
Abstract
Introduction: While most physicians recognize that vitamin D status varies by skin color because darker skin requires more light to synthesize vitamin D than lighter skin, the importance of body weight to vitamin D status is a newer, less recognized, finding. The purpose of this study was to use nationally representative US data to determine the probability of vitamin D deficiency by body weight and skin color.
Methods: Using data for individuals age ≥6 years from the 2001 to 2010 cycles of the US National Health and Nutrition Examination Survey, we calculated the effect of skin color, body weight, and age on vitamin D status. We determined the probability of deficiency within the normal range of body weight for 3 race/ethnicity groups at 3 target levels of 25-hydroxyvitamin D.
Results: Darker skin colors and heavier body weights are independently and significantly associated with poorer vitamin D status. We report graphically the probability of vitamin D deficiency by body weight and skin color at vitamin D targets of 20 and 30 ng/mL.
Conclusion: The effects of skin color and body weight on vitamin D status are large both statistically and clinically. Knowledge of these effects may facilitate diagnosis of vitamin D deficiency.
Vitamin D may be more important to human health than previously recognized. Inside cells, gene activity is controlled by nuclear receptors. The vitamin D nuclear receptor responds to at least 3 vitamin D compounds in humans: the storage form 25-hydroxyvitamin D (25[OH]D), the classically active form 1,25-dihydroxyvitamin D, and the breakdown form 24R,25-dihydroxyvitamin D. With some overlap, each form regulates different genes.1 Estimates of the vitamin D receptor's importance in humans vary, but it seems to control, either directly or indirectly, up to 2000 of the approximately 20,000 to 25,000 human genes.2
Research suggests that the impact of vitamin D status on human health is large enough to have played a remarkable role in human evolution. Anthropologists regard human skin color as an evolutionary adaptation to ultraviolet light.3 The theory posits that dark skin is protective against the intense sunlight at the equator but that at other latitudes individuals with lighter skin have the evolutionary advantage of better health. This is because their sunlight-dependent vitamin D concentrations are closer to those of the ancestral, dark-skinned, equatorial population. Thus the geographic intensity of sunlight and its health impact produce the spectrum of human skin colors we see as we move away from the equator.
From a health perspective, this theory implies that health disparities are found in all populations with diverse skin colors.3⇓–5 In areas of intense sunlight, those with lighter skin are disadvantaged. In areas like the United States, those with darker skin have poorer health. Yet the theory also implies that health professionals can readily take action to alleviate these health disparities: sun protection for those with light skin where sunlight is intense, and vitamin D supplements for those with dark skin everywhere else.
As the theory suggests, at the latitude of the United States, those with darker skin colors actually have much lower vitamin D concentrations than those with lighter skin. For US individuals age 6 years and older, average 25(OH)D concentrations are 17.4 ng/mL for non-Hispanic blacks, whereas Mexican Americans average 26% higher at 21.9 ng/mL and non-Hispanic whites average 62% higher at 28.3 ng/mL (Table 1). In terms of sun protection, on the other hand, invasive melanoma is 24.7 times more likely among US non-Hispanic whites than US blacks.6 Ghanaian farmers living near the equator (6° N) have an average concentration of 30 ng/mL,7 while dark-skinned people living traditionally in east Africa (4° S), who provide the best estimate of vitamin D concentrations over the course of human evolution, have an average concentration of 46 ng/mL.8
In addition to skin color, body weight has an important impact on vitamin D status because of the effect of dilution.9⇓–11 Vitamin D is measured as a concentration (weight/volume), so larger individuals need more vitamin D to obtain the same concentration as smaller individuals. Research suggests that body weight is a better index of this dilution than body mass index.9⇓–11 Many of the diseases and conditions associated with vitamin D deficiency are also associated with race- and obesity-related health problems. Given the potential benefits of optimal vitamin D status and the large impact of skin color and body weight on 25(OH)D status, we focused our research on calculating the probability of vitamin D deficiency by body weight and skin color using nationally representative US data.
