
Abstract
Introduction: The diagnosis of streptococcal infection is usually made with the use of Centor criteria, but some family doctors also rely on the determination of C-reactive protein (CRP) to guide antibiotic therapy.
Methods: This was an observational study conducted in a health center. Adults with acute pharyngitis and the presence of the 4 Centor criteria (tonsillar exudates, tender cervical glands, history of fever, and absence of cough) were recruited. The patients underwent a pharyngotonsillar swab for microbiologic study and a CRP rapid test during the consultation.
Results: A total of 149 patients were enrolled. The most frequent etiology was group A streptococcus, present in 83 cases (55.7%). The highest CRP concentration was observed among patients with group C streptococcus infection, with a mean of 56.3 mg/L (95% confidence interval, 25.7–86.5 mg/L). For patients with group A streptococcus infection, the mean CRP value was 34.4 (95% confidence interval, 25.6–43.3 mg/L).
Conclusion: CRP concentrations are not associated with group A streptococcus infection in patients with acute pharyngitis. The use of this point of care test is therefore not useful for distinguishing patients who require antibiotic therapy.
Point-of -care testing for C-reactive protein (CRP) was introduced into community clinical practice in the early 1990s and is widely used in Scandinavian countries.1 This test provides results in about 3 minutes and guides decisions regarding antibiotic treatment. Several randomized clinical trials and observational studies have found that CRP rapid testing significantly reduces the prescription of antibiotics to patients with lower respiratory tract infections2; several studies have shown that elevated CRP concentrations are associated with bacterial etiology.3 Among patients with acute pharyngitis, only those infections caused by group A streptococcus (GAS) should be treated with antibiotics.4 However, some series have shown a high prevalence of non-GAS infection, and complications after infections caused by groups C and G streptococci have been reported.5 In some countries, this diagnosis is conducted with the aid of rapid antigen detection tests, but because of the uncertainty of infections caused by streptococci other than GAS, some physicians also rely on CRP to guide antibiotic treatment, despite the use of this test not being recommended in such situations.1 We conducted a study aimed at understanding the relationship between the etiology of sore throat and CRP concentrations in patients with suspected streptococcal infection.
Methods
An observational study was undertaken in an urban health center from January 2010 to May 2012. Adults ≥18 years old with acute pharyngitis and the presence of the 4 Centor criteria6—history of fever, presence of tonsillar exudates or hypertrophy, presence of tender cervical glands, and absence of cough—were consecutively recruited. All patients underwent a pharyngotonsillar swab for microbiologic culture, which was sent to the Department of Microbiology, Joan XXIII University Hospital (Tarragona, Spain) in Amies medium (Copan Innovation, Brescia, Italy). Samples were seeded on a plate of blood agar and were incubated at 37°C in an 5% carbon dioxide atmosphere for 48 h. A culture was considered positive for GAS with a growth of any number of β-hemolytic colonies, gram-positive staining with streptococcal morphology, and a catalase negative test with posterior identification with an automated panel for gram-positive cocci using the Wider System (F. Soria Melguizo, Madrid, Spain). Results were confirmed with posterior serogrouping with the Streptococcal Grouping Kit (Thermo Scientific, Oxford, UK). The culture was considered negative with the absence of β-hemolytic colonies after 48 hours of incubation. Patients underwent a CRP rapid test during the consultation by means of QuikRead/Go devices (Orion Diagnostica, Espoo, Finland).
