
Abstract
Background: While increasing evidence supports the beneficial effects of shared decision making (SDM) on patient outcomes, the mechanisms underlying this relationship is unclear. This study evaluated length of the patient-provider relationship as one potential factor that may explain how SDM affects medication adherence in patients with hypertension.
Methods: An observational study of 75 hypertensive patients and 27 providers in 3 primary care practices in New York City. A single-item measure assessed patients' preferences for decision-making style at baseline; medication adherence was collected over the 3-month study with an electronic monitoring device. Length of the relationship was measured as the number of years with the provider, and dichotomized as less than or greater than 1 year with the provider. Two generalized linear mixed models were conducted to determine whether the SDM-adherence association was modified by length of the relationship.
Results: Most patients were Black and women, and 64% were seeing the same provider >1 year. Providers were mostly White women and have been at the clinic for 6 years. In the main-effects model, patients were more likely to exhibit better adherence when they preferred shared and active decision-making styles as compared with those who preferred a passive style (B = 15.87 [Standard Error [SE]: 6.62], P = .02; and B = 22.58 [SE:7.62], P = .004, respectively). In Model 2, the relative importance of SDM on adherence decreased as years with the provider increased (t(48) = 2.13; P = .04).
Conclusion: The benefits of SDM over passive decision making on medication adherence were reduced with increasing years of the patient-provider relationship. Having an established relationship with the provider may have a positive impact on medication adherence that is comparable to relationships high in SDM.
Shared decision making (SDM) has been regarded as the “pinnacle of patient-centered care.”1 As a dyadic process, it recognizes and incorporates both the provider's medical expertise and the patient's lived experience into discussions about care options.2⇓–4 Specifically, within the SDM framework, patients and providers share information about available options, express their preferences and goals for the possible outcomes of the decision, and collaborate in making the final decision.2⇓–4 A recent systematic review reported that an increasing percentage of patients prefer having a shared role in decision making with their provider (from 71% after 2000 vs 51% prior to 2000).5 Patients who report high levels of SDM within the clinical encounter are more likely to exhibit positive health outcomes, including improved self-reported health status, self-management behaviors, emotional health, recovery from discomfort, reduction in referrals for diagnostic testing, satisfaction with care, adherence to treatment plans, choosing less invasive and costly treatment options; and shorter hospital stays.6⇓⇓–9 Given these benefits, the Institute of Medicine and the US Preventive Services Task Force advocates for providers to use SDM when discussing treatment options with patients.10,11
While a growing body of research supports the positive attributes of engaging in SDM on both patient- and relationship-level outcomes, the mechanisms through which SDM may exert its effects remains unclear. A thematic analysis of the extant literature suggests that attributes of the patient-provider relationship and the health care system within which the relationship occurs can either enable or impede patients' ability to engage in SDM.12,13 Good continuity of care is one aspect of the health care system that can engender positive patient-provider relationships (eg, by increasing affiliation) and in turn, facilitate patient's participation in SDM.14 Continuous care is particularly important for patients with chronic diseases such as hypertension who require ongoing management with an established provider to have consistent communication about the disease and its treatment, support patient adherence to their medications, and ensure coordination of care across providers.15⇓–17 In this article, we examine longitudinal continuity (ie, number of years with the provider) as one potential component of continuous care that may explain how SDM affects health outcomes such as medication adherence in hypertensive patients.
Our study aims were 2-fold: 1) to evaluate the direct effect of SDM on objectively measured medication adherence among a sample of primary care providers (PCPs) and their hypertensive patients, and 2) to examine whether number of years with the provider modified the SDM-adherence association. We hypothesized that preference for SDM would be associated with better medication adherence as compared with preferences for passive and active decision making, and that this association would be stronger as years with the provider increased.
Methods
Participants
Participants were previously recruited in an observational study, which evaluated the patient, provider, and clinic-level factors that impact medication adherence among hypertensive patients from 3 primary care practices, which serve a multi-ethnic, low-income population in New York City, NY.18 Patient eligibility included 1) self-identification as Black/African American or White/white, 2) diagnosis of hypertension (ICD: 401 to 401.9), 3) taking at least 1 antihypertensive medication, 4) aged ≥18 years, and 5) having attended at least 1 prior visit with the participating PCP. PCPs were defined as attending providers (MD/DO) or nurse practitioners who provided care at the practices to the study patients. All participants provided informed consent approved by New York University's Institutional Review Board.
