
Abstract
Purpose: In efforts to improve patient care, collaborative approaches to care have been highlighted. The teamlet model is one such approach, in which a primary care clinician works consistently with the same clinical staff member. The purpose of this study is to identify the characteristics of high-performing primary care teamlets, defined as teamlets with low rates of ambulatory care sensitive emergency department (ACSED) visits and ambulatory care sensitive hospital admissions (ACSAs).
Methods: Twenty-six individual qualitative interviews were performed with physicians and their teamlet staff member across 13 teamlets. Potentially important characteristics related to high-performing primary care teamlets were identified, calibrated, and analyzed using qualitative comparative analysis (QCA).
Results: Key characteristics identified by the QCA that were often present in teamlets with low rates of ACSED visits and, to a lesser extent, ACSAs were staff proactiveness in anticipating physician needs and physician-reported trust in their staff member.
Conclusion: This study suggests that physician trust in their staff and proactiveness of staff in anticipating physician needs are important in promoting high-performing teamlets in primary care. Additional studies are indicated to further explore the relationship between these characteristics and high-performing teamlets, and to identify other characteristics that may be important.
Introduction
Many practices focus on establishing teams in which primary care physicians work closely with nurse practitioners, nurses, medical assistants, and others to care for patients.1,2 Teams may be difficult and expensive to create; the concept of “teamlets”—dyads composed of a primary care clinician and 1 other staff member (most often a medical assistant) who work together most of the time—has emerged as a simpler, less expensive alternative to teams.3–6 Teamlets may exist on their own or within a health care team.
Anecdotally, teamlets have long been common in primary care (though the term emerged only recently), but there is little research aimed at identifying characteristics of high-performing teamlets.7–9 In previous work, we found that /77% of primary care physicians reported working together with 1 staff member at least 80% of the time.10 In this study, we seek to identify the characteristics or combinations of characteristics most common in high-performing teamlets by linking Medicare claims data to physician survey and interview data with teamlet physicians and staff members.11–14
Methods
Overview
We used QCA to analyze the relationship between teamlet characteristics and being a high-performing teamlet (defined as those with a lower proportion of their patients having ambulatory care sensitive emergency department (ACSED) visits, ambulatory care sensitive hospital admissions (ACSAs), or both). We selected these outcomes because high quality outpatient care may reduce the ACSED visit and ACSA rates.15,16 QCA is an analytic technique that can quantitatively analyze qualitative data – even when the number of cases is relatively small13, 17 – to determine the characteristics or combination of characteristics most commonly associated with a given outcome.
Sample and Interviews
As described previously,10 we randomly sampled 2300 general internists and family physicians drawn from the nationwide Care Precise database. Selected physicians were sent a survey to determine whether they worked with the same staff member in at least 80% of clinic sessions and, if so, to characterize the physician’s perspectives on the positive and negative aspects of working this way (Appendix 1).
An invitation to participate in a 30-minute qualitative interview (via Zoom) was sent to the 533 physicians who reported working in a dyad). Twenty-one physicians and their respective staff member participated in interviews conducted from 2020 to 2021. Eight of these 21 teamlets were excluded because the physician had not worked with their current staff member during the 2019 period for which quantitative data were available or because, by the time of the interviews, they were working mostly in nonprimary care practice. Interviews were conducted with physicians and staff in the 13 remaining teamlets confidentially and separately using a semistructured qualitative interview protocol focused on understanding the working relationship of the teamlet (Appendices 2 and 3). Each participant received a small stipend.
Analysis
Each interview was coded by 2 researchers (MC and EO) using Atlas TI version 8.4.4 to identify potentially important characteristics of teamlets. Before analyzing the data using QCA, these characteristics were refined based on the extent to which the themes arose in interviews and in physician survey responses, and were reviewed and agreed on by the entire study team. QCA requires all data to be “calibrated” before analysis,11 which involves locating cases on a 0.0 to 1.0 scale, where 1.0 indicates that the characteristic under consideration is fully expressed and 0.0, that it is not expressed. Scores within the 0.0 to 1.0 range indicate that the characteristic is partially expressed. Calibrations were performed by MC and EO to assign a scaled numeric score indicating the extent to which the characteristic was expressed based on interview and survey responses (Table 1). Coders and the team were blinded to teamlets’ performance until after coding and calibrations were completed.
Calibration Details for Characteristics Based on Interview and Survey Data
Teamlets with sicker patient panels may have higher rates of ACSED visits and ACSAs even with good outpatient care, so we calculated, for each teamlet, observed-to-predicted ratios of their ACSED visits and ACSAs respectively from 2019 Medicare claims data. The observed values were the actual ACSED visit and ACSA rates among patients attributed to the teamlet, and the predicted values were derived using a risk adjustment model with patient age, gender, dual-eligible status, race (white, black, other) and Centers for Medicaid and Medicare Services Hierarchical Condition Category score as predictors. A lower observed-to-predicted ratio of either ACSED visit or ACSA rates suggested that the teamlet had achieved a lower rate of adverse events given their patient risk profile. We also used the average of these 2 ratios as an additional composite outcome measure.
