
Abstract
Background: Patient-reported outcomes (PROs) are considered potential quality metrics for patients with multiple chronic medical conditions (MCC). Although continuity of care (COC) is an essential MCC care process, the association between common PROs and COC is unknown.
Methods: We assessed baseline and two-year follow-up self-reported health status, physical, and emotional well-being, and COC in seniors with MCC. Using mixed effects models with repeated measures adjusting for age, gender, and morbidity, we assessed each outcome as a function of COC.
Results: Of 2,078 seniors, 961 completed the initial survey and 806 completed follow-up. On a 0–100 scale, mean (sd) baseline self-reported health status, physical well-being, and emotional well-being were 48.7 (22.0), 36.4 (11.4), and 54.8 (9.0). On a 0 to 1 scale, mean baseline and 2-year COC were 0.24 (sd 0.22) and 0.22 (0.18). Follow-up self-reported health status, physical well-being, and emotional well-being were 48.8 (23.1), 36.5 (11.5), and 55.3 (8.8). In adjusted primary and secondary analyses using all available data, there were no associations between any outcomes and COC.
Conclusion: Given the measurement burden of quality assessment, negative associations between potential quality metrics and care processes are informative. Systematic assessment of PROs can inform patient-centered MCC care. However, PRO scores should be used with caution as quality measures.
- Chronic Disease
- Comorbidity
- Continuity of Care
- Follow-up Studies
- Health Status
- Patient-Reported Outcome Measures
- Quality of Life
- Quality of Health Care
- Self Report
- Surveys and Questionnaires
Patient-reported outcome (PRO) measures such as self-reported health status and physical and emotional well-being are increasingly promoted as potential measures of care quality.1⇓⇓⇓⇓⇓–7 Because PROs capture domains that cross conditions and reflect patient-centered priorities, such measures may more accurately reflect the health and well-being of individuals with multiple chronic medical conditions (MCCs) than do common disease-specific quality measures.8,9 Across populations, higher scores on these and other domains of health-related quality of life (HRQOL) correlate with lower rates of hospitalization, lower overall mortality, lower cardiovascular morbidity, and lower outpatient services utilization in populations of patients with chronic illness.10⇓–12
Although PROs may accurately capture the health of individuals with MCCs, promoting them as quality measures implies that there is evidence linking recommended care processes to these outcomes, and that measuring PROs can evaluate and inform the delivery of care.13,14 However, it is unclear whether recommended elements of care delivery for patients with MCCs affect the most commonly measured PROs that capture domains of HRQOL. Health status, functional status, and emotional well-being are multifactorial constructs, and scores may or may not change based on receiving high- or low-quality care.
One care process that is essential to high-quality care for MCCs is optimal continuity of care (COC). For the population with MCCs, greater COC is associated with lower rates of hospitalization and emergency service use, better control of chronic diseases, greater patient satisfaction, greater patient trust and communication with one's physician, and lower mortality rates.15⇓⇓–18 Although it has been suggested that patient-reported HRQOL could reflect care processes specifically including COC, this specific association has not been evaluated.19
Given this gap in knowledge, we investigated the longitudinal association between COC and 3 domains of HRQOL: self-reported health status, functional status, and emotional well-being. We hypothesized that if there is an association between COC and HRQOL, greater COC would be associated with better HRQOL in a population of seniors with MCCs.
Methods
Study Design and Setting
We conducted a 2-year prospective telephone survey to assess HRQOL as a function of interpersonal COC among patients in Kaiser Permanente Colorado, a not-for-profit, integrated health care delivery system. The Institutional Review Board of Kaiser Permanente Colorado reviewed and approved the study.
