circumstances have a significant effect on health.1 As highlighted in the 2011 report “Health Care's Blind Side,” 4 of every 5 primary care physicians (among 1000 surveyed) said that social needs are as important to address as medical conditions, that they do not feel confident in their ability to address those needs, and that by not addressing them, their patients' health suffers.2
The inability to take action on unmet social needs can be demoralizing for primary care providers who already feel overburdened by treating complex medical needs, complying with new documentation requirements, and confronting pressing time demands. Yet we know that patients, especially those from communities with high rates of poverty, experience significant nonmedical socioeconomic challenges that negatively affect their health.3,4 Primary care providers experience a sinking feeling when after the clinical encounter, their hand on the doorknob to leave the examination room, their patient adds 1 more reason for the visit—perhaps they lost their job, are unable to afford their medicine, or are about to be evicted from their home.
Screening for social needs has proven valuable for certain age groups: children during well-child visits,5 patients with chronic habits such as smoking,6 and high-risk patients with complex chronic diseases.7 The WellRx pilot cast a wider net, evaluating the feasibility of systematically screening for and addressing patients' social needs during every visit in busy general primary care settings.
Methods
Institutional review board approval was obtained to conduct a 90-day feasibility study with providers in 3 family medicine clinics in Albuquerque, New Mexico—2 run by a public university teaching hospital and 1 by a federally qualified community health center. Each of the clinics serves a large, low-income population. With funding from the Blue Cross/Blue Shield Community Grant program, researchers in the Office for Community Health at the University of New Mexico convened providers and community health workers (CHWs) from the 3 clinics to identify the domains of greatest social need experienced by the patients they serve. Eleven were identified: food insecurity, housing, utilities, income, employment, transportation, education, substance abuse, child care, safety, and abuse. The domains were incorporated into a pretested, 11-item questionnaire (available in English or Spanish). A literacy specialist from a university hospital ensured that the questions conformed to “low literacy” (Appendix). Our objectives were to obtain concrete data on the level of patient need, to test different methods of administering the screening tool, and to identify the best approach to connecting patients to needed resources and services.
An attempt was made to screen all patients, either by self-administered questionnaires distributed by front desk staff or by medical assistants (MAs) while recording vital signs. Sites that chose to have MAs administer the surveys were concerned that literacy issues would cause patients, especially those most in need, to decline to complete them. Patients' responses on hard-copy questionnaires were gathered and tabulated. Five members of the research team—1 family medicine faculty member (WK) and 4 family medicine residents (KM, JN, VI, DI)—were providers at the participating clinic sites. As “participant-observers,” they kept journals of their experience with implementing WellRx. Other members of the team (JP, MB) trained clinic staff, gathered data on operational experiences during implementation of WellRx, and documented the role of CHWs in this process. CHWs had extensive experience working in different capacities in their communities. They were trained by the Office for Community Health Workers in a 1-week intensive orientation that provided skills in working within the clinic system, including accessing electronic medical records. All received extensive training in accessing and connecting patients to community resources.
