
Abstract
Basal insulin therapy is a critical part of effective type 2 diabetes (T2D) management for many patients, yet its initiation and titration are often delayed or avoided. Aversion to basal insulin therapy contributes to unnecessary hyperglycemia and poorer outcomes for patients. Primary care physicians often make decisions regarding the initiation of basal insulin in T2D, as they work closely with patients and are well placed to discuss and manage the transition to basal insulin therapy. However, many primary care clinicians hesitate to initiate basal insulin due to concerns regarding time or effort needed to educate patients, doubts about patient acceptance or ability to manage titration or injection, or patient fears of hypoglycemia. Resistance to basal insulin therapy is often linked to the outdated perception that the need for insulin represents a failure to control the disease, or that insulin is dangerous or toxic. Time concerns can be addressed via group classes and mobile technology and by working with diabetes educators in the community. Hypoglycemia or weight gain can be minimized with proper titration and use of second-generation basal insulins. This article reviews strategies for the initiation of basal insulin therapy, with an emphasis on the characteristics and titration of second-generation basal insulins, introducing current guidelines and offering suggestions for recognizing and overcoming barriers to insulin therapy in the management of T2D.
- Hyperglycemia
- Hypoglycemia
- Insulin
- Primary Care Physicians
- Primary Health Care
- Type 2 Diabetes Mellitus
- Weight Gain
Type 2 diabetes (T2D), a leading cause of kidney disease, blindness, amputation, cardiovascular disease, and excess mortality, is a growing epidemic that affects more than 422 million people worldwide.1,2 In the USA, an estimated 90% to 95% of the 30.3 million people with diabetes have T2D.3 Achieving glycemic goals as early as possible is crucial if patients with T2D are to avert the long-term issues associated with uncontrolled hyperglycemia, including microvascular (and some macrovascular) complications and diabetes-related mortality.4⇓–6 Yet according to US Centers for Disease Control and Prevention National Health and Nutrition Examination Survey data for the years 2011 to 2014, only 51% of patients met the generally recommended goal of a glycohemoglobin A1C (A1C) <7.0%, and 27.7% had an A1C >8.0% (including 15.5% with A1C >9.0%).7 The management of T2 Days using individualized targets based on several patient factors (including disease duration and the presence of concomitant illness) is a well-established principle advocated by the American Diabetes Association (ADA).8 In 2014, however, less than two-thirds of patients with T2D in the USA achieved their individualized targets.7
Several new classes of medications, with multiple options within each class, have entered clinical practice in the past few years, complicating the treatment decision-making process for clinicians and patients and adding to the misperception that, as a treatment option, basal insulin is a “last resort.” Despite the increasingly complex management of patients with T2D, insulin remains a mainstay of therapy with a long history of effective and safe use in clinical settings. First-generation basal insulin analogs (insulin glargine 100 U/mL and insulin detemir 100 U/mL) have been in clinical use for over a decade, and clinicians are familiar with these treatments.9 Recently, second-generation longer-acting basal insulin analogs (insulin glargine 300 U/mL and insulin degludec 100 or 200 U/mL), which provide certain advantages over earlier analogs, have become available.10,11 The purpose of this article is to review processes, barriers, and practical issues in initiation and titration of basal insulin, particularly focusing on the second-generation basal insulins, insulin glargine 300 U/mL and insulin degludec.
Barriers to Insulin Initiation and Titration
Diabetes treatment is increasingly becoming the domain of primary care providers (PCPs), and initiation of insulin is commonly believed to be the most difficult aspect of diabetes treatment in primary care.12 It is estimated that more than 90% of patients with T2D receive diabetes care in primary care settings.13 Given their crucial role in managing patients with T2D, PCPs are often responsible for educating patients about the role of basal insulin therapy in their health and wellbeing and ensuring that patients are adherent with therapy.14 A further challenge is presented by patient nonadherence to therapy once basal insulin has been prescribed. Data suggest that almost 25% of patients prescribed basal insulin never use it or do not refill their prescription.15 Furthermore, almost 62% of patients who initiate basal insulin have interrupted therapy, and 18% discontinue therapy within a year of initiation.16 Despite its proven efficacy, multiple studies have found that as little as 30% of patients using basal insulin are achieving their glycemic goals. Failure to titrate is a key reason for this poor outcome, especially early in treatment.17⇓–19 To improve patient care and outcomes, examination of the issues raised when initiating basal insulin can help improve acceptance of therapy by PCPs and patients.