Methods
We used data from a subset of the nationally representative continuous version of the US National Health and Nutrition Examination Survey (NHANES), which is collected by the National Center for Health Statistics, a unit of the Centers for Disease Control and Prevention.12 The National Center for Health Statistics Ethics Review Board approved the NHANES data collection protocols, and the institutional review board of the Teachers College, Columbia University, approved our work with NHANES. NHANES researchers collect data on a 2-year cycle, selecting individuals using complex survey methodology, which creates a nationally representative random sample of the noninstitutionalized US population. Details of the complex NHANES design are presented elsewhere.13
Five 2-year cycles of NHANES (from 2001 to 2010) include serum 25(OH)D measures for individuals age 6 years and above. Data for those older than 1 year are also available in all but the first of these 5 cycles, 2001 to 2002. In this analysis we did not use any of the data for 1- to 5-year-olds so that we could include the 2001–2002 data. For the first 3 cycles, assays were completed using the DiaSorin RIA kit (Saluggia, Italy). For the final 2 cycles, NHANES researchers used standardized liquid chromatography–tandem mass spectrometry traceable to National Institute of Standards reference materials, which only recently became available (http://www.nist.gov/mml/csd/vitamind_071409.cfm). NHANES researchers adjusted values from the DiaSorin assays upward to more closely match the standardized assay.14 This analysis uses the adjusted serum 25(OH)D values. All values were converted from nanomoles per liter to nanograms per milliliter, the serum 25(OH)D reporting standard used by US laboratories, by dividing by 2.496.
