
Abstract
Background: The COVID-19 pandemic disrupted how primary care patients with chronic pain received care. Our study sought to understand how long-term opioid therapy (LtOT) for chronic pain changed over the course of the pandemic overall and for different demographic subgroups.
Methods: We used data from electronic health records of 64 primary care clinics across Washington state and Idaho to identify patients who had a chronic pain diagnosis and were receiving long-term opioid therapy. We defined 10-month periods in 2019 to 2021 as prepandemic, early pandemic and late pandemic and used generalized estimating equations analysis to compare across these time periods and demographic characteristics.
Results: We found a proportional decrease in LtOT for chronic pain in the early months of the pandemic (OR = 0.94, P = .007) followed by an increase late pandemic (OR = 1.08, P = .002). Comparing late pandemic to prepandemic, identifying as Asian or Black, having fewer comorbidities, or living in an urban area were associated with higher likelihood of being prescribed LtOT.
Discussion: The use of LtOT for chronic pain in primary care has increased from before to after the COVID-19 pandemic with racial/ethnic and geographic disparities. Future research is needed to understand these disparities in LtOT and their effect on patient outcomes.
- Chronic Pain
- COVID-19
- Healthcare Disparities
- Idaho
- Opioids
- Pandemics
- Primary Health Care
- Substance Use Disorders
- Washington
Introduction
After a brief decrease in drug overdose deaths, rates have increased again in the past 3 years rising to 106,699 deaths in 2021.1 These deaths have disproportionately affected racial and ethnic minorities.2 Changes in opioid prescribing may affect the risk for opioid overdose and other adverse outcomes. Preliminary studies reported an initial drop in opioid prescribing in the United States during the COVID-19 pandemic followed by a rebound after a few months.3 Meanwhile, use of nonpharmacologic modalities for chronic pain treatment decreased during the pandemic with a parallel increase in opioid prescriptions.4 Two scoping reviews, 1 from the US and 1 from Spain, found increased disparities in pain burden across marginalized groups and reports of poorly controlled chronic pain during the pandemic, which may been a result of changes in how clinicians managed chronic pain including through the prescription of opioids.5,6
The majority of patients with chronic pain receive their care from their primary care clinicians7 and primary care clinicians write almost half of all opioid prescriptions.8 A 2019 Virginia-based study on long-term opioid therapy (LtOT) in primary care found subgroup differences by gender, race and comorbidity in the likelihood of receiving prescriptions for LtOT.9 LtOT is not an evidence-based treatment modality for chronic pain and is one that can lead to increased risk for opioid risk.10 Understanding changes during the pandemic will help future interventions target improvements and improve equity in evidence-based chronic pain management and LtOT prescribing with the goal of reducing overdose risk.11 In our study, we sought to evaluate 1) the association between the COVID-19 pandemic and the likelihood of receiving LtOT in primary care among patients with chronic pain, and 2) whether the pandemic modified the association between demographic characteristics and the likelihood of receiving LtOT.
Methods
Using a retrospective observational design, we extracted electronic health record data from 64 primary care clinics across Idaho and Washington for patients who were 18 years of age or older, had a chronic pain diagnosis, and at least 1 primary care encounter in 1 of the 3 defined time periods. Each period was 10 months in duration: May 2019-February 2020 (prepandemic), March-December 2020 (early pandemic), and January-October 2021 (late pandemic). Patients with active cancer diagnoses were excluded. Our primary outcome was receipt of long-term opioid therapy (LtOT), which we defined as at least 3 consecutive months of receiving an opioid prescription. We obtained demographic characteristics from the electronic health record, calculated rurality using the Rural-Urban Commuting Area Codes12 and the Revised Charlson comorbidity from electronic health record diagnoses.13
We used descriptive statistics to describe patient demographic characteristics and burden of comorbidity by time period. We then used generalized estimating equations with exchangeable correlation structure to estimate (1) the odds ratio of receiving LtOT in the latter 2 time periods compared with the prepandemic period and (2) the 2-way interaction between time period and each demographic characteristic. We fit a separate interactive effect model with logit link function regarding each demographic factor, adjusting for the main effect of all other variables. Statistical analyses were performed using R version 4.1.2. The University of Washington Institutional Review Board approved this study.
