
Abstract
Background: Change champions are important for moving new innovations through the phases of initiation, development, and implementation. Although research attributes positive health care changes to the help of champions, little work provides details about the champion role.
Methods: Using a combination of immersion/crystallization and matrix techniques, we analyzed qualitative data, which included field notes of team meetings, interviews, and transcripts of facilitator meetings, from a sample of 8 practices.
Results: Our analysis yielded insights into the value of having 2 discrete types of change champions: (1) those associated with a specific project (project champions) and (2) those leading change for entire organizations (organizational change champions). Relative to other practices under study, those that had both types of champions who complemented each other were best able to implement and sustain diabetes care processes. We provide insights into the emergence and development of these champion types, as well as key qualities necessary for effective championing.
Conclusions: Practice transformation requires a sustained improvement effort that is guided by a larger vision and commitment and assures that individual changes fit together into a meaningful whole. Change champions—both project and organizational change champions—are critical players in supporting both innovation-specific and transformative change efforts.
- Diabetes Mellitus
- Practice-based Research
- Practice-based Research Networks
- Primary Health Care
- Quality Improvement
The use of change champions to implement new innovations in organizations spans nearly 5 decades.1 There is considerable evidence from multiple disciplines pointing to the importance of champions for moving new innovations through the phases of initiation, development, and implementation.2⇓⇓⇓⇓–7
Current conceptions of champions include several core behaviors such as (1) actively and enthusiastically promoting a new innovation,8,9 (2) making connections between different people in the organization,10 (3) mobilizing resources,11,12 (4) navigating the sociopolitical environment inside the organization,3 (5) building support for the innovation by expressing a compelling vision and boosting organizational members' skills and confidence,11 and (6) ensuring that the innovation is implemented in the face of organizational inertia or resistance.1,3,5,6,9
The value of champions is particularly apparent for health care changes, as evidenced by the sheer number of articles that mention the use of a champion.13⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓–27 Most of this literature, however, presents positive findings associated with a champion without clearly defining or describing the champion role.2,28⇓⇓⇓⇓⇓⇓–35 Too often, little or no information is provided about how the champion(s) came to be, what they actually did in this capacity, or how the role may have evolved over time. One of the dangers of not providing sufficient detail about the champion role is that it encourages an assumption that champions have standard behaviors and characteristics and therefore discourages a critical examination of variables that may be important for organizational change efforts.
With pronounced attempts to produce transformational change in the US health care system, the presence of a champion may be an important driving force behind the implementation of a wide range of change initiatives in health care settings.36 However, meaningful health care system redesign could be more effective with a clearer understanding of the champion role and an evidence base for incorporating champions into appropriate intervention strategies.
In this article, we present a qualitative analysis of a quality improvement (QI) trial called Enhancing Practice, Improving Care (EPIC), which was aimed at improving diabetes and depression care in primary care practices. The intervention design included a series of team-based meetings with an external facilitator and learning sessions. Moreover, it was intended for facilitators to work closely with a change champion in each practice who would be the point person for the project and help drive their team's QI efforts. Our initial purpose was to describe the role of these champions and our primary research question was, How did change champions impact a team's QI effort? What emerged during this inductive approach was an understanding of 2 types of champions: project champions and organizational change champions. This distinction was not conceptualized for the EPIC intervention design but was evidenced in some practices. Our analysis, then, explored practices that had both types of champions, one type or the other, or neither type, and we sought to understand how these variations impacted practices' efforts to implement and sustain their QI changes.
Methods
EPIC was launched in 2005 as a comparative effectiveness research trial of 3 approaches to improve diabetes and depression care. This article describes a secondary analysis of one arm of the trial (described later) and is focused on the role of change champions to better understand processes of QI implementation and sustainability; it does not describe or explain the overall clinical outcomes of the EPIC intervention.
All primary care practices serving adult patients along the front range of Colorado were eligible to participate. Practices were recruited through joint efforts of the Colorado Clinical Guidelines Collaborative and the State Networks of Colorado Ambulatory Practices and Partners, a collaboration of 3 practice-based research networks in Colorado. Thirty-seven practices provided informed consent and were randomized into one of the 3 trial conditions (EPIC arm, n = 14).
The EPIC Intervention
This intervention addressed broad chronic care improvements within each practice on the basis of an assumption that there would be a greater likelihood of sustained improvements when a practice had implemented chronic care office systems. This required that practices have the capacity to make and sustain improvement in their care systems and processes. Thus, the intervention also devoted attention to improving practices' capacity for change by enhancing the organizational context including communication, trust, and teamwork.