Study Population
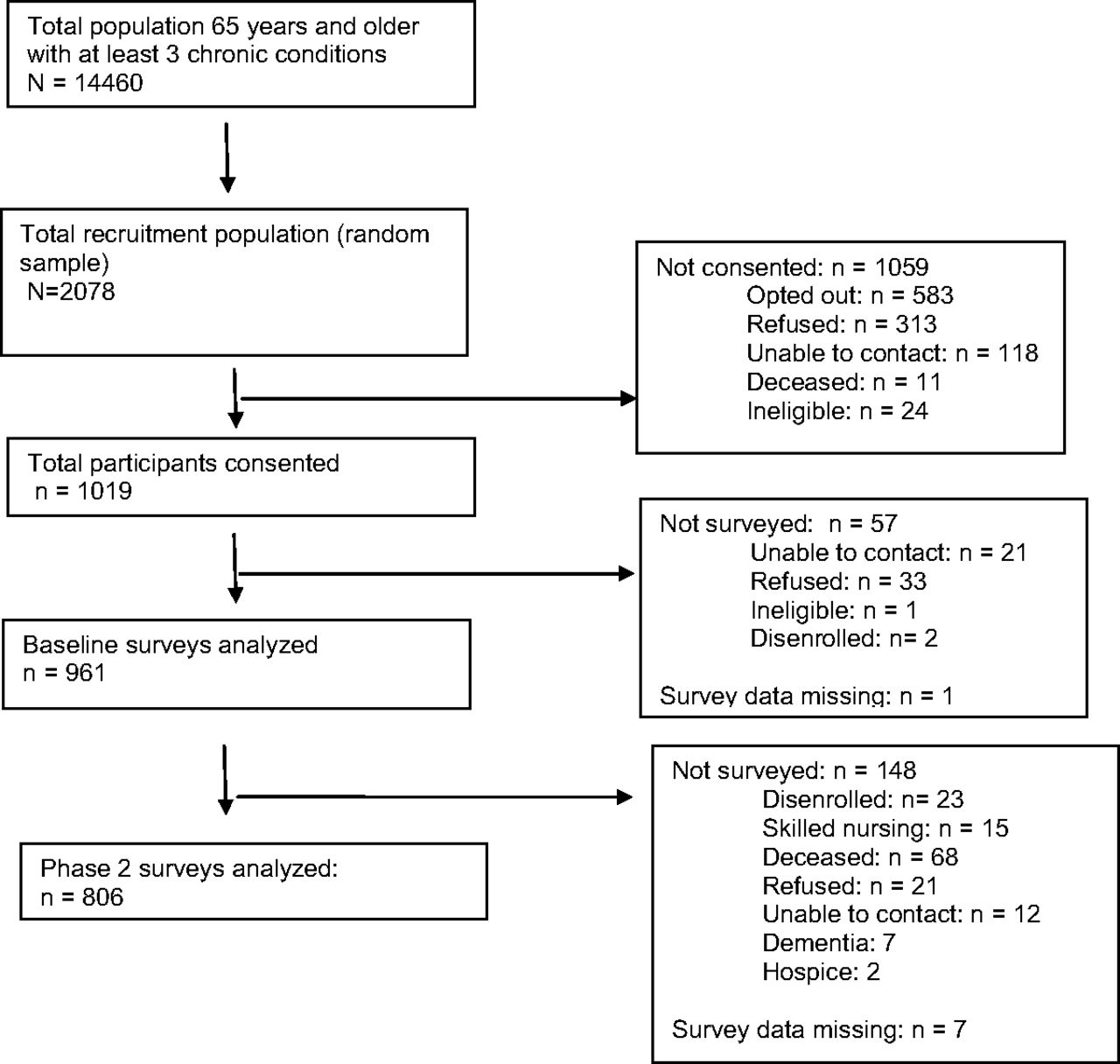
The study population consisted of 961 survey respondents from among a random sample of 2078 adult members of Kaiser Permanente Colorado who were aged ≥65 years on January 1, 2010; had at least 1 year of enrollment before and at least 2 years of enrollment following this date; and had ≥3 of 10 common chronic medical conditions. We excluded individuals with a diagnosis of dementia or who recently or currently required skilled nursing care. Respondents were, on average, 1 year younger than nonrespondents; the 2 groups did not differ with regard to diagnosis-based morbidity level or sex.