Physicians often cite concerns about patients' reluctance to start insulin, doubts about patient adherence, inadequate time for the effort needed to educate patients and help them find their proper insulin dose, and concerns about hypoglycemia and weight gain as reasons to delay initiation of basal insulin. Patients tend to emphasize concerns about hypoglycemia and weight gain, injection pain, social stigma, and disease progression.20 The phenomenon of psychological insulin resistance—in which resistance is based on fears or assumptions rather than clinical facts—can affect clinicians as well as patients.20 While patient and provider barriers are often viewed as distinct, in practice, provider attitudes have an impact on patient barriers. Clinicians who lack confidence in their patients' ability to manage basal insulin may be influenced by the knowledge that educating patients about their treatment and titration can be time consuming. Physicians who delay prescribing insulin may feed patient concerns that the need for insulin represents a serious decline in their health.21,22
Hypoglycemia
The occurrence of hypoglycemia with any diabetes therapy is a serious concern. Its effects range from undermining patients' confidence in their treatment and negatively affecting their quality of life to contributing to excess mortality and cognitive decline.23,24 The avoidance of hypoglycemia is an underlying principle of diabetes therapy, and a drug's potential to cause hypoglycemia should be considered when making treatment decisions.8
Patients who discontinue basal insulin are more likely to have been concerned about hypoglycemia, implying that hypoglycemia affects insulin adherence.25 Hypoglycemia risk can be minimized with appropriate titration and glycemic control during the first weeks (8 to 16) following insulin initiation, as well as by using basal insulins—particularly longer-acting basal insulins.26⇓⇓–29 In a randomized controlled trial, insulin-naïve patients with T2D and who initiated treatment with insulin glargine 300 U/mL (vs insulin glargine 100 U/mL) had less symptomatic hypoglycemia (46% vs 53% for insulin glargine 300 U/mL and 100 U/mL, respectively) and severe hypoglycemia (1% of participants) over 12 months of followup.10 Real-world data also show lower incidence of hypoglycemia with insulin glargine 300 U/mL versus insulin glargine 100 U/mL in insulin-naïve patients with T2D.30 Insulin-naïve patients who initiated insulin degludec 100 U/mL (vs insulin glargine 100 U/mL) had significantly less nocturnal confirmed hypoglycemia (0.25 vs 0.39 episodes per patient-year of exposure for insulin degludec 100 U/mL and insulin glargine 100 U/mL, respectively) and numerically less overall confirmed hypoglycemia (1.52 vs 1.85 episodes per patient-year of exposure for insulin degludec 100 U/mL and insulin glargine 100 U/mL, respectively).11 Direct discussion with patients regarding the potential risk of hypoglycemia, the rarity of severe hypoglycemia, and hypoglycemia prevention and recognition practices may help mitigate patient fears when initiating and titrating basal insulin.31,32
Weight Gain
Weight gain is a common occurrence with basal insulin, not only because of the anabolic effects of insulin itself, but also due to patient actions such as defensive eating to offset hypoglycemia.33 As with hypoglycemia, both PCPs and their patients express concerns over weight gain. This presents a barrier to insulin initiation and titration, and undermines treatment efficacy.25,34⇓⇓–37
In patients who need to minimize weight gain or lose weight, addition of basal insulin is advised only after addition of other agents such as GLP-1 RAs, SGLT-2 inhibitors, or DPP-4 inhibitors.38 Insulin-related weight gain can be mitigated by using treatment strategies that combine basal insulin with metformin or treatments associated with weight loss, such as fixed-ratio combinations with a GLP-1 RA or with an SGLT-2 inhibitor.33,38,39 Insulin analogs result in less weight gain than neutral protamine hagedorn (NPH) insulin.40,41 In clinical trials, weight gain associated with second-generation basal insulin analogs was generally low, ranging from a mean of 0.5 kg to 2.5 kg,10,26,27,42 with younger age being one of the baseline predictors of higher weight gain.43,44 Insulin glargine 300 U/mL (but not insulin degludec) was associated with less weight gain than insulin glargine 100 U/mL.10,26,27,42
Lack of Time and Increased Treatment Complexity
Concerns regarding time constraints and the complexity of initiating or titrating basal insulin are issues commonly cited by both PCPs and patients.25,32,34,35,45,46 More than half (53%) of PCPs surveyed in the USA felt that the training and education of patients regarding titration was “very challenging” or “extremely challenging” to achieve in the limited time available during consultations.25 In a patient survey, 50.6% believed that insulin therapy would restrict their lives and 40% to 50% believed that the regimen would be too complex for them to handle.46 In general, patients who find integrating insulin into their daily routine difficult are more likely to discontinue therapy.25 The use of preprepared media resources that the patient can rewatch at home, such as an injection-pen or titration training video, can take less than 5 minutes, and may allay fears regarding the complexity of treatment.
