
Abstract
Objective: To determine whether electronic health record (EHR) documentation of certain early childhood risk factors for asthma, such as wheeze differ by race, ethnicity, and language group, and whether these children have different subsequent asthma prevalences.
Methods: We used EHR data from the Accelerating Data Value Across a National Community Health Center (ADVANCE) Clinical Research Network from children receiving care in US community health centers (n = 71,259 children) across 21 states to examine the presence of ICD-coded documentation of early childhood wheeze and its association with subsequent asthma diagnosis documentation in the EHR by race/ethnicity/language.
Results: ICD-coded wheeze was present in 2 to 3% of each race/ethnicity/language group. Among the total sample, 18.5% had asthma diagnosed after age 4. The adjusted prevalence of subsequent asthma diagnosis was greater in children with wheeze than those without. Odds of asthma diagnosis did not differ among children in all race/ethnicity/language groups with early childhood wheeze. Non-Latino Black children without wheeze had higher odds of asthma (OR = 1.19, 95% CI = 1.08-1.32) compared with non-Latino White children without wheeze.
Discussion: In US community health centers which serve medically underserved populations, EHR documentation of early childhood wheeze was uncommon and did not differ significantly among race/ethnicity/language groups. Differences in asthma diagnosis in Latinos may not stem from differences in early-life wheeze documentation. However, our findings suggest that there may be opportunities for improvement in early asthma symptom recognition for non-Latino Black children, especially in those without early childhood wheeze.
Introduction
Asthma outcomes have been found to differ by race and ethnicity.1 Birth cohort studies have examined many early childhood risk factors for asthma development such as health, family history, and environment.2,3 There is evidence that children who wheeze in early childhood are more likely to develop asthma later in childhood,2,4 but there is still uncertainty about whether early childhood wheeze is a symptom that some children experience more than others (eg, by race/ethnicity and language group), whether the recognition of this early childhood symptom differs between racial/ethnic groups, or whether recognition of early childhood wheeze by clinicians is differentially associated with eventual asthma diagnosis. There are few studies that examine this early childhood course using electronic health records (EHR), which offer an objective measure of early childhood wheeze rather than self-reported responses subject to recall bias.
United States (US) community health centers (CHCs) are clinics that serve disproportionately high numbers of patients in racial/ethnic minority groups, including Latino children and patients who prefer to use a language other than English;5 and are also a setting where many children receive asthma care. We used a measure of clinician-diagnosed wheeze in early childhood to examine whether it was associated with subsequent diagnosis of asthma and how that differed in Latino (Spanish or English-preferring), non-Latino Black, and non-Latino White children receiving care at CHCs. We hypothesized that overall, children with documentation of early childhood wheeze will have higher odds of later asthma diagnosis documented on their medical record, but that asthma diagnosis documentation may differ between race/ethnicity/language groups.
Materials and Methods
We used EHR data from 21 states in the Accelerating Data Value Across a National Community Health Center Network (ADVANCE) Clinical Research Network of PCORnet, a national network of CHCs during the study period of 2005 to 2017. We included children who had ≥1 visit before their fourth birthday to assess wheeze in early childhood, and ≥1 visit after turning 4 years old (through age 17 years) to determine subsequent asthma diagnosis. Thus each child had a minimum of 2 visits (1 visit before 4 years and 1 after turning 4 years).
The outcome was asthma diagnosis after the fourth birthday (using International Classification of Disease (ICD) codes 493* or J45*). The first independent variable included clinician-diagnosed early childhood wheeze before the fourth birthday (ICD codes 786.07 or R06.2). The second independent variable was a combination of race, ethnicity, and language, operationalized as English-preferring Latino, Spanish-preferring Latino, non-Latino Black, and non-Latino white. Covariates included patient-level characteristics: sex, number of clinic visits per year, household income as percent of the federal poverty level, overweight/obesity (≥85th percentile for age/sex), and tobacco smoke exposure before age 4.
