
Abstract
Background: Higher trust in healthcare providers has been linked to better health outcomes and satisfaction. Lower trust has been associated with healthcare-based discrimination.
Objective: Examine associations between experiences of healthcare discrimination and patients’ and caregivers of pediatric patients’ trust in providers, and identify factors associated with high trust, including prior experience of healthcare-based social screening.
Methods: Secondary analysis of cross-sectional study using logistic regression modeling. Sample consisted of adult patients and caregivers of pediatric patients from 11 US primary care/emergency department sites.
Results: Of 1,012 participants, low/medium trust was reported by 26% identifying as non-Hispanic Black, 23% Hispanic, 18% non-Hispanic multiple/other race, and 13% non-Hispanic White (P = .001). Experience of any healthcare-based discrimination was reported by 32% identifying as non-Hispanic Black, 23% Hispanic, 39% non-Hispanic multiple/other race, and 26% non-Hispanic White (P = .012). Participants reporting low/medium trust had a mean discrimination score of 1.65/7 versus 0.57/7 for participants reporting high trust (P < .001). In our adjusted model, higher discrimination scores were associated with lower trust in providers (aOR 0.74, 95%CI = 0.64, 0.85). A significant interaction indicated that prior healthcare-based social screening was associated with reduced impact of discrimination on trust: as discrimination score increased, odds of high trust were greater among participants who had been screened (aOR = 1.28, 95%CI = 1.03, 1.58).
Conclusions: Patients and caregivers reporting more healthcare-based discrimination were less likely to report high provider trust. Interventions to strengthen trust need structural antiracist components. Increased rapport with patients may be a potential by-product of social screening. Further research is needed on screening and trust.
- Caregivers
- Cross-Sectional Studies
- Doctor-Patient Relations
- Emergency Departments
- Healthcare Disparities
- Health Services
- Logistic Regression
- Outcomes Assessment
- Perceived Discrimination
- Primary Healthcare
- Screening
- Social Determinants of Health
- Trust
Background
The relationship between trust in healthcare providers and positive health behaviors is well established.1⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓–18 High levels of trust in providers has consistently been associated with adherence to treatment for a wide range of conditions, including hypertension, diabetes, depression, and inflammatory bowel disease among adults, and asthma among children.1⇓⇓⇓⇓⇓–7 High trust in providers has also been linked to increased use of preventive health services such as adolescent HPV vaccination and adult cancer screening, as well as greater patient satisfaction.8⇓⇓⇓⇓⇓⇓⇓⇓⇓–18
Critical to the healthcare system’s efforts to advance health equity, previous studies have found levels of trust in providers to be lower among non-Hispanic Black and Hispanic patients, compared with non-Hispanic White patients.19⇓–21 Poor self-rated health, which is similarly lower in non-Hispanic Black and Hispanic patients, has also been associated with lower trust.22⇓⇓–25 In part, these differences in trust by race and ethnicity may be attributed to experiences of healthcare discrimination; multiple studies have established links between patients’ experiences of discrimination in healthcare settings and low trust in their providers.26⇓–28
Associations between trust and discrimination are particularly compelling areas of research amid increasing calls to integrate social screening (eg, screening for housing stability and food security) into care delivery, to identify and address social drivers of health and promote health equity.29,30 A growing body of literature explores how trust in providers may increase both patient and caregivers’ perception of social screening acceptability.31⇓⇓⇓⇓⇓–37 Similarly, studies have found that healthcare providers perceive that social screening may facilitate patient communication and trust.38⇓⇓⇓⇓⇓⇓⇓⇓⇓–48 As healthcare-based social screening implementation expands,49,50 it is increasingly relevant to explore how social screening impacts trust across patient populations based on their experiences with discrimination and socioeconomic marginalization.
This study’s primary aim was to examine associations between patients’ and caregivers of pediatric patients’ trust in healthcare providers and experiences of healthcare discrimination. A secondary aim was to identify additional factors associated with high patient/caregiver trust in providers, including self-rated health and prior experiences of healthcare-based social screening.