Self Blame and Feelings of Failure
Self blame and feelings of failure associated with the need to initiate insulin are frequently cited by patients and may be underestimated by PCPs.15,36,37 In the Diabetes Attitudes, Wishes, and Needs (DAWN) study, physicians and diabetes nurses failed to recognize that patients' feelings of self blame were associated with delay of insulin initiation, which, combined with a common physician belief that insulin therapy should be delayed as long as possible, suggests a possible causal link between physician and patient attitudes.47 Patients may be receiving messages from physicians that initiation of insulin represents a failure to control diabetes or a “punishment” for failing on their oral therapies.8,46,47
Some patients who are using basal insulin, but are not at their glycemic goal, carry the perception that titration of insulin dose is a sign of worsening disease.25 Physicians should assure patients that an increasing dose does not represent a failure. This may be done by discussing with patients the need to start basal insulin on a low dose and slowly build to a “regular” dose, which will help them avoid hypoglycemia. Further, physicians should emphasize that dose titration does not indicate that their disease is worsening, but rather that it is the normal process when initiating basal insulin.
As many patients view insulin therapy as a “last-resort” therapy, physicians should instead introduce the concept of insulin at the time of diagnosis. They should remind patients that basal insulin is indicated as one of several options for treatment intensification if A1C remains elevated after treatment with oral antidiabetes drugs (OADs) or injectable GLP-1 RAs.38 Patients should be educated that diabetes is a progressive disease; therefore, even if they are doing everything correctly with lifestyle modification and medication, diabetes will still progress over the years, and injectable therapy may eventually be needed. Approximately 30% of people with T2D use insulin during the course of their disease, which likely underestimates the true need.
Misperceptions
Patients' misperceptions, based on poor or inaccurate knowledge about insulin therapy and diabetes, inform their fears and undermine their acceptance of treatment. Patients may wrongly believe that insulin is not effective.15,34⇓⇓–37,47 Patients may also hold a belief that insulin is addictive or toxic, or that it leads to myocardial infarction.15,46⇓–48 The outdated concern about heart disease persists and reflects a lack of knowledge about the role of diabetes in increasing risk for an array of serious cardiovascular outcomes. To address this fear, clinicians should be knowledgeable about the Outcome Reduction with an Initial Glargine Intervention (ORIGIN) study, which showed that insulin glargine 100 U/mL has a neutral effect on cardiovascular outcomes overall and a beneficial effect on microvascular complications, and the DEVOTE study, which established insulin degludec 100 U/mL as having a similar effect to insulin glargine 100 U/mL on the risk of cardiovascular events.49⇓–51 Basal insulins are recommended in the recent ADA/European Association for the Study of Diabetes (EASD) consensus statement as a treatment intensification option for patients with established atherosclerotic cardiovascular disease or chronic kidney disease requiring additional glucose-lowering efficacy after introduction of an SGLT2 inhibitor or GLP-1 RA.38 Unfortunately, physicians may often underestimate patients' concerns that their disease will worsen following insulin initiation.36,52 Another misperception that patients may have, in particular those who drive for a living, is that they will no longer be able to drive when on insulin therapy due to hypoglycemia risk. Clinicians can assure these patients that they can apply for an exemption to a rule that prevents interstate commercial driving while using insulin.53
Lack of Confidence in Patient Ability
PCPs are often familiar with their individual patient cases and may have insight into patient behavior that can affect the physician's opinion regarding the suitability of basal insulin therapy; many physicians underestimate the ability of their patients to manage their disease—most commonly due to concerns surrounding daily injection and titration.48,54 While issues regarding titration of insulin and patient adherence are real, the majority of people can manage their condition using basal insulin when given appropriate diabetes-specific education and support, such as the recommended diabetes self-management education and support (DSMES) programs.16⇓⇓–19,32,38,55 Self titration is recommended by guidelines, achieves similar control to physician-guided titration, and helps overcome a number of insulin barriers.8,56⇓–58 Nonetheless, many health care providers add to their burden in caring for patients using insulin; physicians say they prefer to manage titration alongside their patients, citing likely errors and lack of adherence by patients as potential issues.25,57 It is hard to judge how competent patients are in self titration. The majority of US patients with experience using basal insulin (83%) expressed some confidence in being able to adjust their basal insulin dose correctly; yet in that same study, 42% of patients reported being unaware that titration was required.25 This is where physicians' insights into their patients' behavior can play an important role by encouraging independence in those who can manage it, and by supporting those patients who have doubts about their own abilities. Further, it underscores the important role that educating patients has in optimizing outcomes with insulin therapy. Extending education in basal insulin self-titration methods may improve patient confidence and treatment adherence.25