The NHANES race/ethnicity variable provides nationally representative data for non-Hispanic blacks, Mexican Americans, and non-Hispanic whites, which we use as a proxy for skin color. Our analysis also included sex, age in years, body weight in kilograms, and the appropriate complex survey weight for each case. After listwise deletion of cases with missing data, NHANES provided 36,434 (unweighted) cases for our analysis.
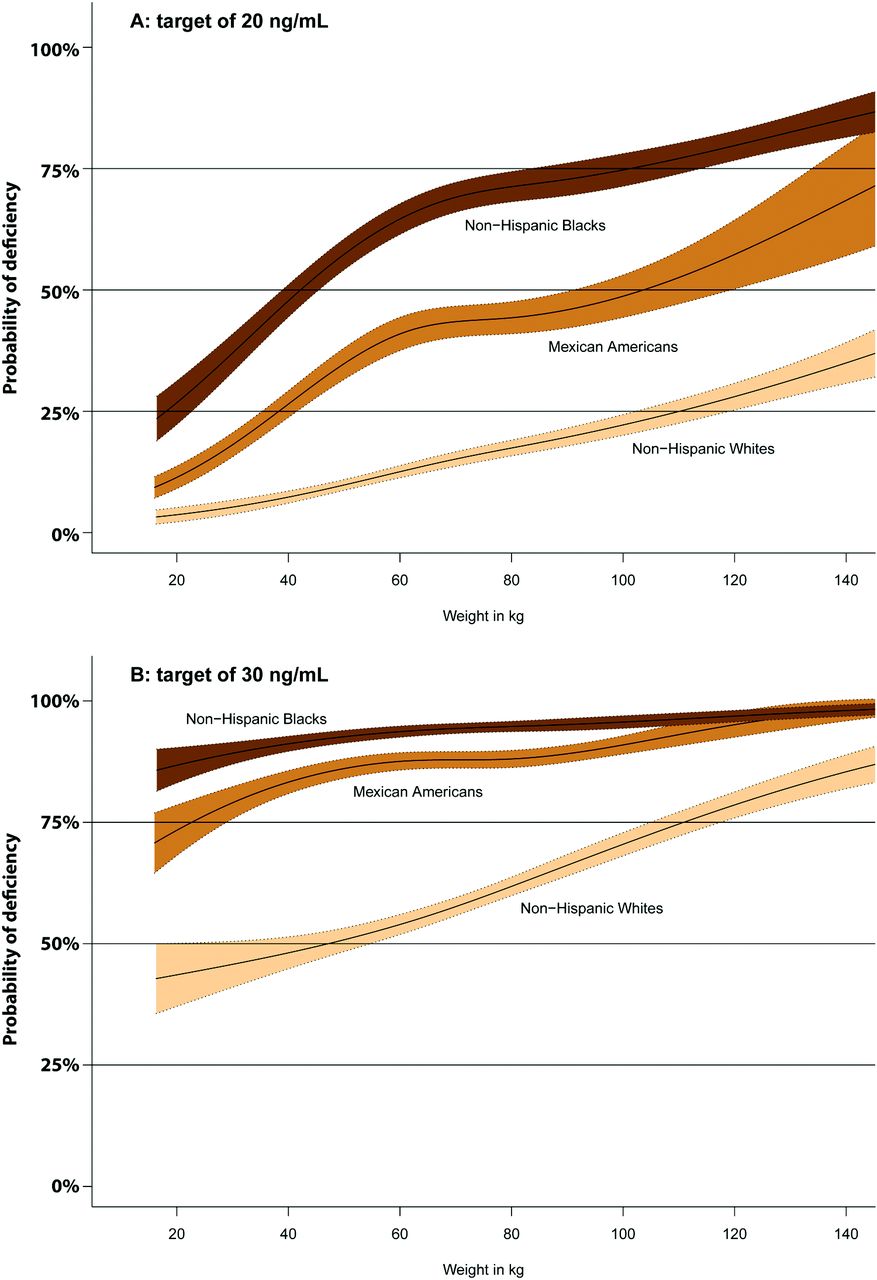
We used the statistical program R, version 3.2.1 (R Foundation for Statistical Computing, Vienna, Austria) and its Survey package (version 3.30), which is appropriate for analyzing complex survey data.15 We created Figure 1 using nonlinear logistic regression based on natural B-splines. That analysis provides the estimated probability that individuals are deficient at various serum 25(OH)D targets across typical body weights by skin color, as well as estimated standard errors, from which we calculated 95% confidence intervals.
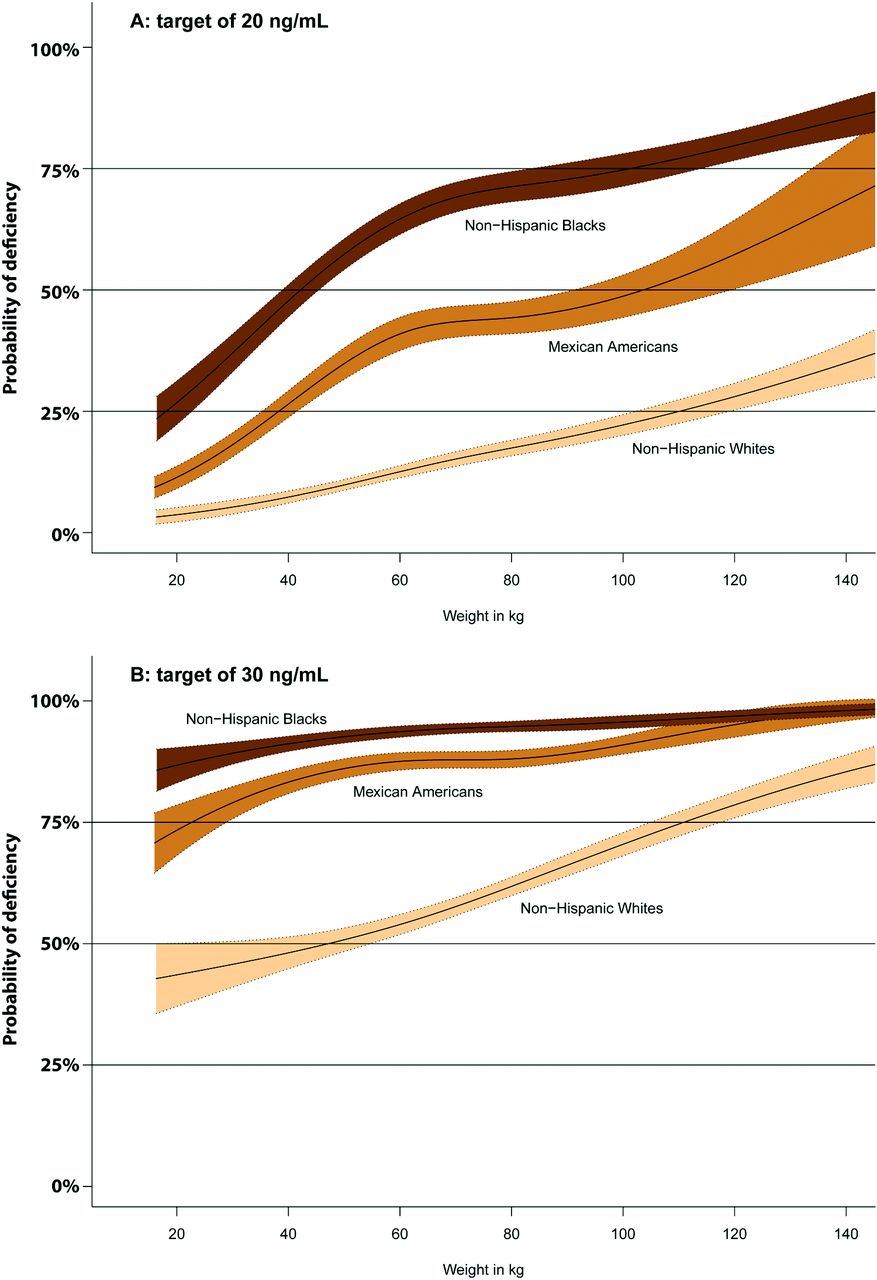
Probability of vitamin D deficiency by body weight and skin color at 2 target 25-hydroxyvitamin D (25[OH]D) concentrations: below 20 ng/mL (A) and below 30 ng/mL (B). If vitamin D deficiency is defined as a 25(OH)D concentration below 40 ng/mL, all 3 lines hug the top of the graph, so that figure is not shown. Bands indicate 95% confidence intervals for the probability of deficiency.
Results