EPIC used an organizational change model comprised of 3 interrelated components: (1) an initial practice assessment, (2) externally facilitated improvement team meetings, and (3) two learning sessions. For the initial practice assessment (the multimethod assessment process),37 study facilitators used ethnographic techniques (eg, observations and interviews) to understand the initial conditions of each practice (eg, aspects of leadership, communication, work relationships, patient population) and the practice's current diabetes and depression care processes and to begin to work with the champion(s) in each practice.
Champions for the EPIC intervention were conceptualized as individuals who would be the point person for the project and help drive their team's QI efforts. As such, they were key members of the improvement team, which consisted of a diverse subgroup of practice members (depending on the size of the practice). Improvement teams met up to 11 times over the 6-month time frame; meetings lasted approximately 60 minutes. Each improvement team used an iterative process described elsewhere as the reflective adaptive process (RAP).38 The facilitator guided the team through application of practical QI tools and methods to address diabetes and depression care needs. Three study facilitators, all whom were Certified Diabetes Educators, received specific training in the use of a number change management strategies including (1) brainstorming; (2) rapid cycle tests of change; (3) detecting causes of process variation; (4) benchmarking for best practices; and (5) monitoring process changes.
EPIC also required that at least 2 individuals from each practice (including the project champion) attend two 1-day learning sessions held locally. The learning sessions provided an opportunity for practice members to share successes and challenges with other practices and to receive additional information from the research team for their practice-based QI efforts.
EPIC was approved by the Colorado Multi-Institutional Review Board. Medical directors, lead physicians, or both from each practice gave informed consent, as did participating staff members. All names have been changed to protect confidentiality. In addition, we have used dual sex identification (eg, his/her) throughout to further mask subjects' identities.
Data Collection
Data collection for the larger trial was designed to report on clinical outcomes (answering the question, Did the intervention work or not?) as well as the implementation/change process (answering the question, How and why did the intervention work—or not—across practices?). The role of the champion was one of the aspects of the implementation/change process that was consistently captured in the data across practices.
Data for this analysis included field notes, transcriptions of interviews conducted at baseline and 9 and 18 months, and transcriptions of metaRAP (periodic debriefing of the 3 facilitators).
Field Notes
Study facilitators spent up to 5 days in each practice for the initial practice assessment (before the start of the intervention); they followed an assessment guide to observe and record current practice care processes, individuals' roles and routines, and various organizational elements such as communication, leadership, and teamwork. During each observation, facilitators wrote “jottings,” which were then typed into longer, narrative field notes at the end of each day. Data also included conversations (not considered formal “interviews”) with each practice member to discuss the project. Similar kinds of field notes also were written for the improvement team meetings, learning sessions, and follow-up assessments at 9 and 18 months after the intervention. Follow-up assessments (at 9 and 18 months) also included gathering specific data on sustainability and practice members' perceptions of the value and success of the intervention.
Interviews
Study facilitators interviewed key practice members, typically including the lead physician/owner, office manager, and project champion(s) as part of the assessment; they followed a semistructured interview guide that sought individuals' perspectives on the practice's current care processes for diabetes and depression and potential ideas to improve these, as well as the organizational context such as communication, leadership, and teamwork. Interviews were audio-recorded and transcribed verbatim.
MetaRAP
During the intervention time frame, facilitators held regular metaRAP meetings (typically one per month) to provide support and insight to help each other based on their experiences within the practices. These meetings were audio-recorded and transcribed verbatim. These were beneficial for our analysis by providing insights into the implementation process, the facilitators' decision-making process, and facilitator perspectives of the practices/teams that may not have been captured in their regular field notes.
Selection of Practices for Analysis
After the intervention and data collection were completed, the authors asked the 3 facilitators to collectively discuss and rank-order the 14 practices in terms of how well each engaged with the intervention. Discussion continued until consensus was reached. Based on the facilitators' subjective assessments, criteria for “engagement” entailed how well practice leaders and staff used the intervention (ie, team-based meetings and learning sessions) to improve their work and care processes. Using this ranking, we began in-depth analyses of practices ranked both high and low in engagement and subsequently selected additional practices with variation in practice size, ownership, and geographic location. For this analysis we purposefully selected 8 practices that reflected differences across the spectrum of engagement with the intervention, level and intensity of improvement activity, and variability in demographic and contextual characteristics.