Measures
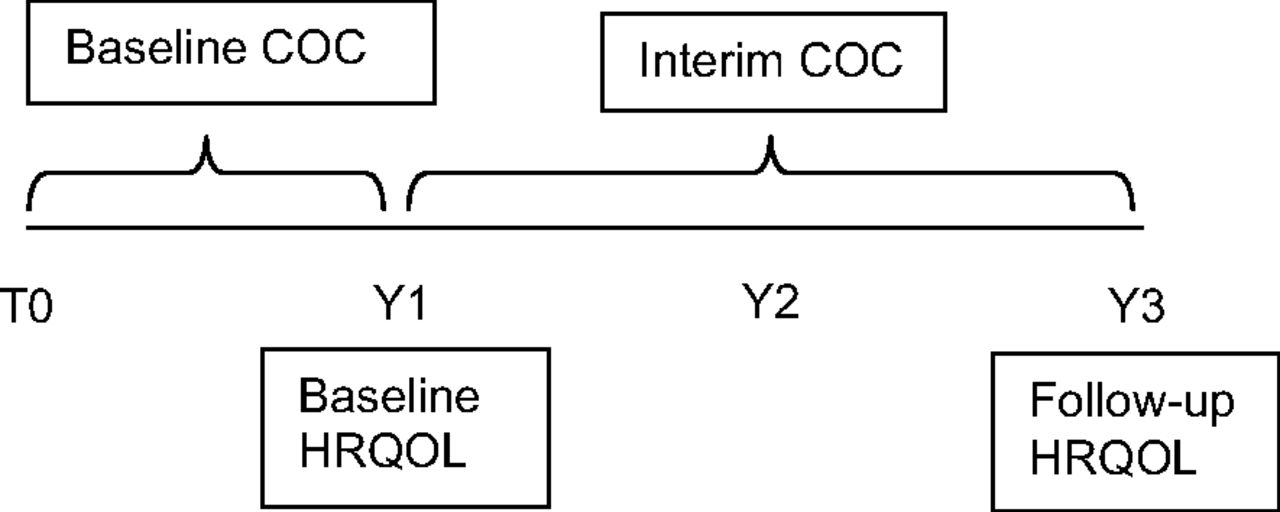
HRQOL was measured at baseline and 2 years later using the 36-item Rand questionnaire to assess self-reported health status, physical function, and emotional well-being.5 We measured interpersonal COC using the COC Index (COCI),20 which captures the concentration of visits to individual providers and is sensitive to the number of providers seen—which is particularly relevant to individuals with multimorbidity. The COCI formula is as follows: COCI = ∑sj = 1nj2 − N/N(N − 1), where N is the total number of visits, nj is the number of visits to provider j, and s is the total number of providers seen. Calculating a stable COCI value requires ≥3 visits. Therefore, for each outcome, we required ≥3 outpatient visits to a primary and/or specialty care clinician during each measurement period. COC was measured during the year before baseline and during the 2-year period between baseline and follow-up. Thus each respondent had up to 2 measures of COC and HRQOL, with each COC measure temporally preceding each measure of HRQOL (Figure 1). Chronic conditions were identified by International Classification of Diseases, Ninth Revision codes listed in the electronic health record during the year before baseline.
