
Abstract
Background: There are known gender differences in both time spent on the electronic health record (EHR) and burnout. Previous studies have described potential benefits of staff support for documentation for physician experience and EHR time. It is not known, however, to what extent availability of staff support for documentation differs by gender in the context of primary care.
Methods: This was a cross-sectional study of primary care physicians (PCPs) using data from the 2018 and 2019 National Electronic Health Records Survey administrations. After descriptively analyzing the prevalence of staff support for documentation, we used multivariable logistic regression to identify the adjusted relationship of staff support for documentation with gender.
Results: Among the 813 physicians who endorsed having an EHR (92.5% of sample, representing 296,854 physicians), female PCPs were significantly less likely than male PCPs (25.1% vs 37.3%; P = .04) to report having staff support for documentation. This difference was most pronounced in practices with a single physician and practices with more than 50% of patients insured by Medicaid. Gender differences persisted in analyses adjusted for practice ownership and percent of patients insured by Medicaid.
Conclusions: Given positive effects of documentation support and known gender differences in burnout and EHR use times, the differences identified have important implications for the physician workforce. Future research should focus on identifying underlying reasons and potential solutions for the gender differences described.
- Cross-Sectional Studies
- Documentation
- Electronic Health Records
- Family Medicine
- Logistic Models
- Practice Management
- Primary Health Care
- Professional Burnout
- Women Physicians
- Workforce
Introduction
There are known gender and specialty differences in time spent on the electronic health record (EHR). Previous work has demonstrated that female physicians spend more total and after-hours time on the EHR1 and more time in the EHR per relative value unit on both clinic and nonclinic days. They also write longer notes and are less likely to close visits on the same day.2 Prior work also has shown that primary care clinicians (where women have a relatively greater representation as compared with other specialties3) spend more total and after-hours time on the EHR than medical or surgical specialists.4 Greater time spent on the EHR, particularly after hours, has been linked to higher levels of emotional exhaustion among primary care physicians.5 This could potentially augment the higher rates of burnout seen among female physicians across specialty types, including primary care.6,7
Use of documentation support, whether in the form of scribes, team-based documentation, or novel technologies that facilitate documentation, has the potential to enhance physicians’ experiences of documenting and providing clinical care. For example, in a randomized controlled trial, use of scribes in primary care was associated with enhanced work efficiency, improved visit interactions, and less after-hours documentation.8 In family medicine, a trial of scribes was associated with improvements in multiple aspects of physician satisfaction as well as with increases in the percentage of charts closed within 48 hours.9 When implemented as part of a broader team-based primary care transformation, team-based documentation, in which a team member such as a medical assistant uses a template to document complaint-based HPI information for a physician, has been associated with increased quality of care and provider and patient experience.10
Given gender differences in time on the EHR and the potential benefits of staff support noted above, improving staff support for documentation in primary care could be 1 important approach toward alleviating these disparities. It is not known, however, to what extent utilization of staff support for documentation differs by gender in the context of primary care. We sought to characterize differences in utilization of staff support for documentation by gender using a nationally representative sample of primary care physicians.
Methods
This was a cross-sectional study using data from the 2018 and 2019 administrations of the National Electronic Health Records Survey (NEHRS). The NEHRS is an annual, cross-sectional survey that queries a sample of physicians not employed by the federal government who provide office-based patient care in the United States and are identified from the master files of the American Medical Association and American Osteopathic Association. It does not survey physicians longitudinally. NEHRS is administered yearly by the National Center for Health Statistics. RTI International (Research Triangle Park, NC) collected data for the 2018 and 2019 NEHRS administrations between September 2018 and March 2019 and between June to December 2019, respectively.11,12 NEHRS administration details and sampling strategies are available from the National Center for Health Statistics.13
We combined responses from 2018 and 2019 for all analyses. From among 2000 and 10,302 physicians initially considered and 598 and 2280 physicians deemed eligible in 2018 and 2019, respectively, 393 completed the 2018 survey, and 1524 completed the 2019 survey. Using the standard Office of Management and Budget unweighted response rate calculation used for federal surveys,14 this represented 36.1% and 41.0% unweighted response rates for 2018 and 2019, respectively. The NEHRS survey queries physicians on their age, gender, specialty, practice setting, practice ownership, the number of physicians in the practice, insurance accepted in their practice, and the percent of patients in the practice insured by Medicaid. It also asks whether physicians have “staff support (eg, scribe) to assist you with documenting clinical care in your medical record system.”
We limited our analysis to the 878 respondents identified as primary care physicians based on classifications adapted by NEHRS from the American Medical Association.11,12 According to this categorization, specialties classified as primary care specialties include family medicine, geriatric medicine, internal medicine, internal medicine/pediatrics, obstetrics and gynecology, pediatrics, sports medicine, and combinations of these specialties.