Data Analysis
All authors were involved with the current analysis, which entailed an immersion/crystallization technique39 that consisted of cycles of reading data followed by discussion/reflection, which were repeated until there was a consensus of interpretation. Because the data for each practice included an extensive set of field notes and transcriptions, steps were taken to make the analysis both manageable and rigorous by using 2 analysis teams: one from Colorado and the other from New Jersey. In their respective teams, the authors read and coded the data for each of the 8 practices and created a case summary of the practice and the improvement process. The 2 teams held regular meetings via conference calls and in-person analytic retreats to ensure that all authors had similar understandings of each practice and improvement process. To focus our analysis, we drew on strategies from Miles and Huberman40 by developing a matrix of key concepts. The authors returned to each practice's dataset to fill in the cells of the matrix, inserting brief excerpts of raw text to substantiate claims or interpretations. This analytic step facilitated cross-case comparisons and in-depth explorations of specific concepts including the project and organizational change champions.
Results
Our initial research question focused on project champions—those who served as the point person for the project and helped drive their team's QI efforts. All but one practice evidenced someone who took on this role. However, from our analysis emerged a distinctly different type of champion that we labeled an “organizational change champion.” This second champion, evidenced in some practices, supported not only the specific change efforts for the project but also a broader and longer-term trajectory of ongoing improvement. Our results are structured to (1) report 2 case examples that help to distinguish these champion roles and provide details of variations where both types were present; (2) report a case example of misalignment between champion types; and (3) report case examples of practices that lacked one or both types of champions. In all 3 sections, we present findings on the impact of these variations on the quality improvement process.
Project and Organizational Change Champions
Drawing on the existing literature and our data, we identified 7 distinguishing characteristics of these 2 champion roles (see Table 1). Although both types of champions do many of the same activities, what largely differentiates the 2 is the focus and boundaries of the change effort that is being championed. The project champion's role is focused on and derived from a particular project-based innovation, whereas the organizational change champion's role assumes a broader vision that sees individual changes in the context of a larger mission of practice transformation. Across practices, we found variations in who took on the project and organizational change champion roles, how they evolved, and how they mattered for the teams' change efforts.
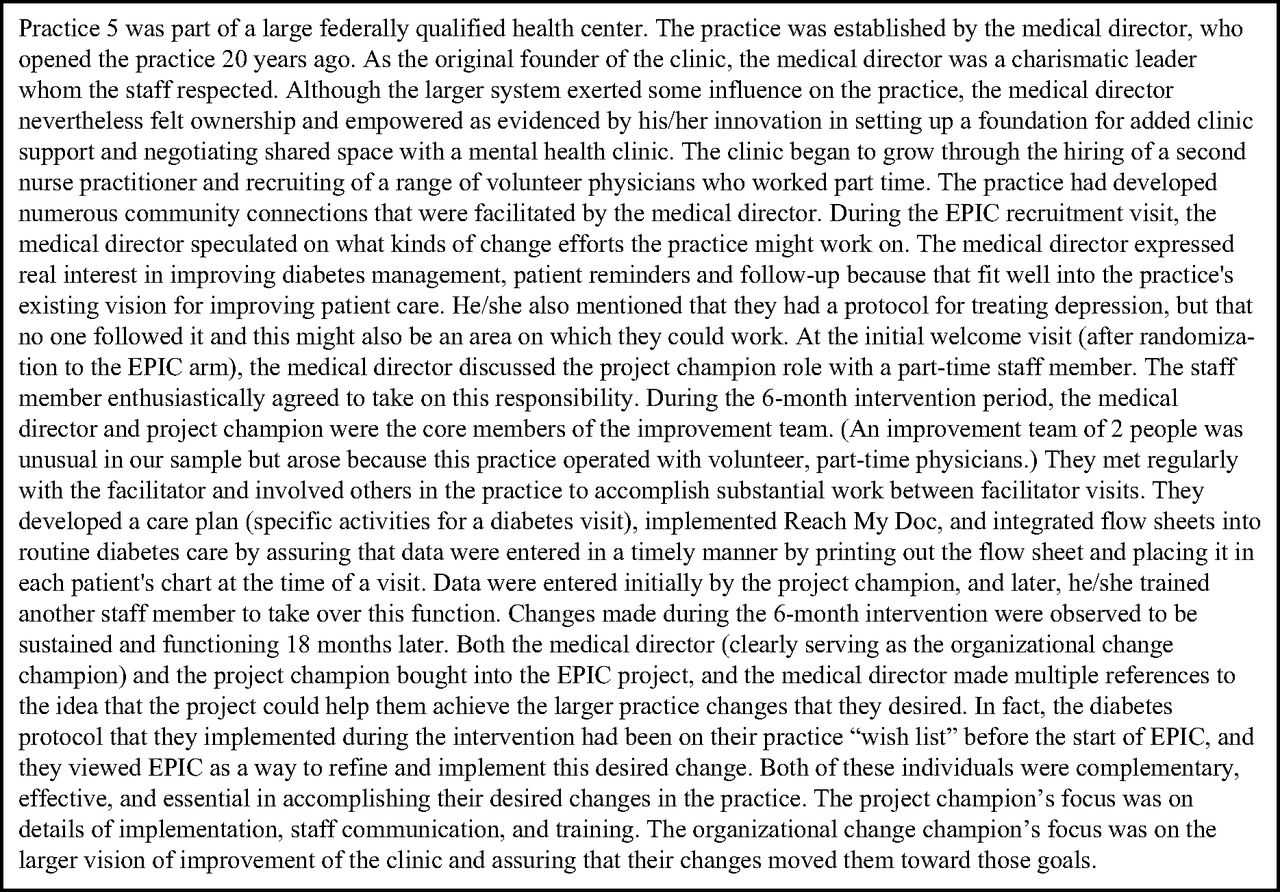
The case study of practice 5 highlights the distinctions between the project and organizational change champions and their respective effect on the change process (see Box 1). This practice had both a project champion and organizational change champion who functioned in complementary ways but with a different orientation and focus on change. The medical director, who had developed the practice from the ground up, was the organizational change champion, articulated a clear vision for ongoing practice change, and garnered support from many other stakeholders to enact that vision. A volunteer nurse in the practice served as the project champion, and with the medical director's support was able to effectively lead their EPIC-based changes. With the presence of both champion roles, this practice was able to implement and sustain a patient registry and a comprehensive protocol for diabetic visits.

Box 1. Case example of practice 5.