We then conducted a QCA using the software packages Kirq (https://grundrisse.org/qca/kirq/) and fs/QCA (https://sites.socsci.uci.edu/∼cragin/fsQCA/software.shtml) to identify patterns of characteristics associated with low observed-to-predicted ACSED visit and ACSA rates using sufficiency analyses, following the protocol outlined by Rihoux and Ragin.13 Details of the calibrations are presented in Table 1. The 3 outcomes were calibrated using the direct method;13 the explanatory characteristics were manually calibrated as detailed in Table 1. The manual calibrations were determined collaboratively, with each teamlet’s score being reviewed by the research team.
Necessity testing identified no characteristics as necessary for realizing any of the outcomes with a necessity consistency score of ≥ 0.9. For the sufficiency analysis, the complex solution11 is presented, using the rule that both raw (configuration) consistency and PRI (proportional reduction in inconsistency) consistency must equal or exceed 0.75 for determining a configuration to be sufficient for realizing the outcome.
Results
Teamlets practiced in a variety of outpatient settings in different geographical areas of the United States, and included physician-owned practices and hospital/health system-owned practices. They encompassed solo primary care practices along with practices with up to 12 physicians.
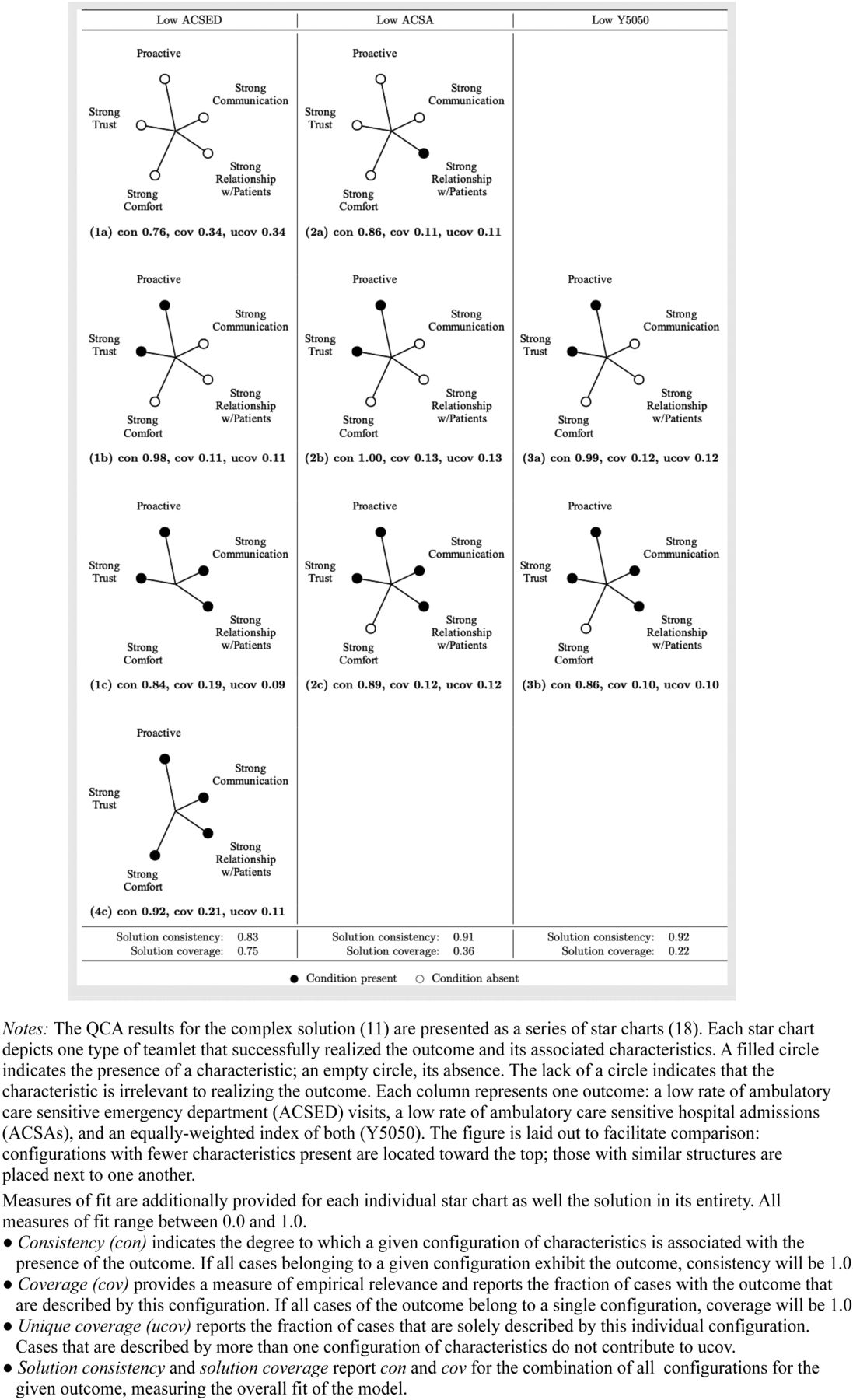
We found a pattern of characteristics in teamlets that had low ACSED visit rates and, to a lesser extent, low ACSA rates or low composite ACSED visit and ACSA rates (Figure 1). Specifically, high performing teamlets had high levels of staff proactiveness in anticipating physician needs and high levels of physician-reported trust in the staff member. Good relationships between the staff member and patients, good communication between the staff member and physician, or both were also often present. Four out of the 8 teamlets with low ACSED visits did not have any of these relationship-related characteristics.