Methods
This study was a secondary analysis of a cross-sectional survey of adult patients and caregivers of pediatric patients from 2018 to 2019.31,51 Participants were recruited from 11 primary care and emergency department sites across 9 states, with each site recruiting convenience samples of 100 adult patients or caregivers of pediatric patients (1 site recruited 50 participants based on site capacity) (Appendix 1). Patients and caregivers were eligible for the study if they met the following criteria: 1) did not require immediate medical attention, 2) were 18 years of age or older, 3) were able to speak and read English or Spanish, 4) were able to provide informed consent, 5) were comfortable using a tablet, and 6) were themselves a patient or caregiver of a pediatric patient getting care at a study site. Recruitment and survey methods have been described in detail in previous publications.31,51 The original study was approved by the institutional review board of UCSF, as well as by 8 of the study sites.
The main outcome was participants’ trust in their or their child’s healthcare providers at the study site. Participants were asked, “How much do you trust your/your child’s healthcare provider(s) at this clinic/emergency department?” Responses were measured on a scale of 1 to 10.52 Prior work has utilized a trichotomous cut point of 1 to 7, 8 to 9, and 10 for trust ratings; however, in this study, we aimed to explore the differences in groups with low/medium and high trust, rather than focusing on differentiating high versus complete trust.31,51 To that end, trust ratings were dichotomized into low/medium trust (1 to 7) and high trust (8 to 10). Caregivers of pediatric patients only responded regarding their trust in their child’s healthcare provider(s).
Participants’ experiences of healthcare discrimination were assessed using an adaptation of the Discrimination in Medical Settings Scale.53,54 Participants were asked whether they had ever experienced 7 distinct instances of discrimination in a healthcare setting due to their race, ethnicity, or socioeconomic status (eg, “felt like a doctor or nurse was not listening to what you were saying”) (see Appendix 2 for the full survey). Healthcare discrimination score was defined as the number of events experienced out of the 7 queried types of discrimination. This score was treated as a continuous variable in regression analyses. In descriptive analyses, healthcare discrimination was treated as a binary variable; participants who reported 1 or more of the 7 types of discrimination were classified as having experienced any discrimination versus those who experienced none.
Exploratory secondary analyses focused on measures of self-rated health and prior experience with healthcare-based social screening/assistance. Participants rated their or their child’s health status on a 5-point Likert scale; results were dichotomized into poor or fair versus good, very good, or excellent.55 Self-perceived SES was assessed by asking participants to place themselves on a ladder relative to other people in the United States, with 1 being the bottom of the ladder and 10 being the top. This measure is designed to assess participants’ subjective social status and has been validated among racially and ethnically diverse populations.56,57 SES ladder placement was treated as a continuous variable. To assess prior experiences with social screening/assistance, participants were asked, “In the past 12 months, not including today, have you been asked approximately any of the following in any healthcare setting?” and “In the past 12 months, not including today, have you received assistance from anyone in any healthcare setting related to…” Both questions were followed by a list of social domains of which the participants could select multiple options (eg, housing, food).
The survey also collected participant demographics, including race, ethnicity, sex, age, years of education, income, and preferred language. Due to low sample sizes in the American Indian or Alaska Native, Asian, and other race groups, these categories were combined into a singular non-Hispanic multiple/other race category. Similarly, all participants identifying as Hispanic were collapsed into 1 category, regardless of origin (eg, Mexican American). The race and ethnicity variable in this study was used as a proxy for experiences of interpersonal and institutional racism.58 In addition to participant-level characteristics, 2 site-level characteristics were included in the analysis: type of healthcare setting (primary care vs emergency department) and percentage of the patient population who were publicly insured/uninsured (dichotomized into less than 80% vs 80% or more).31,51 Aside from these 2 site-level measures, all measures were self-reported by participants.