Novel mobile technology can play a significant role in helping patients titrate and manage their insulin dose, and thus improve both physician and patient confidence. For example, using a web tool to help with insulin titration was shown to provide similar A1C reductions, with similar proportions of patients achieving A1C ≤7.0% and similar hypoglycemia incidence, while increasing patient satisfaction and reducing the number of additional health care provider visits compared with enhanced usual therapy.59 Although this study failed to demonstrate noninferiority for the web tool compared with enhanced usual therapy for the primary composite outcome, the authors concluded that such tools have the potential to reduce physician and patient barriers related to complexity of titration, reduce the time taken to titrate basal insulin, and reduce resource utilization related to basal insulin initiation and titration.59 Using a web tool or a diabetes app through a smartphone to track blood glucose and diet may improve diabetes management and self monitoring.60 The US Food and Drug Administration (FDA) requires premarket approval for insulin dose-calculating apps.61 Currently approved apps are My Dose Coach (https://www.mydosecoach.com), Voluntis' Insulia (http://www.insulia.com), and Accu-Chek (https://www.accu-chek.com).62,63 These apps offer dose calculation based on fasting plasma glucose (FPG) and hypoglycemia data, as well as a database of diabetes information.62,63
Well-designed patient support programs may help improve treatment adherence; for example, the COACH support program provides patients initiating insulin glargine 300 U/mL with tailored support via live phone contact with a clinically trained nurse and resources including product-focused educational materials and encouragement to initiate lifestyle changes.64 Patients enrolled in this program were found to be more likely to refill their prescriptions and stay on therapy compared with matched controls.64
Social Concerns
PCPs are likely to consider a wider array of patient-related factors than specialists when it comes to initiating basal insulin. However, patients' social concerns regarding basal insulin therapy are frequently overlooked.36,52 Social concerns are often related to perceived social stigma, which can result in, for example, a reluctance to inject insulin in public or around family members.37,65 The fear that using basal insulin will interfere with the patient's daily routine is likely to have a negative effect on several aspects of their social life.15,25,37,46 In the Japanese population of the DAWN trial, avoiding social stigma was cited as an issue by 55% of patients and only 7% of physicians.52
To address personal concerns in a social setting, group visits or group classes can be helpful to introduce patients who are new to basal insulin to patients who are already using it. This provides an opportunity to talk with peers about how insulin affects them, whether daily injection is an undue burden, and how they have fit using insulin into their daily lives.
Injection Pain
PCPs should be aware that very few patients have genuine needle phobia, and that for these few patients, counseling can be effective in allaying their fear.66 Pain or fear related to injections or self monitoring of blood glucose (SMBG) is perhaps the most acknowledged barrier to basal insulin initiation. In a survey of beliefs regarding insulin, 93% of PCPs believed that patients would be more likely to initiate insulin if it could be administered without injection, and 89% believed the injection route was the greatest barrier to acceptance.12 However, studies suggest that fear of injection pain is one of the factors most overestimated by PCPs when assessing their patients' receptiveness to therapy.36,48,52 In clinical use, only 37% of patients using injection pens report injection-related pain.67 However, fear of injection, like other barriers, may be anticipatory; it is often transient and tends to minimize or disappear once patients have started using basal insulin.68 Specific fears can be identified using standardized survey tools such as the Diabetes Fear of Injection and Self-testing Questionnaire (D-FISQ).69
Breathing techniques, such as deep breathing and a forceful exhale during injection, may be helpful for some patients.67,70 Anxiety around injection can be mitigated by use of modern insulin injection pens with shorter, finer-gauge needles, which have been shown to reduce pain and bleeding compared with earlier delivery devices.67 It is helpful to demonstrate injection technique in the office before sending patients home with their first prescription; this can mitigate fears about technique and also show patients that injection pain is minimal.67 Physicians may also consider teaching insulin injection at the time of diagnosis, when patients are taught finger-stick glucose monitoring; patients will notice that insulin injection is the less painful of the two.