Results
In our sample, 28,325 patients had a diagnosis of chronic pain in the prepandemic period, 22,079 during the early pandemic and 21,016 in the late pandemic. Of those, 5.3% (n = 1,513) received LtOT prepandemic, 5.3% (n = 1,176) early pandemic and 5.9% (n = 1,248) late pandemic. Table 1 describes the characteristics.
Characteristics of Patients with Chronic Pain Related Diagnoses and Long-Term Opioid Therapy Prescriptions
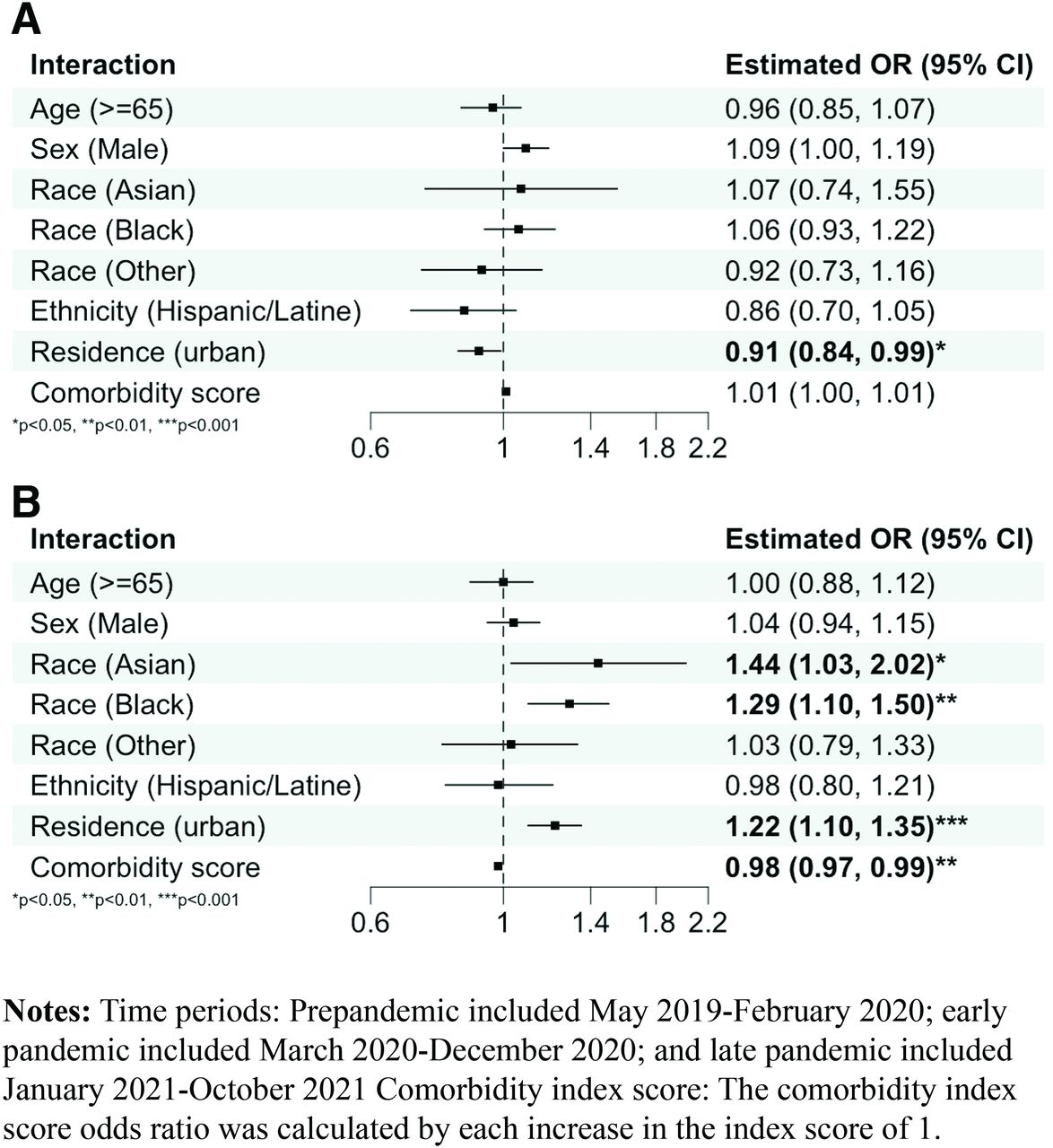
In our generalized estimating equations analysis, we found a decrease in the proportion of those with a chronic pain diagnosis who received LtOT prescription in the early pandemic period (OR = 0.94, P = .007) followed by an increase in late pandemic (OR = 1.08, P = .002), adjusting for age, sex, race, ethnicity, rurality, and comorbidity index. In the 2-way interactions, comparing the early pandemic versus prepandemic period, those living in urban areas had lower odds than those in rural areas to be prescribed LtOT (OR 0.91, P < .05) (Figure 1). Comparing the late pandemic versus prepandemic period, patients identifying as Asian (OR = 1.44, P < .05) or Black (OR = 1.29, P < .01) had a higher odds compared with those identifying as White to be prescribed LtOT. Furthermore, those living in urban (compared with those living in rural areas) (OR = 1.22, P < .001) and those with lower comorbidities scores (OR = 0.98, P < .01) had higher odds of receiving LtOT comparing the late pandemic versus prepandemic period.

Two-way interactions between (A) early pandemic versus prepandemic and (B) late pandemic versus prepandemic and patient demographic characteristics for receipt of long-term opioid therapy.
Discussion
Our study found that the likelihood of receiving LtOT with a chronic pain diagnosis increased since the onset of the pandemic. While the changes in LtOT receipt are statistically significant, their clinical meaning may be negligible given the small odds ratios. However, we did find specific patient subgroup disparities in this change such as in race and geographical region of residence that had higher odds ratios than the overall. This disparity for Black patients was previously reported prepandemic,9 although there are mixed reports of opioid prescribing for Black patients,14 and our study found rates continues to rise for LtOT in comparison to White patients from pre to late pandemic along with higher rates of overdose.2 The increase of LtOT prescribing for Asians through the pandemic has not previously been reported, potentially due to insufficient number of Asians