
Abstract
Background: A rising population of cancer survivors is accompanied by a shortage of oncologists for continuity of care. This study examined the physicians who provided most of the care for cancer survivors, along with written information provided to the survivors before transfer of care.
Methods: Data were collected through the CDC-sponsored Behavioral Risk Factor Surveillance System. Our analysis involved states whose respondents completed a cancer survivorship module from 2016 to 2020. Primary measures were the proportions of physician specialists who provided most of their subsequent health care and the proportions of survivors who received written summaries of their care and instructions.
Results: The 36,737 cancer survivor respondents came from 33 states. Most of their health care came from primary care physicians [family physicians (42.3%, 95% CI: 41.3–43.2%) and general internists (26.0%, 95% CI: 25.2–26.9%)]. When seen by primary care physicians rather than subspecialists, a lower proportion of patients recalled receiving summaries of either their cancer treatments (44.3%, 95% CI: 42.5 to 46.2 vs 50.5%, 95% CI: 49.4 to 51.7%) or follow-up instructions (69.9%, 95% CI: 68.8 to 71.0% vs 78.7%, 95%CI 77.1 to 80.2%), regardless of their cancer type.
Conclusions: Regardless of their cancer type, two-thirds of survivors received most of their health care from primary care physicians. Collaborative community-based care within a shared decision-making framework is essential to prioritize and individualize patients' understandings and needs in this growing population.
- Behavioral Risk Factor Surveillance System
- Cancer Survivors
- Continuity of Patient Care
- Data Analysis
- Delivery of Health Care
- Primary Care Physicians
- Primary Health Care
- Workforce
Introduction
The population of persons who continue to function and prosper despite setbacks from cancer is rising in the United States1⇓–3 This upsurge is accompanied by a shortage of oncology services for the continuity of care after treatment.4, 5 More than a decade ago, the Institute of Medicine released a report charting a pathway for providing care to cancer survivors by transitioning patients back to primary care providers.6 It remains unclear who is providing follow-up care for cancer survivors and whether this need should be prioritized or integrated into primary care.7
Specialist-driven models of cancer care and discordance between expectations about the roles of the oncologist and primary care physician created further barriers to collaboration.8 The lack of a universal definition for cancer survivors may have contributed to the uncertainty as to when primary care should resume responsibility for these patients.6, 9⇓⇓–12 In the meantime, reports from a few states revealed that primary care physicians eventually provided most of the general health care for cancer survivors.13⇓⇓⇓⇓–18
The objective of this investigation was to more comprehensively examine the physicians who provided most of the care for cancer survivors. Perhaps the best means of better understanding this issue is to review state-specific telephone surveys of cancer survivors conducted by the Behavioral Risk Factor Surveillance System (BRFSS).19,20 A more well-informed patient is likely to seek care and focus on their well-being.21 Using these data, we also examined the patient's recall of written information that they received about their treatment and follow-up instructions before seeing their physician for continuity of care.
Methods
Conduct of the Survey
The BRFSS survey was developed and approved by the CDC institutional review committee.22 This premier national system of health-related telephone survey provided state-specific data from a representation of their citizens' health-related risk behaviors, chronic health conditions, and use of preventive services. The data were publicly available without any personal identifiable information. For this reason, our institutional review board granted exemption for conduct of the study.
Provision of a standardized questionnaire and technical and methodologic assistance from the CDC were used to collect prevalence data. The survey had two primary components: (1) core modules which were sets of questions consistently administered at all states and territories to establish national estimates, and (2) optional modules that the CDC developed depending on priorities identified by individual states.
Several state health departments electively chose the optional cancer module, because it was especially relevant to their residents' needs.
Surveys were conducted by telephone calls only. With technical and methodological assistance from the CDC, state health departments either used in-house interviewers or contracted with telephone call centers or universities. All interviewers were trained how to administer the BRFSS surveys throughout the year in the same straight-forward manner. Survey interviewees in each state were selected using Random Digit Dialing (RDD) techniques on both landlines and cell phones. Inclusion criteria of interviewees were noninstitutionalized adults aged 18 years or older who were current residents of state from which their telephone number was selected. There were no exclusion criteria.
The BRFSS median combined landline and cellphone survey response rate for all states, territories and Washington, DC, in 2020 was 47.9% and ranged from 34.5% to 67.2%. Response rates for states included in this analysis had a median of 49.8% and ranged from 30.7% in Louisiana in 2016 to 67.2% in Mississippi in 2020.23⇓⇓⇓–27 If the state resident elected to not be interviewed, then the next randomized person was called until the desired minimum number of interviewees was obtained from representative regions of the state. Respondent demographic data included age, sex, race/ethnicity, education, household income, health plan, and general health status. We collapsed general health status into good or excellent, fair, or poor, and unknown categories. A respondent's health plan was recorded as “yes” or “no” depending on whether that person had any insurance.