Basal Insulin Initiation and Titration: Guideline Summary
Basal insulin remains the single most effective medication to reduce hyperglycemia and is a recommended option that can be combined with almost all other T2D therapies at any time in the course of disease management.8,39 Patients for whom basal insulin should be considered include those with complicated noninsulin regimens that may contribute to poor adherence and failure to achieve A1C goals, and patients with T2D who have not attained A1C goals despite multiple treatments over time. The 2018 ADA/EASD consensus report recommends GLP-1 RAs as the preferred initial choice for patients requiring an injectable medication, due to their lower risk of hypoglycemia and association with weight loss; however, basal insulin is recommended as the first injectable therapy for patients with extreme or symptomatic hyperglycemia, or for whom GLP-1 RAs are not suitable.38 While a number of factors (eg, comorbidities such as cardiovascular disease; need for weight loss; and cost considerations) influence the choice and intensification pathways of glucose-lowering medications, basal insulin is an option for all patients who still have A1C levels above target despite optimization of other treatments.38 The 2018 ADA/EASD consensus report provides advice on the types of basal insulin preferable in different situations, with insulin glargine 300 U/mL or insulin degludec to be considered over insulin glargine 100 U/mL, insulin detemir, and NPH due to their lower risk of hypoglycemia, with considerations for lower-cost insulins in patients where cost is a major factor.38
Basal insulin therapy is designed to replace endogenous basal insulin in patients who lack insulin either completely, as in type 1 diabetes, or partially, as is the case in T2D. The ADA/EASD and the American Association of Clinical Endocrinologists/American College of Endocrinology state that the goals of insulin therapy are to replicate, as closely as possible, a normal glycemic profile without unacceptable weight gain or hypoglycemia.8,39,71 These guidelines, and those from the International Diabetes Federation, recommend initiation of insulin with basal insulin followed by titration to a FPG target (Table 1).8,39,56 Each organization further states a preference for basal insulins over NPH insulin because of their relatively flat action profile over 24 hours, which reduces glycemic variability, and lower hypoglycemia risk.8,39 In practice, however, basal insulin is usually considered as a later therapy option for patients with T2D inadequately controlled on other therapies (Figure 1).8,38,39 At initiation of basal insulin, clinicians should review and adjust a patient's current diabetes medications. Discontinuation of OADs that may increase the risk of hypoglycemia, such as sulfonylureas and other insulin secretagogues, is typically mandated; however, other types of OADs can be continued as they can help to lower insulin dose requirements.8,39

Antihyperglycemia Therapy in Type 2 Diabetes: Consensus of the American Diabetes Association and European Association for the Study of Diabetes.38 ASCVD, atherosclerotic cardiovascular disease; CKD, chronic kidney disease; CVD, cardiovascular disease; CVOT, cardiovascular outcomes trials; DPP-4, dipeptidyl peptidase-4; eGFR, estimated glomerular filtration rate; GLP-1 RA, glucagon-like peptide-1; HbA1C, glycohemoglobin; HF, heart failure; SGLT2i, SGLT2 inhibitor; SU, sulfonylurea; TZD, thiazolidinedione.
Available Basal Insulin Options
The number of different types of basal insulin available may contribute to challenges and delays in initiating treatment for appropriate patients. The first-generation basal insulins (ie, insulin glargine 100 U/mL and insulin detemir 100 U/mL) have a duration of action of up to 24 hours and are injected once daily in most patients.