Practice 1 and practice 8 offer 2 variations of practices with both project and organizational change champions that were successful in implementing and sustaining their change goals. In practice 1, both the project champion and organizational champion roles initially were held by one person (the lead physician), but the project champion role evolved to include others over the course of the intervention. The lead physician was young and enthusiastic and had a vision for the future of the practice that included a population-based approach to patient care, and he/she saw participation in EPIC as a resource toward that vision. He/she was very active in the early stages of the project by providing practice change ideas, identifying team members, and enthusiastically participating in the improvement team meetings. As the intervention progressed and the team became established in their efforts to implement an electronic recall system for their diabetic patients, the physician began to reduce his/her direct involvement on the project-based innovations. This created the opportunity for the other 2 team members to emerge as project champions, taking on a sense of ownership and responsibility for the project and updating the physician on their progress. At the 18-month follow-up assessment, the practice continued to use their electronic recall system successfully and they had plans to expand it beyond diabetic patients to include annual physicals and well-baby checks.
In practice 8, the project champion and organizational change champion roles were held by one person throughout the entire intervention. The lead physician had a vision for the practice that involved providing better chronic care, and he/she saw the EPIC intervention as contributing to this vision. He/she was an exceptional facilitative leader, generating a remarkable level of buy-in for the project and fostering a sense of teamwork as the team collectively developed and implemented a protocol for diabetic visits that involved each functional area of the practice. The lead physician also clearly articulated to others the connection between the focus of the EPIC project and the larger, ongoing improvement goals of the practice. Unfortunately, toward the end of the intervention, the lead physician announced that he/she would be leaving the practice to take another job. Although they appointed another physician to be the project champion, this physician did not have the vision or the leadership skills of an organizational change champion, and as soon as the EPIC intervention ended, the improvement team became inactive. The changes the team had implemented were inconsistently maintained.
Misalignment between Project and Organizational Change Champions
In practice 7, a project champion (a physician assistant) emerged early in the intervention as a direct result of his/her interest in improving their diabetes care specifically. There also was evidence of an organizational change champion (one of the practices' 3 physicians); however, the 2 champion roles were misaligned, which had a deleterious effect on the practice's improvement process. Alignment is defined here as the synchronization of strategic goals with operations and execution tactics. Thus, being misaligned is operationalized here as any disconnect between the vision and ongoing change strategy of the organizational change champion and the intervention-specific goals and actions of the project champion. For example, the organizational change champion regularly articulated a number of innovative change ideas and had support from other practice members to implement them. He/she did not, however, see the relevance of the EPIC intervention for the changes they envisioned and chose to have minimal involvement with the improvement team. He/she gave permission to the physician assistant to lead the EPIC intervention and thereby gave him/her the authority to implement change efforts related specifically to EPIC. As an enthusiastic project champion, the physician assistant was able to work with the team to implement a recall system for diabetic patients, coordinate a diabetes open house, and develop a protocol for diabetes visits. Unfortunately, these changes were not sustained, in part, because the physician assistant did not have the authority to institutionalize the changes once the study ended. Not being aligned with the organizational change champion, the project champion's efforts did not have a lasting impact on the practice.