Responses from Cancer Survivors
A question in the core module was whether the interviewee had any type of cancer in the past. Beginning in 2009, an optional module entitled “cancer survivorship” was introduced in the BRFSS. The optional module questions were asked of respondents who had been treated for cancer and were survivors (lived after treatment). These questions included the respondent's age at the time of diagnosis and the type(s) of cancers. The BRFSS grouped the 10 major cancer types:20 (1) breast, (2) female reproductive (includes cervical, endometrial, and ovarian), (3) head/neck cancer (includes head and neck, oral, pharyngeal, thyroid, and larynx), (4) gastrointestinal (colon, esophageal, liver, pancreatic, rectal, and stomach), (5) leukemia/lymphoma (Hodgkin's lymphoma, leukemia, and non-Hodgkin's lymphoma), (6) male reproductive cancer (prostate and testicular), (7) skin (melanoma, basal cell, squamous cell, Merkel), (8) thoracic (heart and lung), (9) urinary (bladder and renal), and (10) other (bone, brain, neuroblastoma, and other).
We chose the most recent 5 years (from 2016 to 2020) to allow for a large number of respondents representing state health departments requesting examination of the cancer module survey results. Cancer survivors were asked the types of physicians who provided most of their subsequent health care. We classified the type of doctor as being either a primary care physician (family physician and general internist) or subspecialist (cancer surgeon, general surgeon, gynecologic oncologist, plastic surgeon/reconstructive surgeon, medical oncologist, radiation oncologist, urologist, and other nonprimary care physicians). Respondents were asked to recall whether they received a written summary of their cancer treatment and any written instructions for follow-up care.
Statistical Analysis
The state-specific data were collected by the CDC. We calculated the proportions of respondents and associated 95% confidence intervals (CI) by recall of physician type and written reports. The likelihood to visit a primary care physician or subspecialist was compared using the respondent's demographic characteristics, health care access, and general health status. We considered data as being unreliable if the numerator of a proportion was less than 50 or if the relative standard error was more than 30% of the estimate.
Each state in the study sample had responses from cancer survivors for 1 or more of the years. The probability of a survivor being surveyed more than once was very low as participation is random, anonymous, and confidential and samples used in the BRFSS must be probability samples in which all households with telephones have a known, nonzero chance of inclusion. Furthermore, for states participated more than 1 year in the cancer survivorship module during the study period, we reweighted the response based on respective sample sizes in each year. Then we pooled the reweighted cancer survivorship module data of these states to produce a large sample for analysis. We reported weighted estimates to balance data in the calculation of means, proportions, and confidence intervals.
We used the Rao-Scott c2 for test of association between categorical variables. The Rao-Scott c2 statistic was computed from the Pearson c2 statistic and a design correction based on the design effects of the proportions. All P values were 2-sided, and a P < .05 was statistically significant. We conducted statistical analyses with SAS 9.4 software and R 4.1.2.
Results
During this 5-year period, 65,958 (or 11.9%, 95% CI: 11.7 to 12.0%) respondents to the core module in 33 states stated that they had cancer while 322,640 (or 88.1%, 95% CI: 88.0 to 88.3%) did not. A total of 59,324 persons participated in the cancer survivorship modules, and 36,737 of respondents were survivors who completed cancer treatment by the time of interview. Most respondents had only 1 type of cancer (72.5%, 95% CI: 71.6 to 73.4%), and few had 3 or more (2.6%, 95% CI: 2.3–3.0%). Types of cancers among the survivors were in the following order from most to least common: skin, breast, male reproductive, female reproductive, gastrointestinal, head and neck, leukemia/lymphoma, urinary, and thoracic.
The age at the time of cancer diagnosis was often between 45 to 64 years, and the survey was conducted 11.7 ± 10.6 (S.D.) years since first diagnosis of cancer. Slightly more than half (56.3%, 95% CI: 55.3 to 57.2%) were female, and most respondents (86.4%, 95%CI: 85.6 to 87.1%) were non-Hispanic white. Most considered themselves to be in good-excellent health (76.1%, 95% CI: 75.2 to 76.9%) and had health care coverage (96.6%, 95% CI: 96.2 to 96.9%). The household income was usually $50,000 or higher. Their education level was evenly distributed between being high school graduates or less (36.4%, 95% CI: 35.5 to 37.4%) and college graduates or more (31.4%, 95% CI: 30.6 to 32.2%).