Table 1 shows the demographic characteristics of our data set, which is representative of the noninstitutionalized US population aged ≥6 years in the 2001 to 2010 time frame.13,14,16 The first column shows the unweighted number of subjects in each group (some groups were oversampled compared with their presence in the population; weights are used to correct for this and other issues related to obtaining the nationally representative estimates presented in the remaining columns). This is followed by the mean 25(OH)D concentration of the group and its standard error. The following columns show the percentage distribution of each line in the table by 3 vitamin D status groups. For example, considering the column showing 25(OH)D status <20 ng/mL, note that while 27% of the entire population is in this deficient group, it includes 68% of non-Hispanic blacks and 50% of those who weigh >125 kg. In contrast to the very large differences by weight and skin color, the differences by sex and by age after childhood are unremarkable.
The 2 plots in Figure 1 show the probability that an individual in the US population is vitamin D deficient at two target levels of deficiency—below 20 and below 30 ng/mL—by body weight and skin color. The plots also show 95% confidence intervals for the probability estimates. Where the confidence intervals are wider, there are fewer individuals in the population with the corresponding body weight and skin color. Non-Hispanic blacks are more likely to be deficient at all weight levels, followed by Mexican Americans. Figure 1A shows the probability of deficiency at a target of below 20 ng/mL. In Figure 1B the deficiency target is below 30 ng/mL. At a target of below 40 ng/mL, all 3 lines hug the top of the chart between 85% and 100% at all points, indicating that everyone in the US population who is not already using ample vitamin D supplementation would need to do so, so that plot is not shown.