There has been an increase in “follow-on biologics” for first-generation insulin analogs, with several currently under development or approved for use as basal insulins. For example, the FDA-approved alternative version of insulin glargine 100 U/mL (LY2963016; Basaglar, Eli Lilly and Company, Indianapolis, IN) has been shown as noninferior to the originator product (insulin glargine 100 U/mL), with similar safety and immunogenicity profiles.72,73 While discussion of follow-on insulins is out of the scope of the current manuscript, physicians should be aware of whether interchangeability is permissible for alternative versions of insulin analogs, as well as the potential cost-saving benefits from use of follow-on insulins.74
The longer-acting second-generation basal insulins (ie, insulin glargine 300 U/mL and insulin degludec 100 or 200 U/mL) have an extended duration of action that exceeds 24 hours. Insulin glargine 300 U/mL provides the same insulin dose in one-third the volume as insulin glargine 100 U/mL and, following injection, releases the dose more gradually from the subcutaneous tissue. Insulin glargine 300 U/mL has a duration of action of up to 36 hours, giving a more evenly distributed pharmacokinetic/pharmacodynamic (PK/PD) profile with increased stability and reduced variability compared with insulin glargine 100 U/mL and insulin degludec 100 U/mL.75⇓⇓–78 Insulin degludec is available in 100 U/mL and 200 U/mL formulations, the 200 U/mL product providing the same dose as the 100 U/mL formulation in half the volume. Insulin glargine 300 U/mL and insulin degludec 100 and 200 U/mL have been compared with insulin glargine 100 U/mL in clinical trials, with results showing that similar A1C reductions are achieved with less hypoglycemia (particularly nocturnal hypoglycemia), and less weight gain.10,11,26,42,78,79 These outcomes have also been reflected in real-world studies, where both insulin glargine 300 U/mL and insulin degludec were associated with reduced hypoglycemia risk but similar glycemic control levels to other basal insulins.78,80⇓⇓⇓–84 Insulin glargine 300 U/mL and insulin degludec 100 and 200 U/mL are appropriate for use in any patient who requires insulin. In addition, the use of patient support programs, such as COACH and Cornerstones4Care, in combination with these longer-acting basal insulins has demonstrated increased compliance and adherence to treatment schedules. Patients in the COACH program were significantly more likely to refill their prescriptions and stay on therapy (P < .0001 at 6 and 9 months after initiating insulin glargine 300 U/mL for both measures), when compared with patients who did not take part in the program.64
Incorporating Longer-Acting Basal Insulins in Clinical Care
Although the duration of action is up to 36 hours with insulin glargine 300 U/mL, and up to 42 hours with insulin degludec 100 or 200 U/mL, each is designed to be given once daily. The extended duration of action allows patients some flexibility in dosing rather than having to stick to a rigid 24-hour schedule. For example, if a morning dose is missed, patients can take their insulin that evening without compromising basal coverage (provided the 2 doses are separated by at least 8 hours).85,86
For patients not previously taking insulin, the recommended starting dose of insulin glargine 300 U/mL is 0.2 U/kg once daily, according to the manufacturer's guidelines.87 For insulin degludec, the recommendation is 10 U once daily.88 The pens in which these longer-acting basal insulins are provided are specially designed so that the dose counter shows the desired dose in units, meaning no dose recalculation is required, which simplifies administration.87,88
If patients are converting to a longer-acting basal insulin from another basal insulin product (Table 2), they should initiate insulin degludec at the same number of units being used. Insulin glargine 300 U/mL is initiated at the current number of units, but patients must be told to expect their insulin dose to increase by up to 20% compared with insulin glargine 100 U/mL. This is an important point to emphasize with patients so that they do not underdose insulin glargine 300 U/mL or fear that their therapy is unsuccessful as they need a higher dose. Patients should be reminded of the reduced weight gain and hypoglycemia with insulin glargine 300 U/mL to mitigate potential concerns related to the expected dose increase.27
Because the duration of action of the longer-acting basal insulins exceeds 24 hours, while dosing is once a day, there were initial concerns that repeated use of the longer-acting analogs could lead to overaccumulation of insulin in the circulation with a resultant increase in hypoglycemia risk. With prandial insulin, the phenomenon of “stacking” can be observed when additional doses are given before the previous dose has been completely absorbed, resulting in overlapping insulin effects and an increased risk of hypoglycemia.89 Nevertheless, this phenomenon does not occur in clinical use of longer-acting basal insulins because of their relatively flat PK/PD profiles and the achievement of steady state, where the rate of insulin absorption matches the rate of elimination over the dosing period.89 Using the recommended, less-frequent titration schedule of longer-acting basal insulins allows the insulin to reach steady state and avoids this concern.