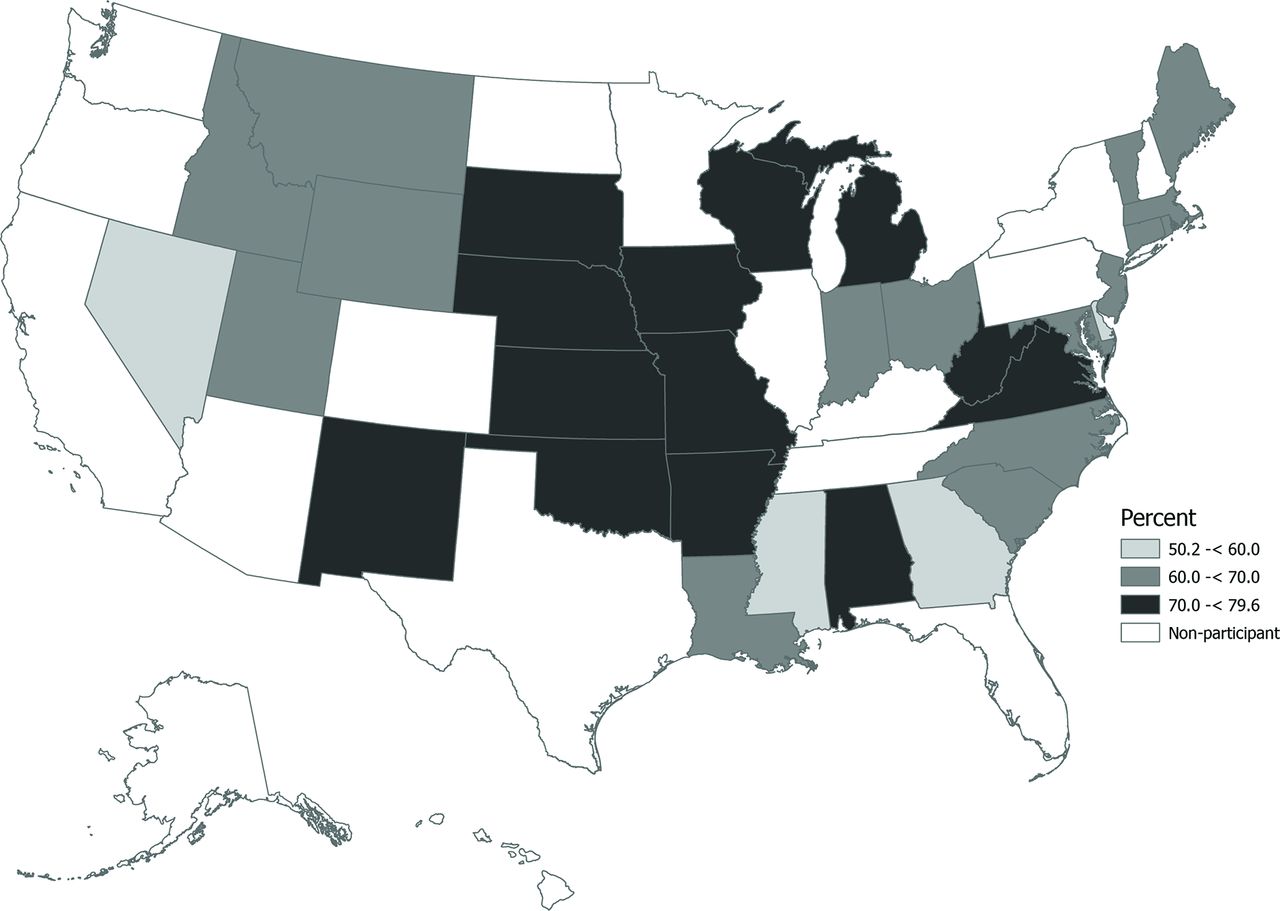
Approximately two-thirds of cancer survivor respondents (68.3%, 95.0% CI: 67.4 to 69.2%) indicated that primary care physicians provided their subsequent health care. Those consisted of family physicians (42.3%, 95% CI: 41.3 to 43.2%), general internists (26.0%, 95% CI: 25.2%–26.7%), and subspecialists (28.4%, 95%: 27.5 to 29.3%). Figure 1 displays the 33 states participating in the cancer survivorship module. In each state is shown the percentage of physicians providing care to cancer survivors who were primary care physicians. The highest percentage of primary care givers were in less densely populated and less urban states.