Star chart of teamlet types with low rates of ambulatory care sensitive emergency department visits and hospital admissions.
Figure 1 presents the results of the QCA as a series of star charts,18 depicting those combinations of characteristics associated with (a) low ACSED visit rates, (b) low ACSA rates, and (c) low ACSED visit rates and low ACSA rates. (A truth table detailing the sufficiency analysis is included in Appendix 4.) Table 2 shows key characteristics identified in the QCA along with sample quotes associated with each characteristic, taken from interviews with physicians and their teamlet staff member.
Key Qualitative Comparative Analysis Characteristics and Sample Quotes from Qualitative Interviews
Discussion
Primary care teamlets may be a simple and inexpensive way to improve primary care, but the characteristics and combinations of characteristics common in high-performing teamlets have not been identified. Our analysis found that 2 characteristics – physician-reported trust in the staff member and high levels of staff proactiveness in anticipating physician needs – were more likely to be present in high-performing teamlets. Good relationships between staff members and patients and good communication between staff members and physicians were present in some high-performing teamlets, suggesting that 1 does not need to have a picture-perfect teamlet to realize benefits.
This study has limitations. First, it is possible that teamlets with strong working relationships between their members were more likely to participate. This may have led to less variation between teamlets on the presence or absence of relationship-related characteristics.
Second, the number of participating practices was relatively small despite multiple rounds of recruitment mailings and phone calls, and the practices in the study may not be representative of the wide range of practices in primary care. Recruitment for the study coincided with the beginning of the Coronavirus pandemic, which may have made physicians and staff members less likely to participate due to difficulty contacting physicians and staff (because some may have been working remotely), increased staffing changes and turnover, and increased practice workloads. Nevertheless, QCA is a useful tool for identifying patterns in data with a small sample size.13,17
Four of the high-performing teamlets did not conform to any of the explanatory recipes identified by our QCA, indicating that there are other combinations of characteristics that can produce high-performing teamlets in addition to those we identified. Identifying these additional pathways to high-performing teamlets is a subject for future research. Future research is also warranted to evaluate further whether staff proactiveness in anticipating physician needs and physician trust in their staff member are related to high-performing primary care teamlets and to expand on our initial studies by exploring whether staff trust in physicians and staff proactiveness in meeting patient needs are also important. Such research should also investigate whether additional factors are instrumental to high-performing teamlets. Through these additional studies, interventions to support strong and sustained teamlet relationships can be developed, such as efforts to foster staff proactiveness and to reduce staff turnover.
Acknowledgments
We would like to thank Rachel Willard-Grace, MPH for advice during the design and conception of the study. We also thank the American Academy of Family Physicians (AAFP) and the American College of Physicians (ACP) for letters of support that we included in survey materials mailed to physicians. Neither the AAFP nor ACP had any role in the design or interpretation of the study.
Appendices.Appendix 1. National Survey of Primary Care Physicians
Appendix 2. Physician Interview Protocol
In responding to our questions, please tell us about how things worked in your teamlet before the COVID-19 epidemic. But if you have something to add about how things have been during the epidemic, please do not hesitate to tell us.
Can you tell us about a time that [name] was particularly helpful with a patient or patients?
In your survey that you completed {give an approximate date}, you said you work with the same staff partner at least __% of the time [will customize to the respondent since we will read the individual’s survey responses before doing the interview]. Is that still true?IF NOT STILL TRUE:
Ask whether there is someone new that the physician works with and about what % of time works with that person.
Regardless of the percent time, continue with the interview as it stands below, asking about the current partner, but toward the end of the interview ask why the physician switched staff members.