After describing sample characteristics overall and by gender, we descriptively analyzed the prevalence of staff support for documentation by physician and practice characteristics. We then used multivariable logistic regression to identify the adjusted relationship of our outcome with gender. Because practice size was collinear with practice ownership and age was collinear with gender, we only adjusted for practice ownership, the percent of patients in the practice insured by Medicaid, gender, and survey year in our main model. We also conducted a sensitivity analysis adjusting for physician gender, physician age category, practice ownership, practice size, the percentage of patients in the practice insured by Medicaid, and survey year. Analyses were conducted using SAS OnDemand for Academics with a 2-sided α of 0.05 using prespecified NEHRS weights to obtain nationally representative estimates. Weights are determined by the sampling methodology and nonresponse patterns to facilitate accurate representation of physician specialty group and geographic area. Given that the data used in this study is publicly available on the NEHRS site and deidentified, this study was exempt from institutional review board review and informed consent.
Results
Our unweighted sample included the 92.5% of primary care physicians (n = 813) who endorsed having an EHR. This represented a weighted sample of 296,854 physicians. A majority of physicians in the sample were male (53.7%) and over age 50 (70.8%). Most practiced in a physician-owned practice or physician group (53.7%) and in a practice setting of 10 or fewer physicians (73.7%) (Table 1).
Sample Characteristics
Consistent with prior data regarding the gender breakdown of US primary care specialists, 42.3% of the sample consisted of female physicians.3 Physicians in this sample were older than those in the US primary care physician population.15 Female physicians in the sample were significantly younger (41.6% of female physicians under age 50 vs 18.6% of male physicians; P < .001). There were no significant differences in distribution of practice ownership or practice size by physician gender, or clear patterns in percent of patients with Medicaid by gender (Table 1).
In unadjusted analyses, female physicians were significantly less likely to report having staff support for documentation (25.1% for female physicians vs 37.3% for male physicians; P = .04). When stratified by practice size and percent of patients with Medicaid, significant gender differences in staff support were seen in practices with a single physician (15.6% of female physicians reporting staff support for documentation vs 84.4% of male physicians; P < .001), and practices with more than 50% of patients insured by Medicaid (19.9% of female physicians reporting staff support for documentation vs 80.1% of male physicians; P < .001) (Table 2).
Staff Support for Documentation by Gender and Additional Demographic and Practice Characteristics
In analyses adjusted for practice ownership, the percent of patients insured by Medicaid, and survey year, female primary care clinicians remained significantly less likely to have staff support for documentation than male counterparts (OR, 0.53; 95% CI, 0.30–0.94; adjusted percentages with staff support for documentation: 23.5% for female physicians vs 36.5% for male physicians) (Figure 1). In a sensitivity analysis adjusting for physician sex, physician age category, practice ownership, percent of patients insured by Medicaid, practice size, and survey year, there were no substantive differences in results.
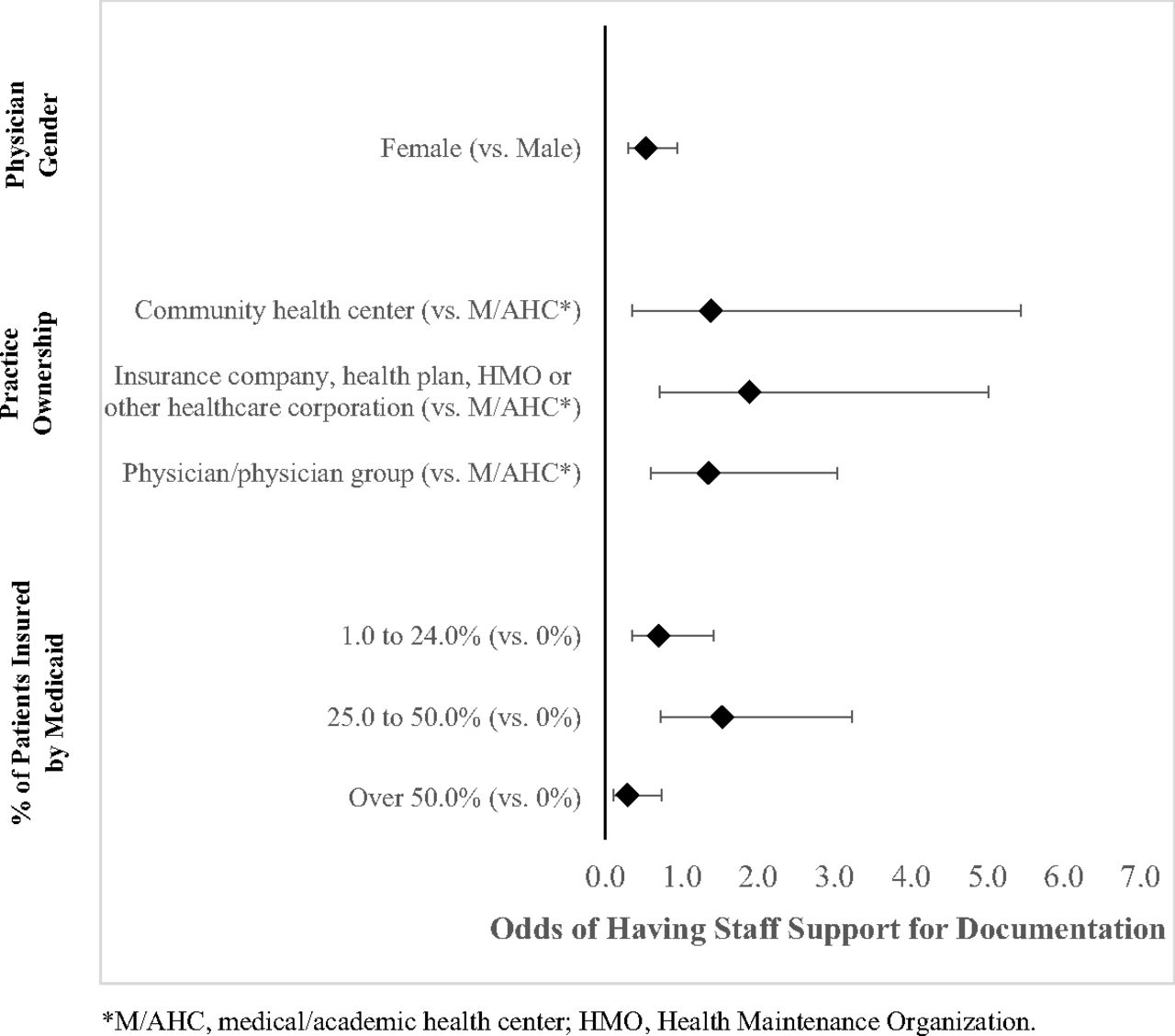
Adjusted odds ratios for presence of staff support; Abbreviations: M/AHC, medical/academic health center; HMO, Health Maintenance Organization.
Discussion