Descriptive analyses using Chi Square tests were used to explore level of trust in providers and experiences of healthcare discrimination among the study sample. Univariable and multivariable logistic regressions were then used to examine associations between level of trust in providers and healthcare discrimination score, health status, having been screened for social risks in a healthcare setting in the past 12 months, and having been assisted with social needs in a healthcare setting in the past 12 months, while controlling for the following participant- and site-level characteristics: sex, race and ethnicity, age, education, income, SES ladder position, health status, preferred language, healthcare setting (primary care vs ED), percentage publicly insured/uninsured at site, and type of participant (adult patient vs caregiver of a pediatric patient), as well as cluster analysis at the site level.12,24,26,27,31,51,59⇓–61 Regression analyses utilized listwise deletion. We did not use multiple imputations because of the likelihood that data were not missing at random, but instead were missing due to the sensitive nature of the data (eg, self-reported income).62⇓⇓–65 Descriptive statistics for the disaggregated Hispanic group were calculated and provided in Appendix 3, as consistent with best practices in the reporting of race and ethnicity data despite small sample sizes.58,66 Unfortunately, this was not possible for the non-Hispanic multiple/other race group, due to very low sample sizes and concerns about participant confidentiality.
We used interaction terms to explore statistical interactions between healthcare discrimination score and other participant-level characteristics (demographics, health status, having been screened for social risks in a healthcare setting in the past 12 months, having been assisted with social needs in a healthcare setting in the past 12 months). These analyses aimed to explore potential differences in the relationship between healthcare discrimination and trust, given the known differences in levels of trust among different populations, the broad nature of the Everyday Discrimination Scale (with participants reporting discrimination based on race, ethnicity, or socioeconomic status), and gaps in knowledge regarding social screening among diverse populations.19⇓–21,24,25,67 Results were stratified by race and ethnicity. Model goodness-of-fit was assessed using R-squared and Akaike information criterion values; models were also evaluated for multicollinearity and specification error. Sensitivity analyses were performed to examine the effect of using a tertile-based cut point (1 to 7, 8 to 9, and 10) for the provider trust outcome. Because of the overall high ratings of trust among the sample, additional sensitivity analyses using a dichotomous 1 to 9 and 10 cut point, as well as a National Quality Forum-recommended 1 to 8 and 9 to 10 cutpoint, were also performed.68 In addition, we stratified by participant type (adult patient vs caregiver of pediatric patient) to evaluate for variations in participant report of trust in their own providers compared with trust in a child’s provider. Similarly, we stratified by healthcare setting to evaluate for differences in trust in providers based on participants being recruited from primary care versus emergency department sites. Data collection took place between July 2018 and February 2019, and analyses were completed between June 2021 and November 2022. All analyses were conducted using Stata 15.1.69
Results
Of the 1,771 adult patients and adult caregivers of pediatric patients who were approached for recruitment, 1,090 provided consent and initiated the survey. The final sample (n = 1,012) consisted of those who completed ≥50% of the survey questions, including the question about level of trust in providers (Appendix 1). 77% (n = 781) of participants were adult patients (Table 1). Participants identifying as non-Hispanic White made up the largest racial and ethnic group in the sample (n = 357, 37%), followed by Hispanic (n = 310, 33%), non-Hispanic Black (n = 207, 22%), and non-Hispanic multiple/other race (n = 83, 9%) participants. 77% (n = 755) of participants rated themselves or their child as being in good, very good, or excellent health.
Sample Characteristics by Level of Trust in Healthcare Provider
Twenty percent (n = 197) of participants were in the low/medium trust group. Participants had a median trust rating of 10/10 (interquartile range = 8 to 10). Those reporting low/medium trust in their or their child’s providers had a mean healthcare discrimination score of 1.65/7, compared with 0.57/7 for participants reporting high trust (P < .001) (Table 1). Participants identifying as non-Hispanic Black (n = 54, 26%) reported the highest percentage of low/medium trust in providers (P < .001) (Table 2). The highest percentage of any reported healthcare discrimination was among participants identifying as non-Hispanic multiple/other race (n = 32, 39%) (P = .012). Significant differences were noted among racial and ethnic groups when comparing each of the 7 types of healthcare discrimination experienced (Table 2). Participants identifying as non-Hispanic Black and non-Hispanic multiple/other race reported higher rates of experiencing each type of discrimination compared with non-Hispanic White and Hispanic participants. Across racial and ethnic groups, the most common type of discrimination reported was “felt like a doctor or nurse was not listening to what [they] were saying.”