Results
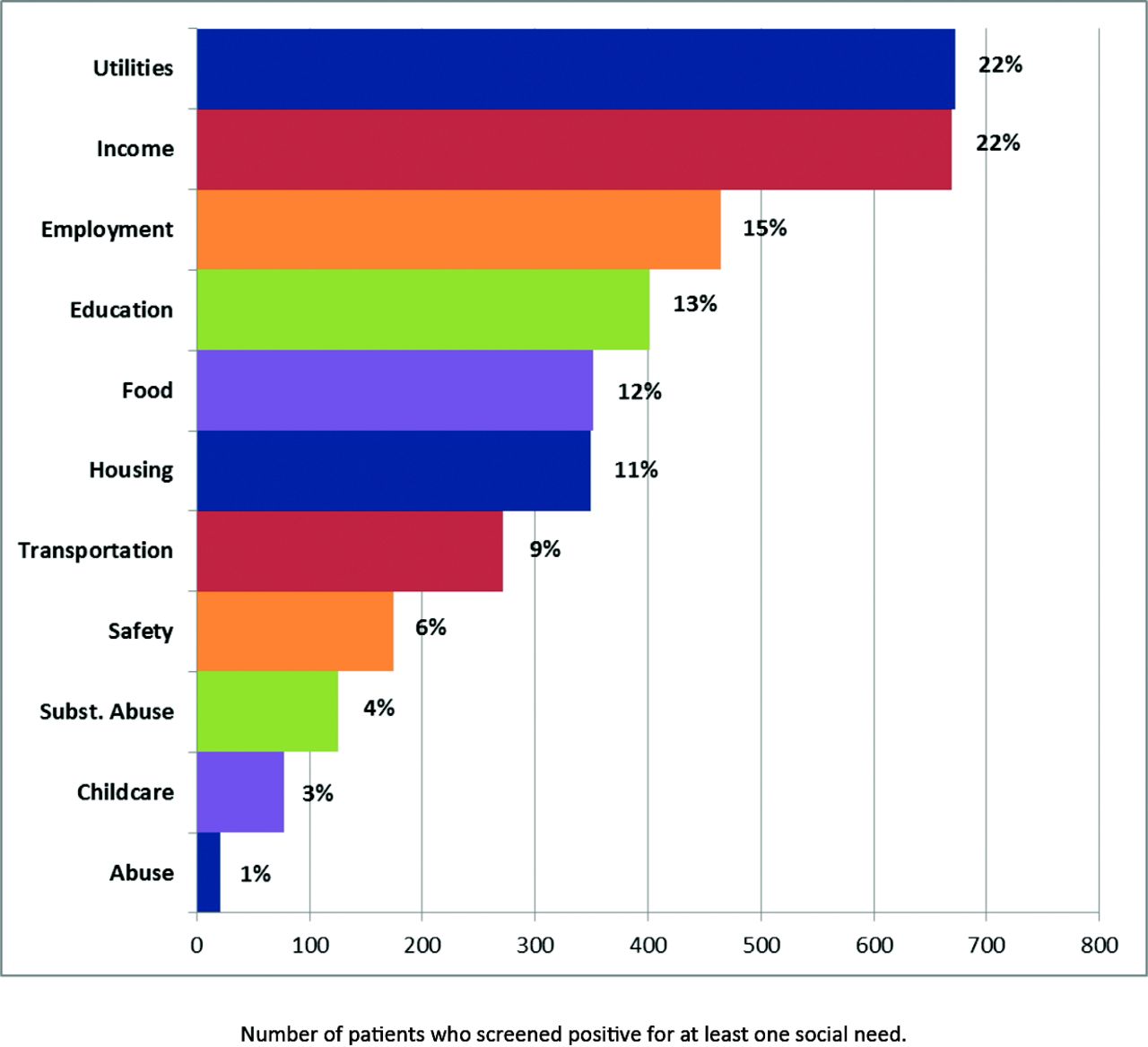
WellRx questionnaires were completed by 3048 patients over the course of the 90-day pilot. MAs' face-to-face-administration of the questionnaire yielded the highest percentage of patients reporting adverse social determinants. A total of 2038 questionnaires were completed by the MAs and 1110 were completed by self-administration. Of those surveyed, 46% (n = 1413) reported at least 1 social need. Of those reporting a social need, 63% (n = 890) indicated multiple needs. Needs most often indicated concerned utilities, income, employment, and education (Figure 1). Previously unknown patient needs were identified and addressed. Patients who screened positive for unmet social needs were offered assistance in connecting with appropriate services and resources. MAs became resources to patients by handing out resource sheets to address identified social needs, resulting in a significant enhanced role for MAs. The role of MAs in identifying social problems and CHWs in intervention led providers to feel that their workloads had lightened, leading to a greater ease of practice and greater confidence that their patients were receiving quality care. In the clinic with CHWs, patients reporting social needs were referred to a CHW. Services offered by CHWs included helping patients to access resources like food banks and to fill out job applications, accompanying patients to apply for food stamps, conducting home visits, or arranging family meetings with the health care team. A patient's level of need dictated the intensity and duration of the CHW's interaction with that patient—usually 1 contact a month and usually for <3 months. Using WellRx greatly accelerated the integration of CHWs into primary care teams. None of the sites reported negative effects on efficiency created by use of the WellRx tool.

Nonmedical needs identified during the WellRx pilot.
Feasibility of the pilot informed key policy decisions by the university teaching hospital, the state department of health, and 2 of the 4 managed care organizations that administer Medicaid programs in New Mexico. The university hospital has now institutionalized the WellRx by requiring that all patients in its 7 primary care clinics be screened for social needs and that those needs be addressed by CHWs newly hired for each clinic. All primary care residents now train at a site with this expanded model of care whereby social determinants are not only identified but also addressed.
Discussion
The WellRx Pilot revealed important insights for primary care practice.
Concrete Documentation of Patient Needs
The WellRx screening process produced concrete data about the magnitude of social needs in primary care patients' lives, resulting in better-informed clinic providers and staff, who are now able to develop more effective intervention and management plans.
Effect of WellRx on Residents and Faculty
WellRx provided an innovative vehicle for training. Residents learned practical skills for engaging patients in discussions that would not normally surface during clinic visits.8 Primary care physicians were initially skeptical about the value of the pilot to patient care, but residents who took part in the pilot became its strongest advocates, teaching attending physicians who were not participating in the pilot about the importance of screening for social needs. At 1 site, 7 providers who were not involved in the WellRx pilot were so impressed by what the residents had been teaching them that they decided to start using WellRx as their diabetes control quality improvement project, and they began referring appropriate patients in this select population to CHWs for action on social needs.