Data Collection
Data were collected at baseline and 3 months following the baseline patient-provider visit. Trained research assistants collected data on patients' preferences for decision making before the baseline clinic visit. After the visit, research assistants provided each patient with an electronic monitoring device (EMD) to measure his/her medication-taking behavior for the duration of the 3-month study. EMDs are standard pill bottles with an electronic cap that records the date and time the bottle is opened. If patients were prescribed multiple antihypertensive medications, PCPs were asked to choose 1 medication taken once daily to be placed in the bottle. Patients received a telephone call the day after the baseline visit to ensure they placed the correct medication in the bottle.
Study Measures
Independent Variable
Decision-making preference was assessed with the Control Preferences Scale19 at baseline. The scale categorizes decision making preference into 3 styles: active, shared, and passive by asking patients to indicate what role they would like to play during clinical visits with the provider. Patient preference for decision making was categorized as active (patient-driven) if they chose the responses, “I prefer to make the final treatment selection,” OR “I prefer to make the final treatment selection after seriously considering my doctor's opinion.” A preference for SDM was categorized by the response, “I prefer that my doctor and I share responsibility for which treatment is best for me.” Lastly, patient preference for decision making was categorized as passive (provider-driven) if they chose the responses, “I prefer that my doctor make the final decision about which treatment will be used, but seriously consider my opinion,” OR “I prefer to leave all decisions regarding my treatment to my doctor.”
Dependent Variable
Medication adherence was assessed with an EMD as noted above. To control for “pocket dosing” (eg, use of pill boxes, removing doses for travel), patients were also asked to keep diaries during the 3-month study period, which were accounted for in the analyses.20 Medication adherence was calculated using the scheduling adherence metric, using the formula, ([the number of pills taken/the prescribed dose per day] × 100%)/the time interval of study period (90 days).21 Adherence rates ranged from 0% to 100%.
Moderator Variable
Length of the patient-provider relationship was collected at the baseline visit using the longitudinal continuity item on the Primary Care Assessment Survey.22 Responses included the following time intervals: less than 6 months, between 6 months and 1 year, 1 to 2 years, 3 to 5 years, and more than 5 years. Responses were dichotomized into 2 categories based on the median value of the scale (median, 4.5; range, 1 to 7): less than 1 year with the provider and 1 year and greater.
Covariates
Sociodemographic Data. Patient-level data included age, gender, race, marital status, employment status, education and income level, and insurance status. Provider-level data included age, gender, race, place of birth, duration of practice at the site, type of provider (ie, MD/DO, nurse practitioner) and specialty. Data on medical comorbidity,23 prescribed antihypertensive medications, and blood pressure were extracted from patients' electronic medical records at the baseline and 3-month study visits.
Analysis
Descriptive statistics were generated for the patient, PCP, and visit characteristics in addition to frequencies of decision making preferences. We compared adherence rates by decision-making preference using the χ2 statistic. Patient- and provider-level variables were included in the multivariate models if they were associated with decision making preference or medication adherence at P < .10 in bivariate analyses.
Analyses were conducted using generalized linear mixed models. Providers were modeled as the random effect to adjust for potential nesting caused by multiple patients seeing the same provider. All independent variables were modeled as fixed effects. Two generalized linear mixed models were conducted to determine whether the association between decision-making preference and medication adherence was modified by length of the patient-provider relationship. In Model 1, independent associations between the independent variable (decision-making preference) and dependent variable (adherence) were assessed, while adjusting for selected patient- and PCP-level covariates (eg, patient's age and race; provider's gender). In Model 2, the product between length of the relationship and decision making preference was added to Model 1. Specifically, point estimates for medication adherence were estimated using the fully adjusted linear regression of Model 2. These estimates were calculated by dividing the sample by decision making style and by individuals who were with their provider for <1 year and those who were with their provider for ≥1 year. These estimates were then plotted and 95% CI were generated. SPSS version 23 (IBM Corp., Armonk NY) was used for all analyses and significance levels were set at P ≤ .05.