Discussion
We present results at 3 different 25(OH)D concentrations because the optimal concentration of 25(OH)D in humans is currently controversial. In part this is because, at the highest suggested concentration of 40 ng/mL, virtually the entire US population would be deemed vitamin D deficient. Even at a suggested concentration of 30 ng/mL, virtually all adult non-Hispanic blacks would be considered vitamin D deficient. Moreover, some research suggests that the optimal concentration of 25(OH)D is not the same in the context of different diseases.17
In late 2010 the Institute of Medicine's Committee to Review Dietary Intakes for Vitamin D and Calcium suggested 20 ng/mL as an appropriate average population concentration for bone health, but said more randomized controlled trials (RCTs) would have to be conducted before it could determine an appropriate level for the other functions of vitamin D.18 The Endocrine Society later released RCT-based guidelines recommending a minimum of 30 ng/mL.19 The Vitamin D Council says that epidemiologic data suggest concentrations in the 50- to 80-ng/mL range are sufficient.20
In addition to body weight and skin color, other determinants of vitamin D status include season, sunlight intensity and exposure, and use of vitamin D supplements.21⇓⇓–24 Research suggests that low vitamin D in obese women is not caused by reduced sun exposure.25 In addition, US health professionals consider age to be the primary determinant of vitamin D status. For example, the Institute of Medicine's Committee to Review Dietary Intakes for Vitamin D and Calcium recommended different vitamin D intakes for those <1 year of age (400 IU/day), those ages 1 to 70 years (600 IU/day), and those over age 70 years (800 IU/day), but made no recommendations by weight or skin color.18 Although it is generally known among health professionals that African Americans have lower vitamin D concentrations than white Americans, the impact of skin color on vitamin D status is considered to be unremarkable compared with the impact of age. The impact of body weight on vitamin D status is a more recent discovery that is still unknown to most health professionals. Furthermore, in an article accepted for publication in Public Health Nutrition, our research group has shown that the apparent effect of age on vitamin D status is quite small after controlling for body weight.
Skin color is important to dosing only because those with darker skin have lower baseline vitamin D concentrations.26,27 A recently reported 3-month dose-response study of African Americans by Ng and colleagues28 did not consider or report body weight, but the average body mass index of the participants was 31.2 kg/m2. Three treatment groups received doses of 1000, 2000, and 4000 IU/day and achieved 25(OH)D concentrations of 29.7 (up 13.5 from this group's baseline), 34.8 (up 20.9), and 45.9 ng/mL (up 30.2 ng/mL), respectively.
Body weight, on the other hand, is important to dosing both because of lower baseline values and because heavier individuals have a lower response to a given dose than lighter individuals. Drincic and colleagues,9 who have been at the forefront of emphasizing the importance of body weight to vitamin D status, have done a study using doses of 1000, 5000, and 10,000 IU for 21 weeks in 62 obese white subjects.29 They suggest a reasonable starting dose of vitamin D3 is 2.5 IU/kg body weight/1 ng/mL of desired increase in 25(OH)D concentration. Singh and Bonham27 more recently published a detailed dosing formula based on results seen in actual health care settings. In the United States vitamin D3 supplements are typically available over the counter in 5000-, 2000-, 1000-IU, and smaller doses; consequently, a calculated result must be adjusted to a workable supplement size before advising the patient. Vitamin D3 is the animal form of vitamin D and is also produced by some plants.30 Vitamin D2, which is used in formulations available by prescription in the United States, is produced by yeast and fungi and is less effective at increasing 25(OH)D concentrations.11 Drincic and colleagues also emphasize that there is a very large amount of individual variation in response to 25(OH)D dose. They suggest that clinicians should rely on a subsequent serum 25(OH)D test to assess the accuracy of a calculated dose.