Trust in Healthcare Provider and Experiences of Healthcare Discrimination by Race and Ethnicity
In the multivariable logistic regression model, participants with higher discrimination scores were less likely to report high trust in their providers (adjusted OR [aOR] 0.74, 95% CI 0.64, 0.85), whereas participants with good, very good, or excellent self-rated health were more likely to report high trust in providers (aOR 3.15, 95% CI 2.01, 4.92) (Table 3). The interaction term between healthcare discrimination score and having been screened for social risks in the past was statistically significant. Increased healthcare-based discrimination was associated with lower odds of high trust regardless of whether the participant had been screened for social risks. However, there was a difference in magnitude – the decrease in odds of high trust was smaller for those who had been previously screened (26% vs 6%, P = .026). In other words, with each 1-point increase in healthcare discrimination score (a higher level of reported discrimination), participants who had not been screened for social risks in a healthcare setting in the prior 12 months experienced a 26% lower odds of high trust (greater odds of low trust), whereas those who had been screened experienced 6% lower odds of high trust. Prior social screening by itself was not associated with trust.
Adjusted Associations Between High Trust in Healthcare Provider and Variables of Interest (n = 690)
In analyses stratified by race and ethnicity, the trends in associations between trust and discrimination, as well as between trust and self-rated health, were similar across groups (Table 4). In sensitivity analyses examining alternative cut points of the trust outcome, as well as stratification by type of participant (adult patient vs caregiver of pediatric patient) and healthcare setting (primary care vs emergency department), results showed consistent trends in direction and magnitude of associations (Appendix 3 Tables 1–8). Disaggregated descriptive statistics for Hispanic participants are displayed in Appendix 3 Tables 9 and 10.
Adjusted Associations Between High Trust in Healthcare Provider and Variables of Interest, Stratified by Race and Ethnicity
Discussion
In this study, we found that as patients and caregivers reported more types of healthcare-based discrimination, they were less likely to report high trust in their or their child’s providers. This finding is consistent with prior work on the relationship between healthcare discrimination and trust.26,27 We additionally found evidence that the negative association between discrimination and trust was different among patients who had previously received social risk screening, based on a significant interaction term coefficient.
Overall, trust in our sample was high. Although it is difficult to make direct comparisons to the level of trust found in other similar samples given variability in measures of patient trust reported in the literature, qualitative assessment of these studies suggests that our findings are substantively similar to what is published. Level of trust in healthcare providers differed significantly between racial and ethnic groups, with participants identifying as non-Hispanic Black or Hispanic reporting higher rates of low trust in their own or their child’s healthcare providers. Reporting healthcare discrimination was common in our sample; more than a quarter of participants reported at least 1 experience of discrimination. Previous estimates from studies with similarly diverse samples have ranged from 6% to 21%.70,71 We also found significant differences between racial and ethnic groups in terms of reporting experiences of healthcare discrimination, with participants identifying as non-Hispanic multiple/other race or non-Hispanic Black reporting higher levels of discrimination compared to the non-Hispanic White participants.
Prior research has demonstrated that trust in providers plays an important role in treatment adherence, use of preventive healthcare, and patient satisfaction.1⇓⇓⇓⇓–6,8⇓⇓⇓⇓⇓⇓⇓–16 The responsibility to build trust falls on individual providers, care teams, and healthcare systems, and there must be comprehensive system-wide efforts to improve trustworthiness.72 Given our finding that healthcare discrimination is associated with low trust, antiracist policies and programs should be evaluated as ways to improve trust alongside preventing and addressing healthcare discrimination. Many institutions have implemented individual-level interventions such as trainings in antiracism and cultural competence, however, multiple systematic reviews have found little to no evidence to support the idea that these programs impact healthcare workers’ behavior or patient outcomes.73⇓–75 Studies show that racial and ethnic concordance between patients and providers is associated with better communication,76⇓–78 as well as increased use of preventive care and decreased emergency department visits.79,80 Recent research, including qualitative studies of Black women’s reproductive health, has demonstrated the role of patient-provider racial concordance in facilitating trust and combating the effects of racism in healthcare.81,82 Thus, the recruitment and retention of more diverse providers may be 1 strategy for improving minoritized patients’ experiences and outcomes. This is the rationale for educational pipeline programs focused on diversity, for instance. Per Calliste and Dei, antiracism is “an action-oriented, educational and/or political strategy for systemic and political change that addresses issues of racism and interlocking systems of social oppression”; however, existing research is heavily weighted toward individual-level efforts.83 Evaluation of antiracism efforts should include both process and impact measures, at individual, care team, and organizational levels. In addition, evaluation should examine not only discrimination, but also associated factors, such as trust and health outcomes.