Titration of Basal Insulin
Targeted titration of basal insulin is an essential part of the process of initiating basal insulin therapy.8,38,39,71 Regular glucose monitoring is necessary for accurate titration, and patients must be trained in SMBG using commercially available glucose meters and test strips. For most patients initiating basal insulin, SMBG can be done once a day to assess FPG with the dose adjusted upward or downward at regular intervals based on the results. Adjusting every 2 to 3 days is typically recommended with insulin glargine 100 U/mL and insulin detemir; however, in practice it is also appropriate to tell patients to simply increase by 1 U every day until FPG reaches target.90 There are several other common approaches to titration illustrated in Table 1 and Figure 2. In addition, a recently published review discusses practical considerations for insulin initiation and titration in patients with T2D.91 These can be adapted based on the patient's capabilities, hypoglycemia risk, comorbidities, and other factors. Because of the PK/PD properties of insulin glargine 300 U/mL and insulin degludec 100 or 200 U/mL, they are not titrated as frequently as insulin glargine 100 U/mL. Generally, titration should be done no more often than every 3 to 4 days, to allow insulin concentrations to reach steady state (Table 2).87,89 Although it would be off label for insulin glargine 300 U/mL, a patient-driven algorithm changing the dose by 1 U/day has been shown to provide comparable efficacy and safety to an algorithm that changes the dose every 3 days. Furthermore, the 1 U/day algorithm was preferred by health care professionals.90

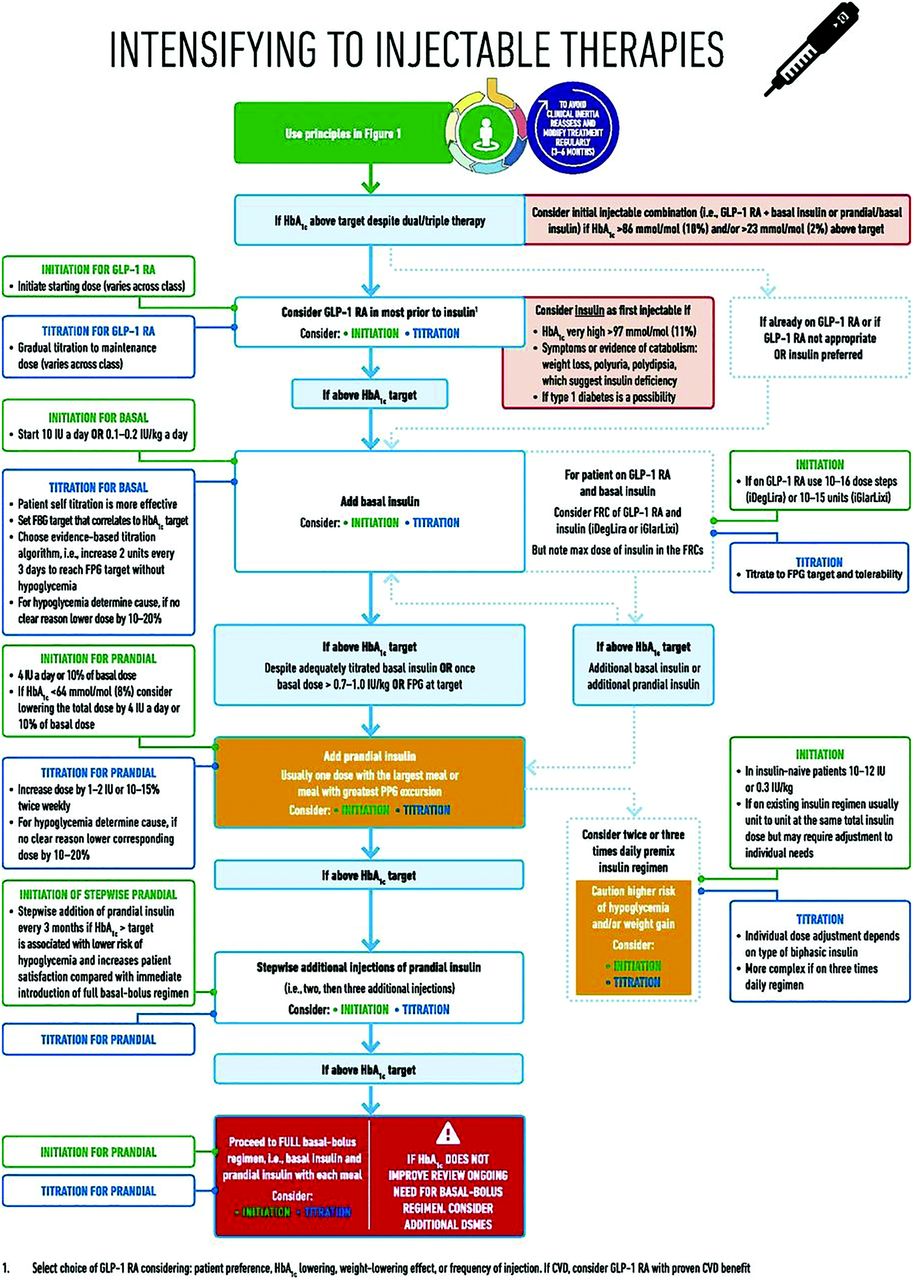
Intensification to Injectable Therapies (GLP-1 RAs and Basal Insulin): Consensus of the American Diabetes Association and European Association for the Study of Diabetes.38 FBP, fasting blood glucose; FPG, fasting plasma glucose; FRC, fixed-ratio combination; GLP-1 RA, glucagon-like peptide-1 receptor agonist; HbA1C, glycohemoglobin; IU, insulin units; PPG, postprandial glucose.