Until recently there has been a great deal of concern related to vitamin D toxicity in the context of supplementation. However, actual cases of vitamin D toxicity are extremely rare and typically result in complete recovery after the source of excessive vitamin D is discovered and removed.31,32 In general, reported cases result from compounding or manufacturing errors that could happen with any drug or supplement and are not specific to vitamin D. Concerns about vitamin D's toxicity date to the 1950s, when unusual cases of idiopathic infantile hypercalcemia occurred soon after foods were fortified with vitamin D. Recent genetic studies have clarified that idiopathic infantile hypercalcemia is related to a mutation in the CYP24A1 gene, which produces the enzyme that metabolizes 25(OH)D and 1,25-dihydroxyvitamin D.33 Individuals with this mutation or with diseases known to lead to high calcium concentrations, such as sarcoidosis and lymphoma, should receive vitamin D supplementation only under medical supervision.
Moreover, many individuals do not follow professional advice to take vitamin D supplements. Research to date has found only 1 technique that has a major impact on supplement adherence: providing the recommended supplement dose on a prescription form.34
Limitations
US health policy panels have said that it is premature to recommend that African Americans increase their vitamin D concentrations because of a lack of evidence from RCTs.18 On the other hand, such panels rely almost entirely on epidemiologic evidence to recommend sun protection, which primarily benefits those with light skin.6 A reasonable approach would be to use the same standard of evidence for all sunlight-related health consequences rather than different standards for different groups.
In 2013 Powe and colleagues35 published an article in the New England Journal of Medicine suggesting that
low total 25(OH)D levels do not uniformly indicate vitamin D deficiency and call into question routine supplementation in persons with low levels of both total 25(OH)D and vitamin D binding protein [that is, African Americans] who lack other traditional manifestations of this condition…. Labeling the majority of the black participants as vitamin D-deficient would be inconsistent with the observation that they had higher bone mineral density, higher calcium levels, and only slightly higher parathyroid hormone levels than their white counterparts.
However, their conclusions may be premature. The higher bone mineral densities and calcium concentrations among US blacks were well known36 before the study by Powe et al.35 They had been and are considered a paradox. The results of the study by Powe et al do not explain this paradox, although other theories do.37 Powe et al's theory of bioavailable vitamin D is only one of multiple theories suggesting how vitamin D compounds cross the cellular membrane—all of which may be true. Individuals with dark skin living near the equator in Africa have much higher vitamin D concentrations than any group in the United States, indicating that sunlight intensity accounts for the higher concentrations. The study by Powe et al suggests instead that the genetics of vitamin D binding protein in African-origin populations accounts for the low vitamin D concentrations found in African Americans. In that case we would expect to find those same low concentrations in Africa, but we do not.7,8 Importantly, there is evidence of an association between vitamin D status and US racial health disparities.3⇓–5 Finally, Powe et al limited their discussion to bone health and did not consider any other effects vitamin D may have on human health.
The results of this study apply to the US population and should not be assumed to be relevant in other countries. In addition, because researchers have only recently realized the importance of body weight to vitamin D dosage requirements, there are currently no vitamin D dose-response studies in the literature that combine both body weight and skin color. Additional research on larger groups, covering a wider range of body weights and baseline and target vitamin D concentrations, is needed to clarify dosage recommendations.
Conclusions
The effects of skin color and body weight on vitamin D status are large, both statistically and clinically. At typical target concentrations of deficiency (below 20 or below 30 ng/mL), those with darker skin colors or heavier body weights have a higher probability of being vitamin D deficient. Knowledge of these effects may facilitate the diagnosis of vitamin D deficiency.
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: TW has an intellectual passion about vitamin D and has an unpaid, volunteer relationship with the Vitamin D Council. The other authors have no conflicts of interest.
- Received for publication August 10, 2015.
- Revision received November 12, 2015.
- Accepted for publication November 17, 2015.




{kind=link}