CHWs as Crucial Members of the Primary Care Team
The WellRx pilot revealed the important role CHWs can play in a primary care clinic. The University of New Mexico Office for Community Health has many years of experience in training and deploying CHWs to help address the social needs of high-cost/high-risk patients enrolled in Medicaid managed care.9 But these CHWs have always worked in the community, with little linkage to the primary care clinics to which Medicaid enrollees are assigned. CHWs have key skills for helping patients navigate external bureaucracies; they provide assistance with complicated application processes and even accompany patients who lack the skills to do so on their own to apply for benefits. The CHWs complement and extend the reach of the clinic-based social worker through home visits and visits to community sites.
WellRx as a Trigger for Broader Institutional Transformation
Providers often believe that screening for patients' nonmedical social needs is not feasible in a clinic setting in terms of time and the ability to provide assistance. In addition, these needs are not generally considered to be within the purview of the medical system. The WellRx pilot demonstrated that it is feasible for a clinic to screen and address patients' social needs on site, without disrupting clinic flow and while actually improving provider ease of practice and enhancing staff roles. Because the WellRx pilot was incorporated into some of the busiest and most visible family medicine clinics within a university health system, word of its positive outcomes on clinic practice spread rapidly and influenced the university hospital administration to hire CHWs and incorporate the screening tool into all primary care clinics.
Innovative Clinic Improvement Pilot Can Affect State Policy
In March 2014 the governor of New Mexico signed into law the Community Health Workers Act, which paved the way for a certification process for CHWs in New Mexico and included the possibility of Medicaid reimbursement for certified CHW services. But few models existed in which CHWs were fully integrated into primary care practices. The success of the WellRx pilot laid the groundwork for a larger study involving a collaboration between state Medicaid managed care, the university, Molina Health Care of New Mexico, Blue Cross Blue Shield of New Mexico, and 2 federally qualified health centers—Hidalgo Medical Services and First Choice Community Healthcare. That study is evaluating screening for social needs and addressing those needs through CHWs integrated into primary care clinics by determining their impact on care quality and cost for 10,000 Medicaid enrollees, including both healthy and very ill patients.
Acknowledgments
The authors acknowledge the numerous individuals who assisted with implementation of the pilot, including physicians, residents, physician assistants, medical assistants, nurses, receptionists, clinic coordinators, and clinic directors at all the sites for participating in the project.
Appendix
WellRx Questionnaire
DOB__________________ Male___ Female _____
WellRx Questions
Notes
This article was externally peer reviewed.
Funding: Development of the WellRx Toolkit was supported with a grant from the Blue Cross/Blue Shield Community Grant Program.
Conflict of interest: WK, JN, KM, VI, and DI are practicing physicians at clinics where the pilot was implemented. Each of them served as “participant-observers” of the process and recorded thoughts and notes for research according to an institutional review board–approved protocol.
- Received for publication August 26, 2015.
- Revision received November 16, 2015.
- Accepted for publication November 17, 2015.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Families Perspectives on Social Services Navigation After Pediatric Urgent Care
- Assessing Implementation of Social Screening Within US Health Care Settings: A Systematic Scoping Review
- Patients Willingness to Accept Social Needs Navigation After In-Person versus Remote Screening
- Patients Willingness to Accept Social Needs Navigation After In-Person versus Remote Screening
- Patient Barriers to Accessing Referred Resources for Unmet Social Needs
- Routinely asking patients about income in primary care: a mixed-methods study
- Content Analysis of Transportation Screening Questions in Social Risk Assessment Tools: Are We Capturing Transportation Insecurity?
- Knowledge, Attitude, and Practices of Health Professionals Working in A Major Health Care System Regarding Social Determinants of Health (SDOH) and Community Health Workers (CHWs)
- Utilization Patterns of a Food Referral Program: Findings from the Mid-Ohio Farmacy
- Provider Impacts of Socioeconomic Risk Screening and Referral Programs: A Scoping Review
- Adults with Housing Insecurity Have Worse Access to Primary and Preventive Care
- Advancing Social Prescribing with Implementation Science
- Association of the Social Determinants of Health With Quality of Primary Care
- Clinician Experiences with Screening for Social Needs in Primary Care
- Roles and Functions of Community Health Workers in Primary Care
- Reducing Social Distress for Chronic Disease Patients in Primary Care: An Intervention for Latino Type 2 Diabetes Patients Seen at Community Health Centers
- Agriculture and Health Sectors Collaborate in Addressing Population Health
- Housing, Transportation, And Food: How ACOs Seek To Improve Population Health By Addressing Nonmedical Needs Of Patients
- CommunityRx: A Population Health Improvement Innovation That Connects Clinics To Communities
- Social Determinants of Health and Primary Care: Intentionality Is Key to the Data We Collect and the Interventions We Pursue