Results
Patient and PCP Characteristics
A total of 104 patients were recruited into this study: 75 (83%) had usable EMD data. There were no significant differences between patients with and without usable EMD data for all demographic and decision-making variables. Of the 28 PCPs invited to participate, only 1 declined. Therefore, our study analytic sample was comprised of 75 patients and 27 PCPs. Patient and PCP characteristics are shown in Tables 1 and 2, respectively. Approximately half of patients were female (56.0%), one third had Medicaid (33.3%), and half reported some college education (56.0%), with a mean age of 60 (SD, 10.3) years. Almost two thirds of patients (62.7%) had been seeing the same PCP for at least 1 year. Most PCPs were MDs (96.3%), internists (94.3%), and female (66.7%) with a mean age of 36.2 years.
Comparison of Patient Characteristics by Decision-Making Preference (N = 75), 2011 to 2014
Demographic Characteristics of Primary Care Providers from Safety-Net Practices (N = 27), 2011 to 2015
Decision-Making Preferences for the Total Sample
Almost two thirds of patients (57.3%) preferred to engage in SDM in the clinic visit (Table 3). Alternatively, one quarter (24.0%) of patients preferred active decision making, in which patients make the final decisions, after possibly considering the provider's opinion. Few patients preferred passive decision making (18.7%) suggesting that fewer individuals want to leave decision making solely up to their provider.
Rates of Medication Adherence by Decision-Making Preference, as Assessed by an Electronic Monitoring Device Using the Scheduling Adherence Metric over the 3-Month Study Period (N = 75)
Relationship Between Decision-Making Preference and Medication Adherence
The mean adherence rate for the total sample was 81.3% (SD, 23.1). Patients who preferred an active decision-making style (N = 18) had a mean adherence of 89.3% (SD, 17.7; Table 3). The mean adherence for patients who preferred SDM (N = 43) was 83.8% (SD, 19.5). Patients who preferred a passive style (N = 14) exhibited the lowest adherent rate of 63.0% (SD, = 30.2).
After adjusting for patient (age, race, insurance status, number of medications) and provider characteristics (gender, age), there was a significant main effect of decision-making style on adherence in Model 1, such that preferences for shared and active decision-making styles were associated with better medication adherence as compared with preference for a passive style (B = 15.87 [Standard Error [SE]:6.62], P = .02; and B = 22.58 [7.62], P = .004, respectively; Table 4).
Results of the Generalized Linear Mixed Models Testing the Associations Between Medication Adherence and Decision-Making Preference as Moderated by Years with Primary Care Provider Among 75 Hypertensive Patients
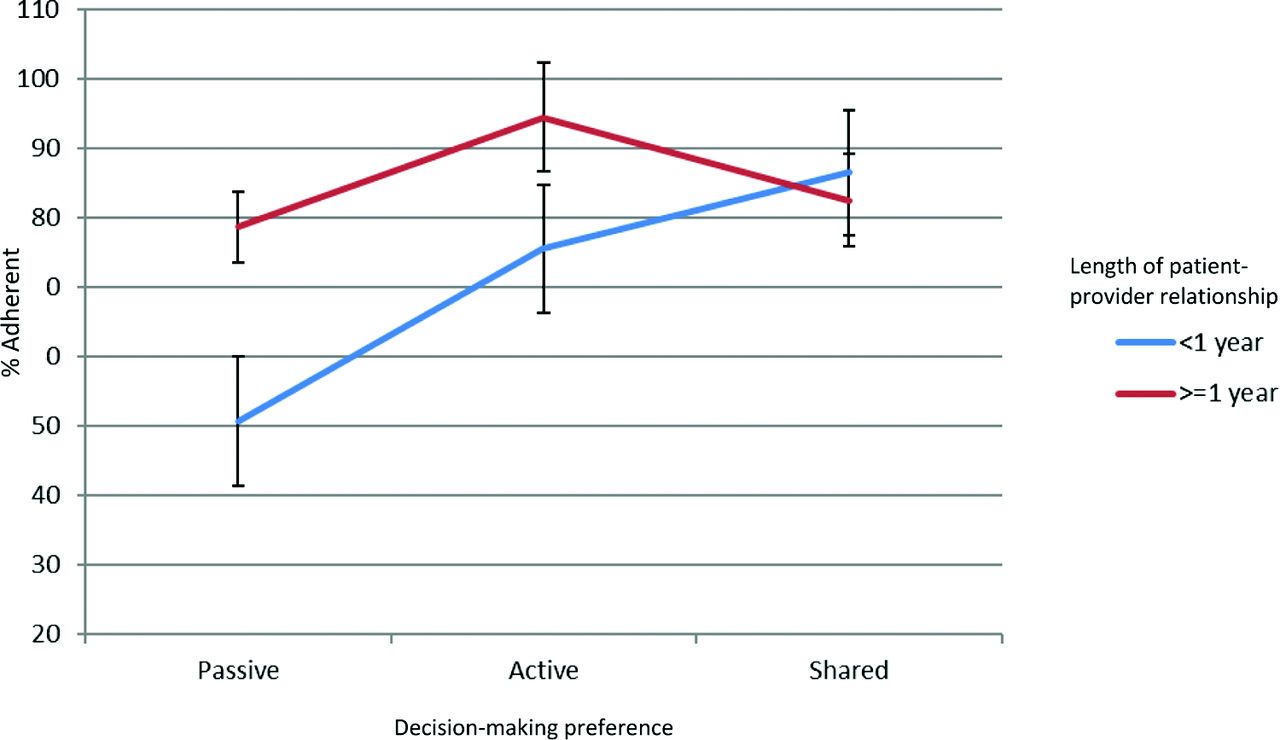
In Model 2, the product of decision-making preference and relationship length was added to Model 1. As shown in Table 4, there was a significant effect modification of the association between preference for SDM and medication adherence by relationship length (B = −28.74 [12.50]; P = .025). The negative relationship indicates that the relative importance of SDM on adherence decreases as the length of the relationship with the provider increases. Length of the patient-provider relationship also had a direct effect on adherence (B = 27.53 [SE:10.93]; P = .01). Post-hoc analysis of the interaction effect indicates that the difference in estimated adherence for the passive decision making group in comparison to the SDM group is significantly different from zero (t(48) = 2.13; P = .038). That is, adherence rates among patients who prefer a passive decision-making style increases to a level similar to those patients who prefer SDM as the length of the relationship increases. The test of this difference is nonsignificant in the shared and active decision-making groups indicating that length of the relationship has no effect on adherence among these patients (t(52) = 1.46; P = .15). Figure 1 displays the results of Model 2.