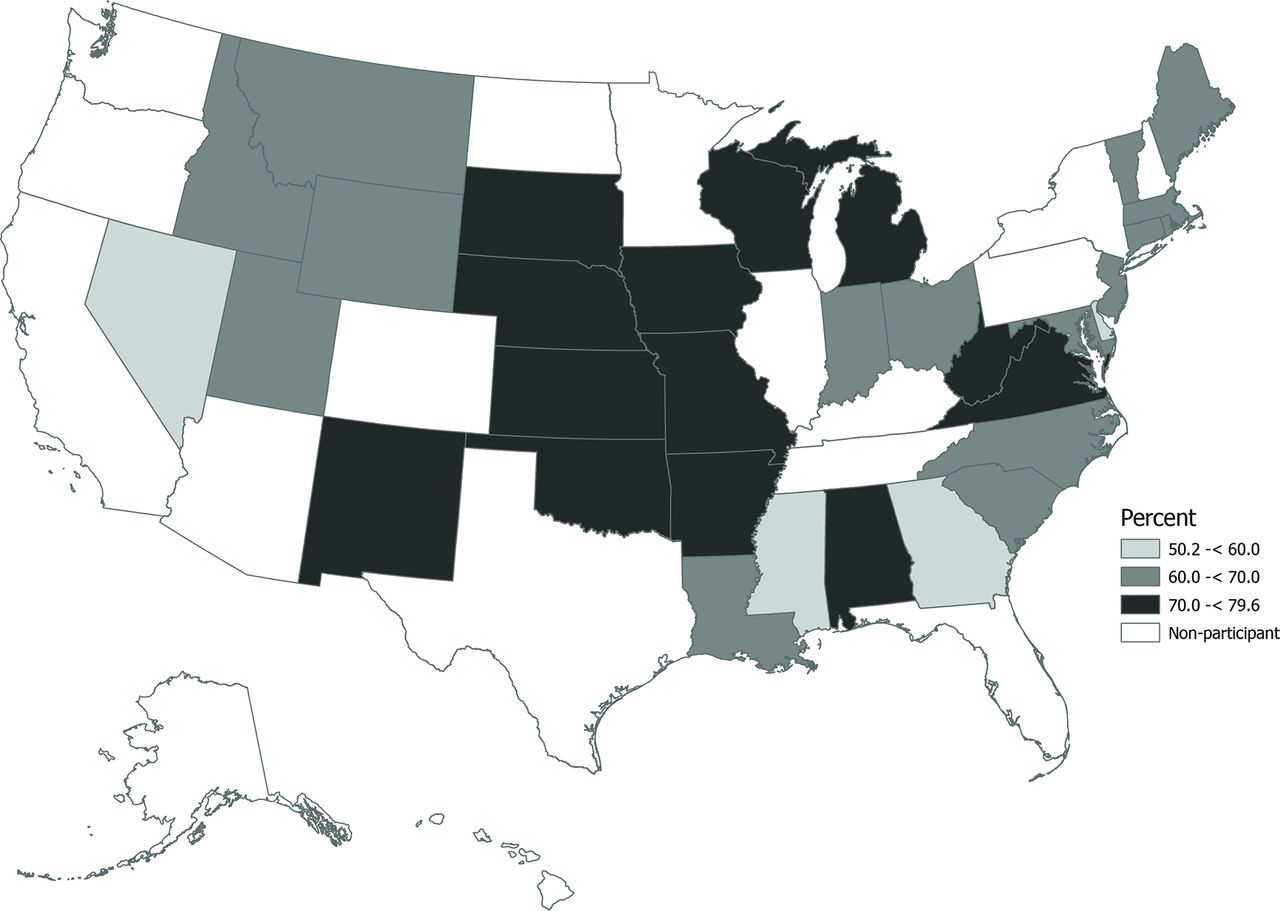
Proportion of cancer survivors seeking health care from primary care physicians of the 33 states participating in the optional Behavioral Risk Factor Surveillance System (BRFSS) cancer survivorship module, 2016 to 2020.
The physician group most involved with patients according to the cancer type is shown in Table 1. Primary care physicians were more likely to see survivors with skin, breast, female reproductive, and male reproductive cancer. Subspecialists provided continuity of care if the survivor had a less common cancer (eg, leukemia/lymphoma, thoracic, head/neck). Regardless of cancer types, states, or years (data not shown), primary care physicians provided the majority of health care for cancer survivors.