and the collapse of the Asian race into the Other category in many other studies. This increase is concerning in light of recent reports that Asians have substantially increased rates of substance use disorder compared with White individuals from pre- to late pandemic.15 More research is needed to elucidate the reasons why these disparities have worsened for Asian and Black subgroups since the pandemic.
Meanwhile, initial decrease in LtOT in the early pandemic followed by an increase in the late pandemic for patients living in urban areas (compared with rural) also merits further study. Finally, compared with the 2019 primary care study on LtOT prescribing where patients with higher comorbidities were more likely to receive LtOT,9 our study found that those with higher comorbidities were less likely to receive LtOT, suggesting that primary care clinicians are heeding guidelines that caution against LtOT for patients with higher risks for harm.
Our study has several limitations. First, since our data are from clinics in 2 states in the Pacific Northwest, it may not be generalizable to all populations in the US although the 2 states included provide a diversity of race/ethnicity and rurality to minimize this. Second, since we used retrospective data, causality cannot be inferred including whether the COVID-19 pandemic was the primary driver of these changes. Third, we looked at any opioid prescribing and not opioid dosing and, as such, may not be able to elucidate disparities in opioid dosing. Fourth, since we only included those with chronic pain in our sample, there may be a selection bias.
Conclusions
The use of LtOT for chronic pain in primary care has increased from before to after the COVID-19 pandemic. Further studies are needed to understand disparities in receipt of LtOT and to develop interventions to improve health equity related to chronic pain management and LtOT prescribing for subgroups affected by these disparities.
Notes
This article was externally peer reviewed.
Funding: This study was supported by the National Institute on Drug Abuse (UG1DA013714) and the National Center for Advancing Translational Sciences (UL1TR002319). Dr. Anastas’ time on this study was supported by an institutional training grant from the National Institute of Mental Health (T32MH020021).
Conflict of interest: None.
To see this article online, please go to: http://jabfm.org/content/37/2/290.full.
- Received for publication October 3, 2023.
- Revision received November 18, 2023.
- Accepted for publication November 27, 2023.




{kind=link}