Statistical Analysis
We used descriptive analyses to examine patient characteristics. For the main analysis, we used generalized estimating equations logistic regression including the main effects and interaction effect between wheeze before age 4 and race/ethnicity/language, including the above-listed covariates, to obtain adjusted odds ratios (ORs) and corresponding 95% confidence intervals. The GEE model utilized an exchangeable working correlation structure to account for the clustering of patients within clinics. All statistical tests were performed with a 2-sided type I error of 5%. Analyses were conducted using Stata (version 15). This study was Institutional Review Board approved. The data used in this study are collected during routine primary care and consent from patients to use data in research is obtained from clinics. The data are deidentified before transfer to the study team.
Results
The sample included 71,259 children who received care at CHCs between 2005 to 2017 (Table 1). Table 2 shows, by presence of early childhood wheeze, the adjusted prevalence of asthma diagnosis among our 4 racial/ethnic groups. The difference in prevalence of asthma diagnosis documentation between those with documented early childhood wheeze and those without ranged from 10 to 15%. Notably, asthma diagnosis after age 4 was more prevalent in non-Latino black children. All children with early childhood wheeze were more likely to have asthma diagnosis subsequently documented, and the differences between the race/ethnicity/language groups was similar within wheeze groups (Table 2).
Characteristics of Community Health Center Patients, 2005–2017 (n = 71,259)
Adjusted Prevalence of ICD-Coded Asthma Diagnosis in the Electronic Health Record after Age 4, Stratified by Presence of Early Childhood Wheeze
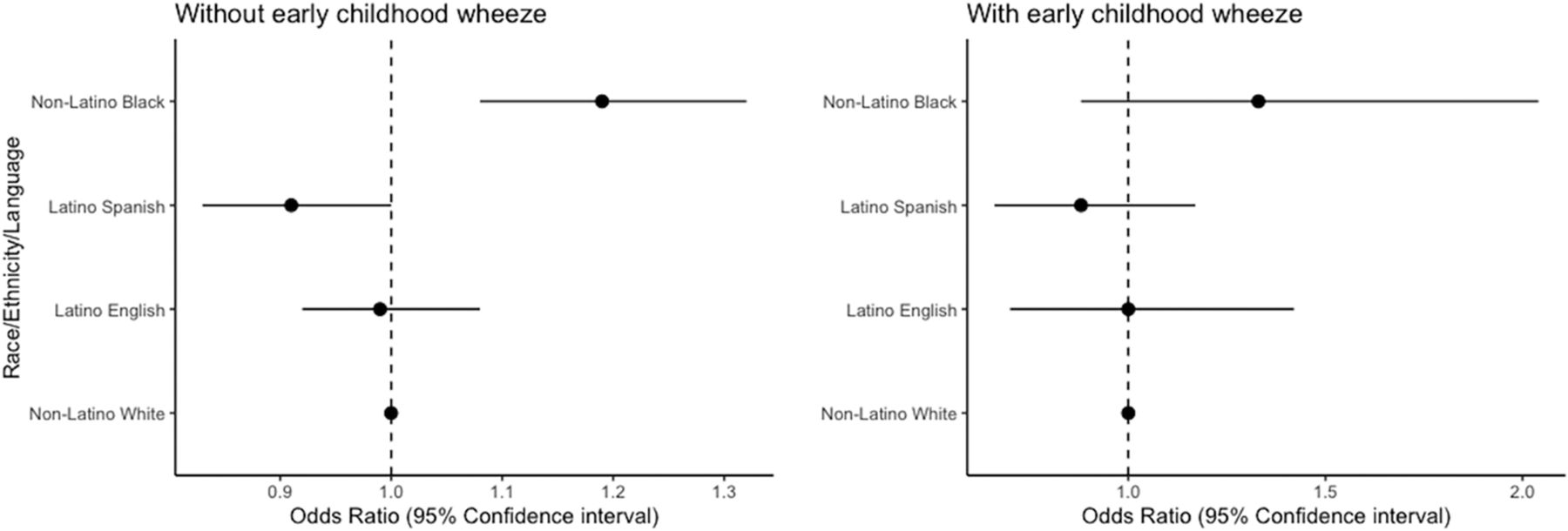
Figure 1 shows covariate-adjusted odds of asthma diagnosis after age 4. Compared with non-Latino White children who did not wheeze, non-Latino Black children without wheeze had higher covariate-adjusted odds of later asthma diagnosis (OR = 1.19, 95% CI = 1.08-1.32). Latino children (English- and Spanish-preferring) without wheeze had similar odds to non-Latino white children without wheeze of developing asthma. Among children with early wheeze, all had similar odds of later asthma diagnosis compared with non-Latino white children with early childhood wheeze.