Results
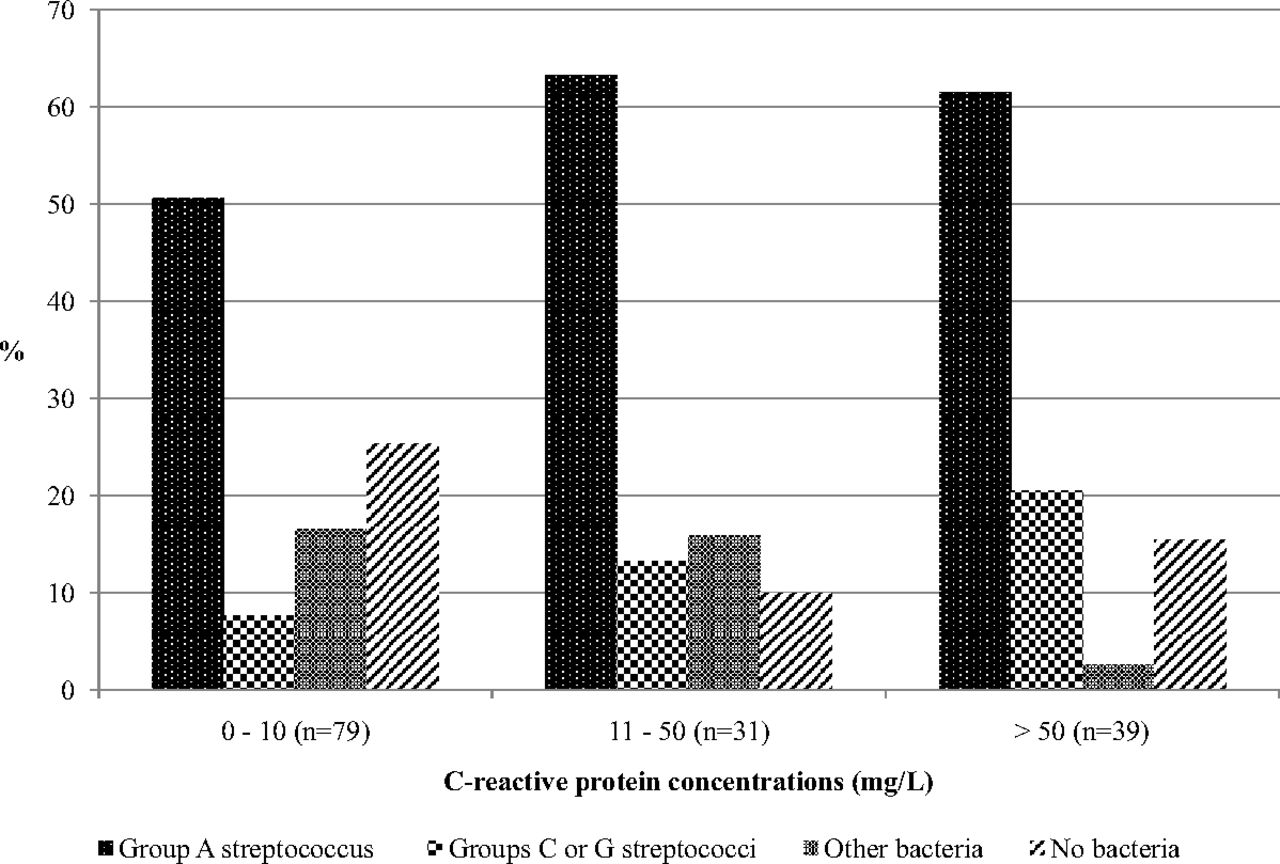
A total of 149 patients were enrolled. The most frequent etiology was GAS, present in 83 cases (55.7%). No bacteria were identified in 29 patients (19.5%). The age of the patients ranged from 18 to 51 years, with a mean of 28.5 years. GAS infection presented a higher CRP concentration compared with other etiologies (34.4 vs 29.9 mg/L, respectively), with no statistically significant differences (Table 1). The highest CRP concentration was observed among patients with group C streptococcus infection. Infection with groups C and G β-hemolytic streptococci was associated with slightly higher concentrations of CRP (49.9 mg/L) compared with those with infection by GAS, other causes, or no infection (Figure 1). The highest CRP concentration (182 mg/L) was observed in a patient presenting with a peritonsillar abscess and no bacterium identified during the consultation.