Study findings also suggest that being screened for social risks in healthcare settings may help build rapport and trust with patients’ healthcare teams, thus reducing the impact of prior discrimination. These findings align with the results of several recent studies of social resource interventions, in which screening and assistance with social needs was associated with more trust in, and better relationships with, providers.84⇓–86 Previously published findings from the parent study from which our data were derived also reported that patients/caregivers perceived value in screening for the purpose of making healthcare providers aware of their social context and did not expect the healthcare team to resolve their social needs.32 Similarly, in a separate study of adult patients who were screened for social risks, 43% wanted their healthcare team to be aware of their screening results, but did not expect assistance.87 This supports the idea that even in the absence of interventions, social screening may help to build trust, especially when delivered by personnel trained in empathic inquiry and trauma-informed approaches to screening.36 Universal social screening may provide opportunities to strengthen patient-provider relationships, beyond the goal of reducing social needs.88 It is notable that our dataset did not offer opportunities to examine more nuanced associations between trust and the context of social screening, however. It is possible that screening may exacerbate feelings of healthcare discrimination and/or worsen mistrust if not accompanied by adequate assistance, or if screening itself causes patients to feel stigmatized.89 Perceived failures in the process of providing assistance could also affect patient/caregiver willingness to engage with future screening and/or assistance programs. Future research might explore best practices for social screening across different patient populations.67 This research should prioritize examining both the intended and unintended impacts of screening, especially as it relates to trust and health equity. Factors such as patient-provider racial concordance, culture, nativity, and language may affect patients’ receptivity to answering screening questions.77,90
This study has several limitations. First, due to the cross-sectional study design, we were not able to assess the temporality of participants’ experiences of healthcare discrimination, or if/how their trust in providers changed in relationship to experiences of discrimination. Participants’ report of discrimination could have been influenced by their previous levels of trust. Although participants were asked about their trust in providers at the study site where they were completing the study survey, they were asked to report any prior discrimination across healthcare settings more generally. Regardless of setting, the survey did not assess care continuity. Care continuity should be assessed in future research as it may influence patients’ trust in their healthcare team or organization, as well as moderate/mediate the relationship between trust and self-reported experiences of discrimination.91,92 Similarly, we cannot establish temporality between experience of discrimination and screening for social risks. The healthcare setting at which participants were surveyed and asked about their trust levels may not have been the same setting in which they were screened for social risks. Study findings cannot be used to determine causation. Second, the study is subject to selection bias, given the convenience sample design, as well as social desirability bias. Dropout due to missing data may also have biased our study, likely away from the null. In addition, although we included a diverse set of primary care and emergency department study sites, findings may not be generalizable across settings. The use of a single aggregated Hispanic category and a single non-Hispanic multiple/other race category due to small sample sizes also limits generalizability and may mask differing levels of trust and differing experiences of discrimination within these groups. Participants were also limited to those who could speak and read English and/or Spanish. Finally, our study survey did not capture all known factors anticipated to influence trust and discrimination, for example, racial concordance between patient and provider team and care continuity. Future research should consider incorporating a wider set of key variables that can be used to more carefully understand and improve experiences of social care. Despite these limitations, study findings deepen our understanding of factors that may influence patients’ and caregivers’ trust in providers, as well as provide directions for future research.
Conclusions
Experiences of healthcare-based discrimination were associated with low trust in healthcare providers. These findings underscore the need for systemic antiracist interventions to prevent and address healthcare discrimination and improve healthcare system trustworthiness. In addition, a potential by-product of social screening in healthcare settings may be building rapport with patients, possibly reducing the impact of prior discrimination on trust. More research is needed on the relationship between social screening and trust, particularly as social screening programs are implemented more widely.
Acknowledgments
We thank the study sites and participants for sharing their time and experiences.