Across a national sample of primary care physicians, we found significant gender differences in staff support for documentation, with female primary care physicians significantly less likely to report staff support for documentation than their male counterparts. These differences persisted when adjusting for practice ownership and percent of patients insured by Medicaid. In stratified analyses, female physicians were less likely to have staff support for documentation in single physician practices and in practices with over 50% of patients insured by Medicaid.
Given known gender differences in burnout rates,6 EHR use times, and documentation length,2 associations between EHR time and burnout,5 and the positive effects of documentation support on physician experience,8 the differences we identified have important implications for the physician workforce. They suggest that enhanced attention should be given to reducing gender disparities in support for documentation in the primary care workforce, including perhaps targeted efforts by payers or health systems to facilitate adoption in solo practice settings. Documentation support could take the form of scribes, team-based documentation workflows, or ambient, technology-enabled documentation solutions with the potential to enhance provider experiences. In addition, a greater understanding of reasons for the differences identified is needed, including to what extent they are related to funding availability, physician preferences, workplace culture and dynamics, workforce interest in documentation support, or other issues.
Our findings of significant gender gaps in staff support for documentation in solo practices and those with more than 50% of their population insured by Medicaid suggest that these settings may particularly benefit from novel documentation support solutions. Previous work by Basu et al. demonstrated that in a fee-for-service payment model, clinical documentation assistance would need to save 3.5 minutes per encounter to avoid net revenue loss, while an advanced team-based care strategy in which medical assistants support documentation would need to save an average of 7.4 minutes per encounter to break even.16 Similarly, Miksanek et al. established that, based on average Medicare billing, an average of an additional 1.2 visits per day worth of revenue was needed to recover the costs of a scribe program in an internal medicine outpatient practice. These incremental time savings and increased revenue may be harder to achieve in solo practices and those with a greater portion of their population insured by Medicaid, thus potentially making these practices ideal candidates for documentation solutions that lean more heavily on technology (ie, ambient documentation solutions) as they are developed.17
A strength of our study is the use of data from a large, nationally representative database with information about both physician and practice characteristics. Response rate limitations, the restricted scope of the 2018 NEHRS administration, NEHRS’s focus on the outpatient setting, and the overrepresentation of PCPs above the age of 50 in this sample may reduce the generalizability of our findings. The study’s sample size may also have limited the significance of numeric differences seen in stratified analyses. Finally, as this was a multiple-choice survey, information about exact sources and details of staff support for documentation reported by respondents are not available.
Conclusion
There are significant gender differences in staff support for documentation among primary care physicians. Future research should focus on identifying the underlying reasons for these differences and identifying both workflow and technology solutions that can help close the documentation support gap.
Notes
This article was externally peer reviewed.
Funding: None.
Conflicts of interest: David W. Bates received grants from EarlySense and IBM Watson; personal fees from CDI Negev, ValeraHealth, and FeelBetter; owns equity in CLEW and MDClone; and serves as a consultant for Leapfrog.
To see this article online, please go to: http://jabfm.org/content/35/3/000.full.
- Received for publication February 18, 2022.
- Revision received May 19, 2022.
- Accepted for publication May 23, 2022.




{kind=link}