Lacking Either/Both Champions
We found 3 practices that had a project champion but no organizational champion (practices 2, 3, and 4) and one practice that did not have either (practice 6). We explore examples from these to show how the lack of one or both types of champions challenged the implementation and sustainability of the practices' innovations.
In practice 2, a physician assistant emerged as the project champion, but the practice's change efforts suffered from not having an organizational change champion. Although the lead physician initially seemed to have the potential of being the organizational change champion, there was additional evidence that he/she did not cultivate an environment or provide leadership for ongoing practice change. For EPIC, the lead physician made unilateral decisions about what the team would focus on, which included improving office morale and implementing a diabetic patient registry. He/she also revealed an inconsistent practice change vision by abandoning the patient registry after the intervention was over. Over the course of the intervention, it also became clear that the lead physician was actually instigating disharmony in the practice. Despite the work of the project champion to implement and populate the registry, his/her efforts could not be sustained without the leadership and consistent support of the lead physician.
Practice 4 was part of a federally qualified health center. Two individuals from this practice (the medical director and office manager) volunteered to be project champions. Both were effective in driving their project-based innovations; however, their efforts were stunted because they did not have an organizational change champion to help them integrate these changes into ongoing practice change efforts. The project champions were enthusiastic about their EPIC-based changes and were instrumental in involving appropriate staff in discussions and maintaining enthusiasm for the project. Neither, however, was effective in navigating the sociopolitical environment of the larger system to institutionalize their new innovations. This likely contributed to the larger system overturning some of the EPIC-based innovations that the team tried to implement. At the 18-month follow-up, the practice had experienced considerable turnover, including the medical director, which also negatively impacted the practice's ability to sustain their EPIC-based changes.
Practice 6 had neither a project champion nor an organizational change champion. This practice was comprised of a single physician and 2 staff. Although the facilitator led several EPIC team meetings, there was sporadic attendance and a lack of energy to implement new ideas. At one point, the physician acknowledged a sense of guilt in wasting the facilitator's time. During the intervention, they began intermittently using the 9-item Patient Health Questionnaire and a manual tracking system for patients with depression. By the 18-month follow-up, the physician reported that they continued to use the 9-item Patient Health Questionnaire but the tracking system had been abandoned. They discontinued holding improvement team meetings as well. Ultimately, there was little enthusiasm for implementing EPIC-related innovations, no evidence of a vision for ongoing practice improvement, and a lack of change leadership.
Discussion
This analysis sensitized us to the differences between the roles and functions of a project champion and an organizational change champion in team-based QI efforts in primary care settings. Both roles are valuable and the effectiveness of the combination seems to be associated with both the intensity of change activities during the intervention and the extent to which changes were sustained after the intervention. Those practices that had effective project champions and organizational change champions were best able to implement and sustain their desired improvements. However, the presence of both types of champions is not necessarily sufficient for effecting change, as evidenced in the case example of misalignment between project and organizational change champions. Moreover, our findings indicate that project champions played a key role in implementing project-based innovations. Yet, without an organizational change champion who provided leadership, authority, and a vision for the “big picture” of ongoing organizational change, the sustainability of their project-specific change efforts was hindered. Last, our findings support previous work that has shown the negative effects of not having any champion for the change process.2,41,42
Although our findings reinforce the importance of project champions for making discreet improvements in small primary care practices, the kind of transformation that is envisioned by the patient-centered medical home cannot be achieved through only a series of incremental improvement projects.42 Transformation instead requires a sustained improvement effort that is guided by a larger vision and assures that individual changes fit together into a meaningful whole. The literature is replete with examples of successful individual improvement projects, but it is thin on examples of successful transformation that emerges from a sustained pattern of improvement. From our analysis, we conclude that transformation requires not only effective project champions but effective organizational change champions as well.