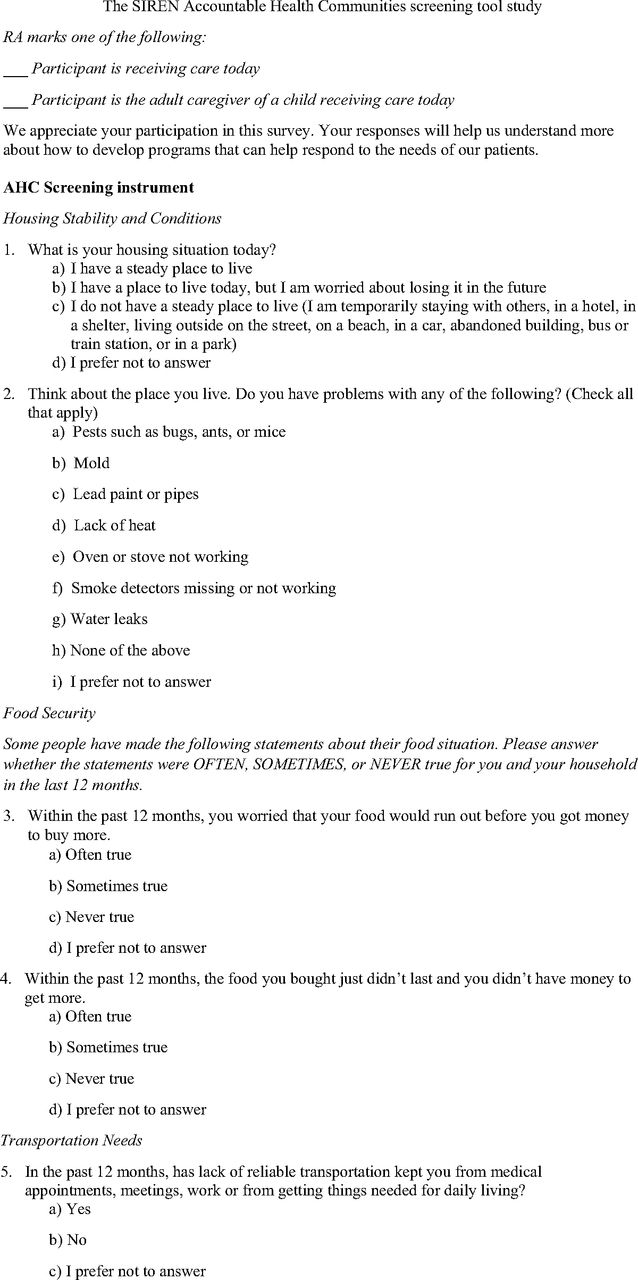
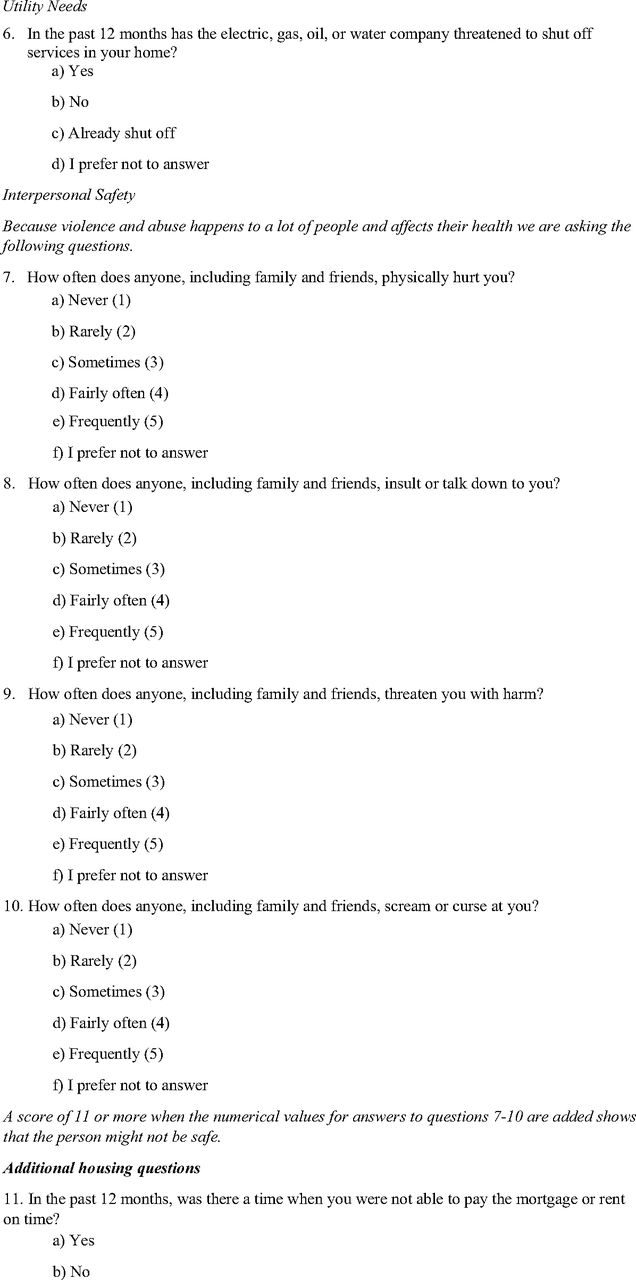
Appendix 2






Appendix 3
Adjusted Associations Between Complete Trust in Healthcare Provider and Variables of Interest (n = 690) (Sensitivity Analysis Using 1–9 vs 10 Cut Point)
Adjusted Associations Between Complete Trust in Healthcare Provider and Variables of Interest, Stratified by Race and Ethnicity (Sensitivity Analysis Using 1–9 vs 10 Cut Point)
Adjusted Associations Between High Trust in Healthcare Provider and Variables of Interest (n = 690) (Sensitivity Analysis Using 1–8 vs 9–10 Cut Point)
Adjusted Associations Between High Trust in Healthcare Provider and Variables of Interest, Stratified by Race and Ethnicity (Sensitivity Analysis Using 1–8 vs 9–10 Cut Point)
Adjusted Associations Between High Trust in Healthcare Provider and Variables of Interest (n = 690) (Sensitivity Analysis Using 1–7 vs 8–9 vs 10 Cut Point)
Adjusted Associations Between High Trust in Healthcare Provider and Variables of Interest, Stratified by Race and Ethnicity (Sensitivity Analysis Using 1–7 vs 8–9 vs 10 Cut Point)
Adjusted Associations Between High Trust in Healthcare Provider and Variables of Interest, Stratified by Participant Type (Original 1–7 vs 8–10 Cut Point)
Adjusted Associations Between High Trust in Healthcare Provider and Variables of Interest, Stratified by Healthcare Setting (Original 1–7 vs 8–10 Cut Point)
Characteristics of Disaggregated Hispanic Participants
Trust in Healthcare Provider and Experiences of Healthcare Discrimination Among Disaggregated Hispanic Participants
Notes
This article was externally peer reviewed.
Funding: The parent study was supported by The Commonwealth Fund (CWF) (award 20181338), a national, private foundation based in New York City that supports independent research on healthcare issues and makes grants to improve healthcare practice and policy. The views presented here are those of the author and not necessarily those of CWF, its directors, officers, or staff. CWF had no role in study design; collection, analysis, or interpretation of data; writing the report; or the decision to submit the report for publication. EHD was supported by a grant from the National Research Service Award (NRSA) (T32 HP19025). EB was supported by a grant from the National Institute on Minority Health and Health Disparities (NIMHD) (K23 MD015267). NJG was supported by a grant from the Health Resources and Services Administration (HRSA) (T32 HP42019). AJC was supported by a grant from the US Department of Veterans Affairs (VA), Health Services Research and Development Service (CDA 20-037). The manuscript’s contents are solely the responsibility of the authors and do not represent the official views of the CWF, NRSA, NIMHD, HRSA, or VA.
Conflict of interest: The authors have no conflicts of interest to report.
To see this article online, please go to: http://jabfm.org/content/37/4/607.full.
- Received for publication May 12, 2023.
- Revision received March 4, 2024.
- Accepted for publication March 11, 2024.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}