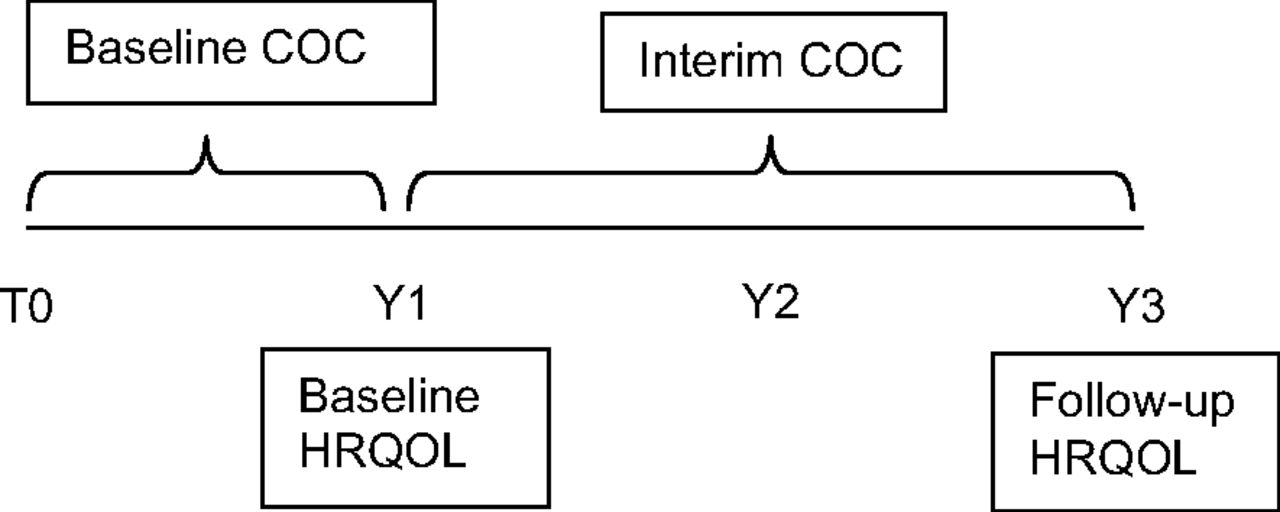
Measurement timeline for health-related quality of life (HRQOL) domains and continuity of care (COC). T0, Time zero; Y1, year 1; Y2, year 2; Y3, year 3.
Analysis
To assess the domains of HRQOL as a function of COC and time, we used a mixed effects model with a maximum likelihood estimation approach to analyze repeated HRQOL measures collected at baseline and follow-up, adjusting for age, sex, and morbidity burden. We also conducted secondary analyses using multiple imputation to account for missing data. Both maximum likelihood and multiple imputation methods assume data are missing at random, which allows the probability of missingness to depend on observed data and not on missing data.21,22 Given the number of predictors we considered in the regression model, the sample size in our study population provided 80% power to detect a small effect size (R2 = 0.02) at α = 0.05.23 This effect size is consistent with minimally clinically significant differences in HRQOL scores.24
Results
Of the 961 seniors who responded to the initial survey, 806 completed the 2-year follow-up. Figure 2 illustrates cohort development and Table 1 describes population characteristics. Losses to follow-up were primarily the result of death (n = 68); ineligibility because of dementia, skilled nursing care, or disenrollment (n = 45); and refusal (n = 21). On a normed scale of 0 to 100, mean (standard deviation) self-reported health status, physical well-being, and emotional well-being were 48.7 (22.0), 36.4 (11.4), and 54.8 (9.0), respectively, at baseline. Among cohort members with enough visits to calculate COCI, mean overall COCI was 0.24 (0.22) on a 0-to-1 scale at baseline and 0.22 (0.18) during the 2-year follow-up. Minimal change in HRQOL domains occurred over 2 years. Mean (standard deviation) self-reported health status, physical well-being, and emotional well-being during follow-up were 59.6 (21.2), 36.5 (11.5), and 55.3 (8.8), respectively.

Consort diagram.
Demographic, Clinical, and Outcome Characteristics of Seniors with Multiple Chronic Conditions at Baseline (2010) (N = 961)
In adjusted repeated measures analyses using all available data, there was no significant association between any of the HRQOL domains and COC (Table 2). Greater morbidity burden was negatively associated with self-reported health status and physical and emotional well-being. There was minimal change in calculated morbidity level from baseline to follow-up. Female sex and older age were also negatively associated with physical well-being.
Adjusted Associations Between Health-Related Quality of Life and Continuity of Care
Participants with missing follow-up data because of disenrollment or reasons other than death had baseline characteristics similar to those with complete follow-up. Participants with missing follow-up data because of death were older, had greater morbidity, and had worse health status at baseline than those with completed follow-up (P < .001 for all). The lack of an association between COC and HRQOL did not change in secondary analyses using multiple imputation.