Effect modification of length of patient-provider relationship on decision-making preference and medication adherence.
Discussion
Findings from this study demonstrate that patient decision-making preference is an important predictor of medication adherence among Black and White patients with hypertension. Specifically, patients exhibited better medication adherence when they preferred a shared or active role in decision making than those preferring to take a passive role. Our findings add to the growing body of research showing that patients with chronic disease who are more active in their health decision making are more likely to be adherent to their prescribed medications; a finding that has been shown to persist 1 year later.11,24,25
Our study extends these findings by examining the length of the patient-provider relationship (ie, longitudinal continuity) as a potential mechanism that links patients' preference for decision making to medication adherence. We found that the additional benefits of preference for a shared role in the decision making process over that of a passive role on adherence was significantly reduced with increasing years of the patient-provider relationship. Our findings suggest several reasons why having an established relationship with the same provider may show benefits in adherence. One possibility is that such longstanding relationships may increase the provider's familiarity with patient's needs and values, which can signal to the patient genuine caring and concern by the provider, and engender patient trust. Previous research has identified patient trust as an important determinant of medication adherence in hypertensive patients.26,27 An established relationship also offers repeated opportunities for patients and providers to develop a therapeutic alliance thereby increasing mutual understanding and respect for 1 another's unique experiences, knowledge, and preferences.28 This creates an environment where patients are comfortable to participate in the decision making process, at their preferred level of involvement, and for providers to offer the appropriate level of decisional support to patients.29
An established patient-provider relationship may be particularly beneficial for chronic disease management in hypertensive patients because continuous care can help reshape patient attitudes and behaviors related to their roles/responsibilities in engaging in decision making about their treatment options, increase patient comfort to disclose nonadherent behaviors, facilitate active involvement in their disease self-management, and build self-efficacy to adhere to treatment recommendations.30⇓⇓–33 This is consistent with a recent review of empirical studies that found patient involvement in decision making that occurred over several sessions with the provider was associated with improvements in psychosocial, (eg, satisfaction with care, trust in physician, confidence in decision), behavioral (eg, diet, exercise, stress management), and health outcomes (eg, blood pressure, quality of life, depression).11
We should note the following limitations: Our study was comprised of predominately low-income Black and White hypertensive patients receiving care in safety-net clinics thus; the findings may not generalize to higher income patients or other racial/ethnic groups. Due to cost constraints, this study only allowed the patient's primary antihypertensive medication to be monitored by the EMD. While this does not reflect adherence rates to other medications, there is evidence that the pattern of adherence to one antihypertensive medication often reflects adherence to others.34 We also examined self-reported preferences for decision making style and not what actually happened during the encounter. In addition, preferences were measured at baseline in the context of one discussion.