3. We are seeking to understand more about your experiences working consistently with one staff person. Could you tell us a little bit about your working relationship with your staff partner? How has it evolved over time?
4. How well do you feel that [name] knows your patients and has a trusting relationship with them?
Probe: (If they do feel there is such a relationship):
Can you tell me about a time when this knowledge of your patients/trusting relationship with your patients (or lack thereof) made a real difference?
5. What is the best thing about working with [insert staff member’s name]?
Probe: can you give us an example?
6. What is the most difficult thing about working with [insert staff member’s name]
Probe: can you give us an example?
7. What are some things that you wish your staff partner could do but which they do not currently do? Why don’t they do these things?
Probe:
government regulations
union rules
staff member’s access to the EHR
documentation issues
any others?
8. Do you prefer to work with one staff member consistently or would you prefer to work with different staff members on different days?
a. Probe: Why?
9. You answered in your survey that you have (“a great deal of influence/some influence/very little influence/no influence” – customize based on response to survey Q9) over selecting the staff member with whom you work most frequently. Can you tell us more about how you are involved in the hiring of this staff member?
Probe: Are you satisfied with the extent of involvement you have in hiring the staff member with whom you work most frequently? Why or why not?
10. Do you consider that you and [staff member name] are a small team within a larger, formally defined team that includes other staff members as well?Probe if YES:
How important to you is the small team (you and NAME) vs. the larger team? Can you explain?Probe for examples.
b. If no longer working with the same staff member, ask: Can you give us a sense of why you stopped working with the previous staff member?
11. In the survey, you mentioned that staff turnover was a [major barrier/minor barrier/not a barrier]. Can you tell me more about this?
Probe: Is this a problem for you or your practice? If not, what have you been able to do to keep MAs in your practice?
12. What advice would you offer a younger colleague about working with a clinical staff partner such as a medical assistant? What do you think is most important to making that relationship effective?
13. How do you imagine that the COVID-19 pandemic may change the role of and your relationship with your clinical staff partner in the long term?
14. Is there anything else that you would like to add? Is there anything we haven’t asked you that we should be asking?
Appendix 3. Staff Interview Protocol
In responding to our questions, please tell us about how things worked in your teamlet before the COVID-19 epidemic. But if you have something to add about how things have been during the epidemic, please do not hesitate to tell us.
Can you tell me about a time when you and Dr. X worked particularly well to look after a patient?
About how long have you been working with Dr. X? (make sure worked with doctor during entire 2019)
About what percent of your time do you work with Dr. X?
Has your working relationship with Dr. X evolved over time? Probe: If so, how has it evolved?
What do you think are the two most valuable things that you do to help Dr. X and his/her patients?
Could you tell us about a time that you worked particularly well together with Dr. X to take care of a patient’s needs?
Did your practice give you additional training so that you can provide more help to Dr. X and his/her patients?
a. Probe:
i. If not described, ask the interviewee to tell you a bit about this additional training.
Are there responsibilities that you would like to take on, but that you can’t do because of legal, union, or other barriers?
What is the best thing about working with Dr. X?
a. Probe: can you give us an example?
What is the most difficult thing about working with Dr. X?
a. Probe: can you give us an example?
Do you prefer to work with one physician consistently or would you prefer to work with different physicians on different days?
a. Probe: Why?
We’d like to ask you a question about burnout, and whether you feel burned out from your work. Do you feel burned out: [Note: if the interviewee asks what we mean by burn out, tell them to use their own feeling of what it means to be burned out.]
Frequently
Occasionally
Never or almost never
Do you consider that you and [Dr. X] are a small team within a larger, formally defined team that includes other staff members as well?
Probe if YES:
a. Does the larger team help you and Dr. X take better care of patients?
b. Probe:
1. If yes, give an example.
2. If no give an example
What are the most positive things about your job that entice you to stay?
What advice would you offer a younger colleague about working with Dr. X? What do you think is most important to making that relationship effective?
How do you imagine that the COVID-19 pandemic may change the role of and your relationship with your clinical staff partner in the long term?
Is there anything else that you would like to add? Is there anything that we haven’t asked you that we should be asking?
Appendix 4.Truth Table.
Notes
This article was externally peer reviewed.
Funding: This work was supported by a grant from the U.S. Agency for Healthcare Research and Quality (AHRQ) 5 R01 HS025716-03.
Conflict of interest: None.
To see this article online, please go to: http://jabfm.org/content/37/1/105.full.
SECTION: Brief Report
COVER/FOOTER: High-Performing Teamlets in Primary Care
- Received for publication March 17, 2023.
- Revision received August 18, 2023.
- Accepted for publication September 5, 2023.




{kind=link}