Barriers to Initiation and Titration Are Also Applicable to Nonbasal Insulins
While the initiation and titration of basal insulins are the focus of the current discussion, many of the barriers outlined above are also potentially applicable to prandial insulin. Patients beginning prandial insulin are usually already receiving basal insulin, and therefore physicians may consider some of the barriers to be less of a concern for these insulin-experienced patients. However, escalation of therapy may be associated with feelings of failure, and patients may still have concerns about potential weight gain or hypoglycemia from the new treatment, or the increasing complexity of the treatment regimen. Transition to multiple injections per day may also lead to an increased fear of disruption of a patient's daily routine, or reduced treatment adherence. The paths to overcoming these barriers discussed below are important considerations for patients transitioning to all insulins, not just those receiving basal insulins.
Communication and Education: The Path to Overcoming Barriers
Education of physicians and their patients is the first essential step to demystify basal insulin usage and remind us of its importance as a cornerstone in diabetes care. Beginning at diagnosis, patients should receive education about their disease, its likely progression, the consequences of poorly controlled hyperglycemia, and the role of basal insulin in treatment and improving their long-term outcomes.8 DSMES programs, which are recommended from diagnosis and throughout treatment, generally allow face-to-face contact with trained educators in individual or group settings, and can promote adherence to treatment as well as aid in lifestyle management interventions such as healthy eating and increased physical activity.38 The initiation of basal insulin should never be used as a threat to attempt to maintain a patient's adherence to an exercise or OAD regimen.8,36 To facilitate patient education, group-based DSMES programs, the use of mobile technology, and the use of diabetes educators and specialists in difficult cases can reduce the time burden of individual patient education.92
Individualized patient care extends to understanding a patient's specific barriers to basal insulin therapy and is the first step in overcoming them.31 Data suggest that patient barriers to insulin may be temporary and overcome once they experience insulin therapy and confront their fears.68 This is best achieved through open communication with the individual; for example, via direct email communication offering titration advice and ensuring that the patient does not feel isolated. Effective strategies that can be used to identify and address specific barriers have been developed; once individual barriers have been identified, counseling strategies are available to address them (Table 3).
Conclusions
Basal insulin represents an effective therapy that can be initiated at any time during treatment of T2D in a patient who has not reached individual glycemic goals. PCPs should be careful not to allow their own attitudes and concerns to become barriers when initiating a patient on insulin therapy and should use their familiarity with the patient to fully understand and address any issues, fears, and concerns that may impact optimal therapy. Improvements in basal insulin formulations, pen injection devices, and digital dose titration applications can be used alongside practical measures focused on communication and patient education to overcome barriers to basal insulin initiation and titration.
Acknowledgments
This article was funded by Sanofi US, Inc. The authors received writing/editorial support in the preparation of this manuscript provided by Grace Richmond, PhD, and Rasila Vaghjiani, PhD, of Excerpta Medica, funded by Sanofi US, Inc.
Notes
This article was externally peer reviewed.
Funding: This article was funded by Sanofi US, Inc. The authors received writing/editorial support in the preparation of this manuscript provided by Grace Richmond, PhD, and Rasila Vaghjiani, PhD, of Excerpta Medica, funded by Sanofi US, Inc.
Conflict of interest: LP is on the speakers bureau for Novo Nordisk, Merck, BI/Lilly, Astra Zeneca, Janssen, Orexigen, and advisory board/consultant for Novo Nordisk, Merck/Pfizer, BI/Lilly, Sanofi, Medscape, WebMD. TS-C is a consultant/speaker for Dexcom, Novo Nordisk, Sanofi, Senseonics, and Valeritas. LV and JN have nothing to declare.
To see this article online, please go to: http://jabfm.org/content/32/3/431.full.
- Received for publication May 31, 2018.
- Revision received January 25, 2019.
- Accepted for publication February 5, 2019.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Post Hoc Analysis Evaluating the Impact of Antihyperglycemic Background Therapies on Attainment of A1C Targets Without Hypoglycemia in the ACHIEVE Control Pragmatic, Real-Life Study
- Evaluation of Clinical Outcomes With the V-Go Wearable Insulin Delivery Device in Patients With Type 2 Diabetes
- The Most Frequently Read Articles of 2019
- Family Medicine: Data Driven Practice with Emphasis on Underserved Patients