Odds ratios of asthma diagnosis after age 4 by race, ethnicity, language groups. Generalized estimating equation models adjusted for sex, visits per year, income, insurance, body mass index, and household smoke exposure before age 4.
Discussion
Among children with early childhood wheeze, documented diagnosis of asthma after age 4 did not differ by race/ethnicity/language in children. However, non-Latino Black children without early childhood wheeze had increased odds of asthma diagnosis documentation later in childhood.
In our sample of CHC patients, differences in asthma diagnosis documentation in Latinos likely do not stem from differences in the documentation of this early life symptom. Our finding that non-Latino Black children have a higher asthma burden is consistent with prior literature.6,7 Our adjusted findings show that this burden may be more disparate in Black children without early childhood wheeze. Because wheeze is a commonly understood symptom of obstructive lung pathophysiology,8 these results suggest that disparities in asthma diagnosis may occur in Black children who also have less typical symptom courses (chronic cough, for instance, or prolonged symptoms after upper respiratory infection). These less typical symptoms should be noted by clinicians to start early treatment for asthma. In addition, asthma symptoms in younger children are often viral-induced and do not always include wheeze as opposed to later in childhood when longer-lasting wheeze occurs.9 We did not evaluate these phenomena, however, and this would be productive ground for further research. In addition, although we were limited to ICD-coded wheeze (meaning some wheeze was likely missed as it is a symptom of many conditions that could be coded instead), a diagnosis code of wheeze will likely capture the most severe wheezers, so we are confident that those classified as having early childhood wheeze actually did wheeze. We also do not have data on clinician behavior and attitudes regarding the choice to include an ICD code for wheeze versus other diagnosis codes that include wheeze as a symptom. In addition, it is possible that asthma could be missed in some children at well-child checks who may seem healthy. Furthermore, as all our data come from CHCs, these findings may not be generalizable to all patients in the US, however, many children in the US do receive care at CHCs.5
Although early childhood wheeze is an important factor in later diagnosing asthma, our findings suggest opportunities for improvement in early asthma symptom recognition, especially in those without early childhood wheeze.
Acknowledgments
This work was conducted with the Accelerating Data Value Across a National Community Health Center Network (ADVANCE) Clinical Research Network (CRN). ADVANCE is a CRN in PCORnet, the National Patient Centered Outcomes Research Network. ADVANCE is led by OCHIN in partnership with Health Choice Network, Fenway Health, and Oregon Health & Science University. ADVANCE’s participation in PCORnet is funded through the Patient-Centered Outcomes Research Institute (PCORI), contract number RI-OCHIN-01-MC.
Notes
This article was externally peer reviewed.
This is the Ahead of Print version of the article.
Funding: National Institute on Minority Health and Health Disparities (NIMHD). Grant number R01MD011404 to John Heintzman.
Conflict of interest: The authors have no conflicts of interest.
To see this article online, please go to: http://jabfm.org/content/00/00/000.full.
- Received for publication March 22, 2023.
- Revision received July 6, 2023.
- Accepted for publication July 18, 2023.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.