There are several implications of this work. First, future research should continue to develop theory-driven models that evaluate the pathways through which decision-making preferences affect patient outcomes.35 Based on this study, interpersonal factors such as patient trust and familiarity as well as organizational factors such as physician turnover and time spent with the patients would be a logical next step.13,31 Our findings, and those of other investigators, also raise the question of whether we should conceptualize patient involvement in decision making as a “preference continuum,” as opposed to a categorical construct. Future research should explore the contextual factors (ie, patient age, health status, context of the decision) that influence patients' desired level of involvement across the continuum.31,36
Second, as suggested by our findings, we recommend continued efforts to increase physician retention in primary care settings to facilitate the development of longitudinal patient-provider relationships. Previous research has documented several benefits of high interpersonal continuity of care including better disease control and lower odds of mortality.37 Alternatively, disruptions in continuity of care due to high physician turnover produce significant negative consequences for patient safety and quality of care.38 For example, low physician retention (the proportion of physicians practicing at a clinic site during a 5-year period) was associated with higher hospital admission rates (19.9% [95% CI, 15.2% to 24.7%]) for ambulatory care–sensitive conditions.39 Such evidence supports the need for models of care such as the Patient Aligned Care Team, which promotes longitudinal patient-provider relationships so patients can benefit from coordinated, continuous care at every clinic visit.40,41
Third, our findings underscore the need for providers to understand and respect patients' preferences for decision making. Importantly, previous research has shown that patients place higher value on the process of engaging with their provider in the context of a caring and supportive patient-provider relationship than their actual ability or desire to participate in the decision making. Increasing longitudinal continuity will enable the development of a patient-centered relationship that ensures patients' desire to be known and involved in care (whether in a shared or passive context) on their own terms are met by the provider. Patient narratives offer 1 method to help providers appreciate patients' decision making preferences and could be used as a training tool to help providers better understand patients' experiences with and preferences for engaging in SDM.42 The Health Experiences Research Group's free online database contains a wide range of patient experiences in video, audio, and transcribed form that could be used for this purpose.43 Patients' preferences for decision making could also be assessed previsit using mobile health (mHealth) technology to help providers' tailor their conversation to each patient.43 Future research is needed to determine whether mHealth applications serve as novel method to foster SDM in the clinic visit or as a detriment to patients who prefer a passive role in the interaction.44
Conclusion
In conclusion, we found that patients exhibit better medication adherence when they preferred to play a shared or active role in decision making than those that preferred to take a passive role. We also found that the relative importance of preference for SDM on adherence decreased as the length of the relationship with the provider increased. The research and clinical implications of this work include training providers in effective communication strategies to identify and support patients' preferred levels of involvement in decision making, offering time-sensitive strategies to incorporate SDM in the clinic visit, and supporting health policies that seek to retain physicians in their practice.45,46
Notes
This article was externally peer reviewed.
Funding: This study was supported by a grant from the National Heart, Lung, and Blood Institute (NHLBI) HLK23HL098564.
Disclaimer: The contents of this article are solely the responsibility of the authors and do not necessarily represent the official views of the National Heart, Lung, and Blood Institute. The funding agency did not play a role in the study design; collection, analysis, and interpretation of data; the preparation of the article; or the decision to submit the article for publication.
Conflict of interest: none declared.
To see this article online, please go to: http://jabfm.org/content/31/5/752.full.
- Received for publication January 8, 2018.
- Revision received May 22, 2018.
- Accepted for publication May 25, 2018.




{kind=link}