Discussion
In a health care delivery culture of substantial primary care measurement burden and misguided quality incentives, negative associations between potential quality metrics and important care processes are informative. PROs have been promoted as a means to evaluate the effect of clinical processes and interventions on elements of health and well-being.27 Based on this analysis, self-reported health status and physical and emotional well-being do not seem to be associated with COC. This suggests that these well-validated and easily quantifiable PROs may not accurately reflect the important processes of care for MCCs and should be used with caution as a broad quality measure for this population.
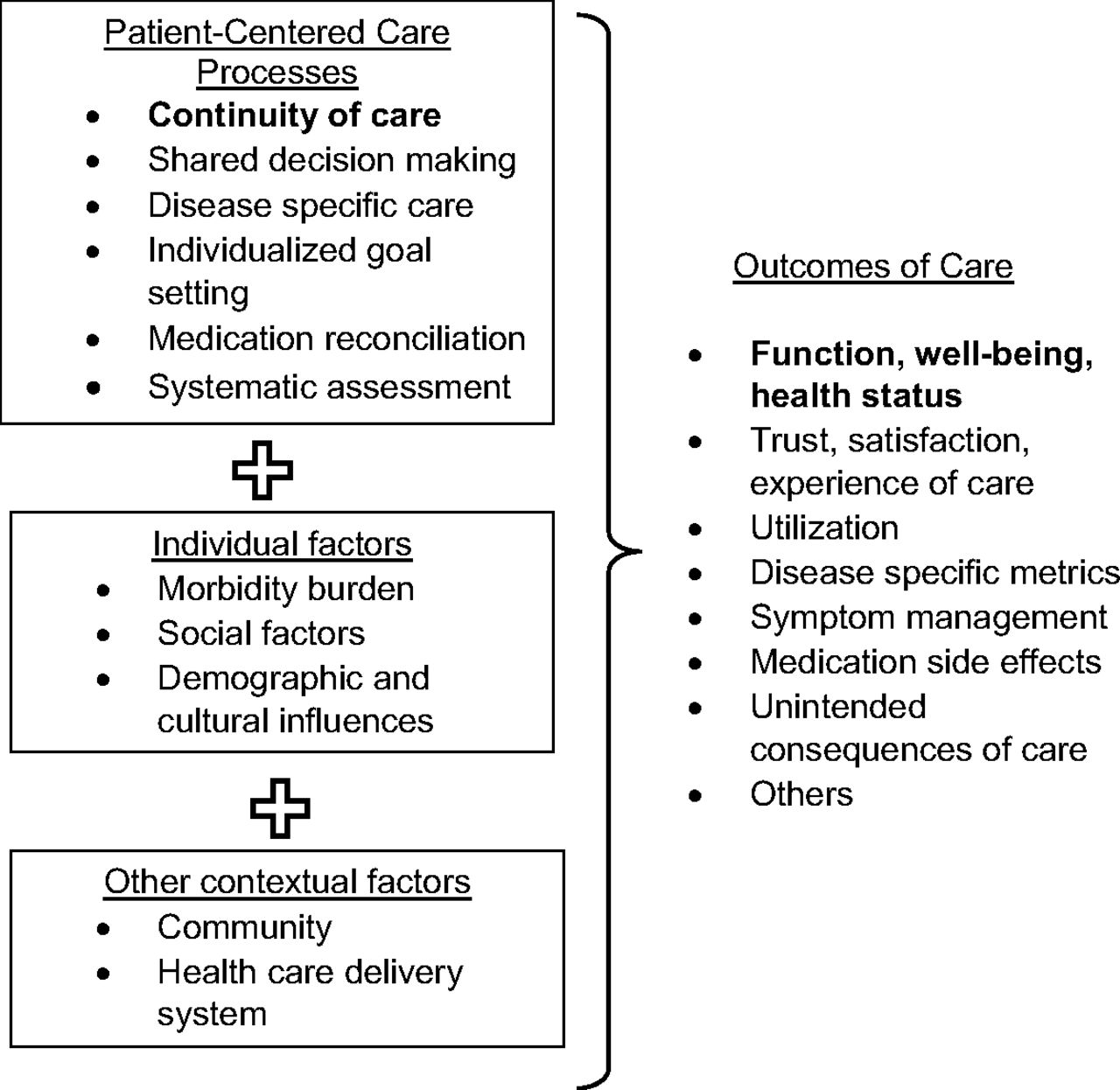
National Quality Forum criteria for developing quality measures from PROs specifies that they be psychometrically sound, person-centered, meaningful, and amenable to change.2 Importantly, they must also be valid and responsive to the care process or intervention.2,28 This has been demonstrated for physical and emotional well-being scores in response to specific interventions such as joint replacement and depression treatment.29,30 In our analysis, health status and physical and emotional well-being as functions of COC did not meet these criteria. In the context of primary care delivery especially, care processes and outcomes are multifactorial (Figure 3). As an outcome, HRQOL is a broad construct that reflects biological factors, functional status, social and emotional well-being, environmental influences, expectations of health, and disease-specific symptoms.31⇓⇓–34 Although HRQOL is associated with morbidity burden as measured by diagnoses, diagnosed conditions account for only part of overall HRQOL.35 As a care process, COC is only 1 aspect of patient-centered care that may affect health outcomes, and even optimal chronic disease care may not markedly affect overall morbidity burden—especially in the short term.34 Generating evidence to promote optimal care for individuals with MCCs requires an understanding of the multiple and complex associations between these processes and outcomes.