Types of Physicians Providing Care for Survivors by Cancer Type, 2016 to 2020
Less than half (44.2%, 95% CI: 44.3 to 45.2%) of all survivors recalled being given written summaries of their treatment. Receipt of summaries was lower under the following conditions: if there had been 3 or more cancers, were currently 75 or older, were Hispanic, had a lower income, and were less educated. More recalled receiving written instructions of care (72.0%, 95% CI: 71.2 to 72.9) if their current age was less than 75 years, their income was higher, or their education was higher.
Compared with those who received care by subspecialists, survivors seeking care from primary care physicians were more inclined to not recall whether they received written comments about their cancer treatment (44.3%, 95%CI: 42.5 to 46.2 vs 50.5%, 95% CI: 49.4 to 51.7%; P < .001) and their follow-up instructions (69.9%, 95% CI: 68.8 to 71.0% vs 78.7%, 95% CI: 77.1 to 80.2%; P < .001). This finding did not vary depending on whether the primary care provider was a family medicine physician or general internist.
Discussion
A workforce shortage in oncology, combined with an exponentially increasing number of cancer survivors, has reduced the sustainability of a specialist-based model of care.5,28 This study examined physicians who provided continuity of care for cancer survivors. Our findings showed that 2-thirds of cancer survivors sought their maintenance of care from either a general internist or usually a family physician. This group was more inclined to assume the continued care of survivors whose cancer was common. Survivors who did not recall receiving any written summaries or instructions were more often to seek care from primary care physicians.
Recognizing findings in the present study, more will need to be done to encourage consistent communication between the oncology team, physician to whom care is transferred, and the engaged patient. Risk stratification and delineation of care could further define the physician's role, preferably before and at the end of treatment and after transfer of care.7 For example, patients with an early stage of a common cancer (eg, breast, colorectal, or prostate cancer), those undergoing standard treatment, are senior, or with comorbid medical conditions are often transitioned to community-based primary care physicians.
Unlike care for patients with heart disease or diabetes, long-term care for cancer survivors is currently not integral in medical school education or primary care residency training. Our results strengthen the need for integrating cancer survivorship topics into residency education.29 Another training option could be postgraduate work in shadowing at cancer centers to bolster patient and oncologist receptivity in collaborating and transitioning into continuity care.7
After training, information about care of the cancer survivor is handled most quickly by direct discussions with the oncologist. Patient-specific guidelines with the integration of a “look-up” electronic education resource is useful in reducing knowledge gaps. A multi-team approach is more desirable for determining cancer-specific markers for early recurrence, timing of any routine diagnostic testing, and emotional support for survivors and their families.
A goal at many NCI Comprehensive Cancer Centers is to create partnerships with the community. An online format about cancer survivorship is through Project ECHO (Extension for Community Health care Outcomes). Monthly, telementoring ECHO programs are now available for primary care physicians, advanced practice providers, and community health workers or navigators.30 Evidence-based and case-based coursework usually includes an introduction to survivorship, palliative care, survivorship care plans, and current means in screening for any recurrence.
Limitations with this investigation deserve our acknowledgment. All information collected from the BRFSS was self-reported and subject to recall bias by the patient after several years. Reliability of the data collection has been validated, and surveyors were well-trained for consistency.31,32 Thirty-three of the 50 states requested use of the cancer survivorship module on their population from 2016 to 2020, so our findings may not represent the entire US population. However, those states were widely distributed throughout the US, and respondents represented adult populations within different regions of each state. The respondents' age, gender, health status, educational background, and health care insurance were well distributed, although our population consisted of a higher proportion of non-Hispanic whites than the US population. It was not possible to assess the status of the respondent's overall health, although most respondents stated that it was either good or excellent. Lastly, skin cancer was the most common reported by the survivors and likely includes those that are easily curable.
In conclusion, this report deals with the evolving health care needs of the expanding number of cancer survivors. Information about their management and instructions of care affect not only the patients but their physicians, especially family physicians in ambulatory practice settings. Enhancing primary care physician preparedness for the often-complex needs of these patients will require ease in accessing information about past and future rescreening and treatment options, preferably before transfer of care. Primary care, along with oncology and other subspecialties, should coproduce and translate new knowledge within a shared decision making framework to optimize care. These collaborative efforts will require an open dialog between the oncology team and those practitioners who provide more accessible and community-based care for these individuals with special needs.
Notes
This article was externally peer reviewed.
Funding: No funding was used to prepare this investigation.
Conflict of interest: None.
To see this article online, please go to: http://jabfm.org/content/35/4/708.full.
- Received for publication November 7, 2021.
- Revision received April 10, 2022.
- Accepted for publication April 25, 2022.




{kind=link}