This article fills some important gaps in the current literature about change champions. Previous studies have noted the importance of different types of champions for driving an innovation through the phases of initiation, development, and implementation.32,43,44 Our analysis identifies a distinction between 2 types of champions that has, to date, been absent from the literature. Our results revealed that practices could accomplish project-based innovations during the time frame of the intervention study with only a project champion. But, for the project-based innovations to be sustained and integrated into the ongoing vision of practice change, there must be an organizational change champion. This role could be performed by the project change champion or by a separate person. If multiple people fulfill these roles, they need to be aligned. In fact, our results highlight the deleterious effects of the change process when the project and organizational change champions were effective in these roles but not aligned in their purpose and vision. This finding speaks to the importance of clear communication between champions, having a clear understanding of the structure of power and authority within the organization, and communicating a clear vision to the entire practice of the project-based innovation and how it fits into ongoing practice change.
Another finding points to the evolving nature of the champion roles. Although there is a dearth of research that has focused on this aspect of change champions, one study identified the evolution of a project champion from team leader, to coach, and finally to salesperson.45 We found that there was not a single pathway for the emergence and development of change champions for successful implementation of project-based innovations. For example, a single person may initially take on both project and organizational change champion roles, and as the team develops, new project champions can emerge who take over the primary responsibilities of the project. When there are open lines of communication and working relationships that allow such evolutions to occur, the change process can be enhanced.
Our analysis also points to the importance of champions' leadership skills. Previous research has noted that charisma can only get a champion so far and champions need “facilitative leadership” qualities, which include the ability to empower staff and create psychologically safe and respectful environments for culture change.42 In our analysis of small to medium sized practices, the organizational change champions were the owners and lead physicians. Yet ownership does not equate with being an organizational change champion. Our findings revealed that one's position as a practice leader does not always translate into effective leadership behaviors for ongoing practice improvement. Researchers and interventionists should not, then, assume that practice leaders have the abilities and skills to drive new innovations. Leadership skills should be carefully assessed, and interventions should build in opportunities for champion development when needed.
We recognize limitations in our analysis. First, we focused only on how champions influenced the extent to which changes were made and sustained. We do not report on associations between champion roles and clinical performance measures. Given the dearth of research about champions, we believe this focus was warranted. Additional research is needed to better understand the complex dynamics of individual change champions, team functioning, and clinical outcomes. Also, we recognize that the interpretative nature of our analysis can raise questions of validity. The benefits of qualitative research include in-depth understandings of a phenomenon. We took strategic steps to minimize researcher bias through ongoing discussions among the authors; we looked for disconfirming evidence to challenge and update our preliminary findings; and we used rigorous techniques to verify our interpretations and conclusions.
Conclusions
Primary care practices face extensive challenges in becoming patient-centered medical homes and good citizens of the health care neighborhoods envisioned by the accountable care organization model. Transformation to new models of primary care practice requires the ability to make and sustain a program of continual adaptation and improvement. Change champions—both project and organizational change champions—are critical players in supporting both innovation-specific and transformative change efforts.
Acknowledgments
We are grateful to the practice clinicians and staff who participated in the EPIC study. We would like to acknowledge the study facilitators, who diligently worked with the practices.
Notes
This article was externally peer reviewed.
Funding: The trial on which this secondary data analysis is based is supported by a grant from the National Institute of Diabetes and Digestive and Kidney Diseases (DK067083) and the National Institute of Mental Health (MH069806).
Conflict of interest: none declared.
- Received for publication September 30, 2011.
- Revision received March 14, 2012.
- Accepted for publication March 19, 2012.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Mixed Methods Evaluation of the 'Caring for Providers to Improve Patient Experience intervention
- The role of emergent champions in policy implementation for decentralised drug-resistant tuberculosis care in South Africa
- Increasing North Carolinas Workforce Capacity for Prescribing Buprenorphine Products
- Distributing leadership for scaling up evidence-based innovation in LMICs: a case for leadership development in India
- Strategies supporting sustainable prescribing safety improvement interventions in English primary care: a qualitative study
- ThinkCancer! The multi-method development of a complex behaviour change intervention to improve the early diagnosis of cancer in primary care
- Evaluating the impact of a champion on implementation of the Back Skills Training (BeST) programme in Canada: a mixed methods feasibility study protocol
- Staff experiences of enhanced recovery after surgery: systematic review of qualitative studies
- Implementation of Technology-based Patient Engagement Strategies within Practice-based Research Networks
- Practice Facilitation to Improve Diabetes Care in Primary Care: A Report From the EPIC Randomized Clinical Trial
- Primary Care Research Conducted in Networks: Getting Down to Business