Example processes and outcomes relevant to the care of individuals with multiple chronic conditions.
When asked, patients with MCCs describe high-quality care as being empathic and respectful, thorough, continuous, efficient, safe, and of high technical quality.35⇓⇓⇓–39 Systematically assessing patient-reported information as part of an annual health assessment can guide patient-centered care and shared decision making.40 When PROs have been systematically integrated into care delivery, patients find the ensuing discussions helpful and patient-centered.41 However, assessing and acting on patient-reported information may not change individual or population-level scores of the measures themselves.27,34,42,43 Thus it may be the process of PRO assessment and clinical action that reflects high-quality care and not necessarily the change in PRO score. This interpretation of PRO use is consistent with calls for “reimagining” quality assessment to focus on measuring important processes, with less emphasis on outcomes.44
Our study has several limitations. All methods for managing missing data have inherent limitations. Some of our HRQOL data were missing because of death or functional decline, and some COC data were missing because of less contact with the system among individuals with lower morbidity. We followed literature-based recommendations for managing missing data under general missing-at-random conditions, but other methods such as assigning zero values to HRQOL variables for known decedents have also been proposed.21,45 Based on primary and secondary analyses, we think it is unlikely that we missed a significant association between COC and HRQOL. Because our study was conducted in an integrated delivery system with a common electronic health record, our COC scores reflect relational continuity of care within that system; however, interpersonal COC remains relevant and improves outcomes within integrated systems.15 Our participants' mean COC score was in the low-to-medium range for geriatric populations.17,46 This likely does not reflect underascertainment, as claims data supplements electronic health record data to capture all primary and specialty care. Associations between HROQL and COC may differ in nonintegrated delivery settings or for populations with different distributions of COC and HRQOL. Finally, we only assessed the relationship between 3 domains of HRQOL and 1 important process of care. Further research is required to understand the multidimensional relationships between PROs and other care processes to adequately inform the use of PROs as a quality indicator for complex patient care.
Conclusions
Our findings illustrate the importance of selecting appropriate measures to evaluate and promote patient-centered care—especially for complex patient populations who benefit from multidimensional approaches to care delivery. Although systematic assessment of PROs can and should inform optimal care, assessing and acting on PROs may be more reflective of high-quality care for MCCs than the specific scores themselves, which may not reflect important care processes such as high COC.
Notes
This article was externally peer reviewed.
Funding: This investigation was funded by the Agency for Healthcare Research and Quality (1R01 HS018404–01).
Conflict of interest: none declared.
Disclaimer: The funder had no role in the study design; collection, analysis, and interpretation of data; writing of the report; or decision to submit the article for publication.
To see this article online, please go to: http://jabfm.org/content/30/2/205.full.
- Received for publication July 13, 2016.
- Revision received October 25, 2016.
- Accepted for publication November 1, 2016.




{kind=link}
{kind=link}
{kind=link}