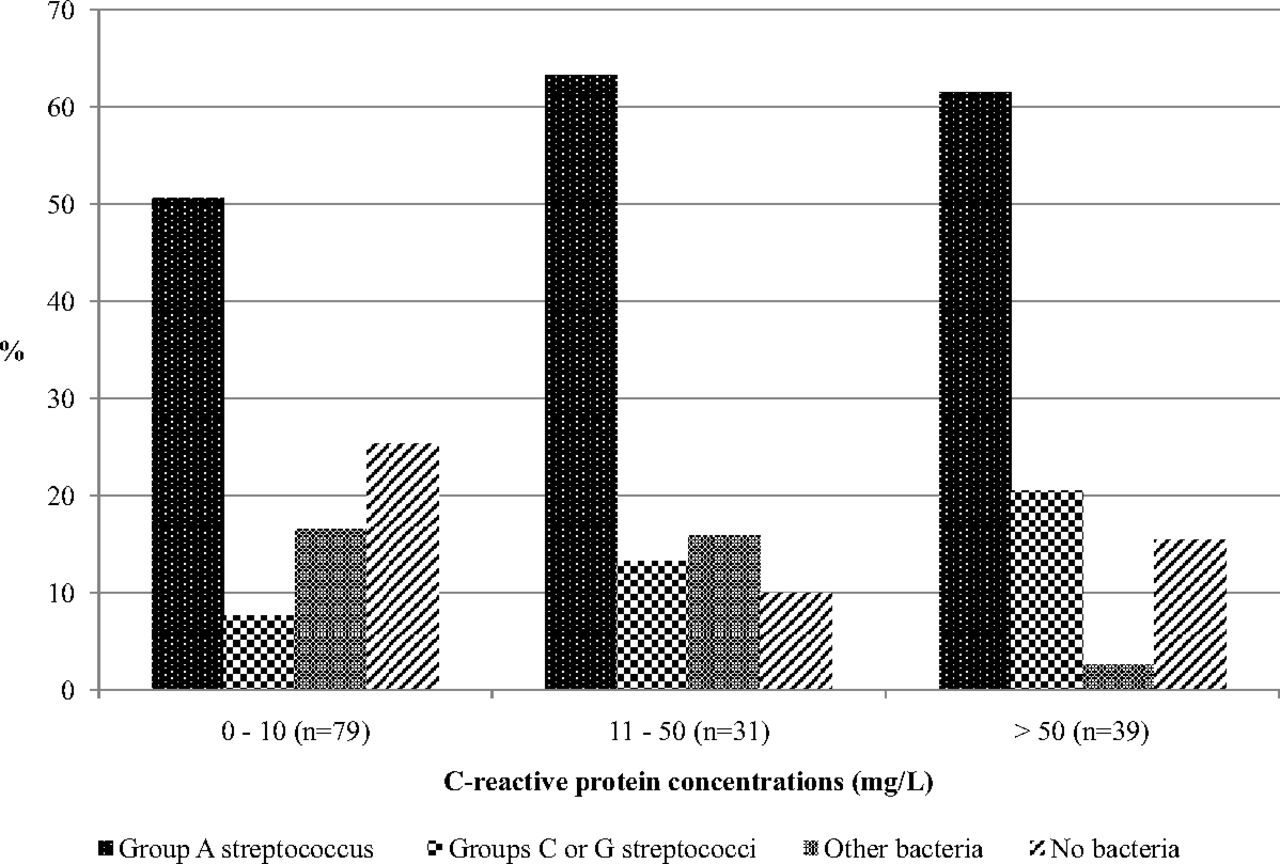
Association between C-reactive protein concentrations and the cause of infection among patients with sore throat and 4 Centor criteria.
Discussion
This study has several limitations. Only patients with the 4 Centor criteria were recruited, which explains why more than half of the patients actually had a GAS infection. Outcomes were not collected, nor was the evolution of symptoms measured, but we do not consider these limitations to be important since our goal was to identify the association of CRP concentrations with the etiology of the pharyngitis. The microbiologic study did not take into account the study of anaerobes, and some of the patients in whom no bacteria were identified may have been infected by these organisms. In our study the CRP rapid test used a finger prick blood sample; however, studies comparing these rapid tests with the routine CRP laboratory test have shown a very good correlation, thereby demonstrating its reliability.
Some studies have shown high CRP concentrations with GAS infection. Hjortdahl and Melbye7 observed a mean CRP concentration of 50.4 mg/L among patients with GAS infection, and Melbye et al8 observed an even higher mean value of 100.3 mg/L; however, they recruited only 11 patients with GAS. On the other hand, other studies have shown no relationship between CRP concentrations and GAS infection. In a Swedish study, the mean CRP value was 37.6 mg/L for the group with rapid antigen detection tests showing GAS and 37.4 mg/L for those with a test not showing GAS.9 Lindbæk et al10 observed mean CRP values of 43 mg/L, with the highest concentrations being found in infections caused by groups C and G streptococci, which is similar to our results.
Conclusion
Some studies suggest that CRP testing is overused.1,9 Our results show that CRP is not useful for differentiating GAS infection from other etiologies that do not require antibiotic therapy.
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: CL reports having a grant from the Fundació Jordi Gol i Gurina for a research stage at the University of Cardiff. He also reports receiving research grants from the European Commission (Sixth and Seventh Programme Frameworks), Catalan Society of Family Medicine, and Instituto de Salud Carlos III (Spanish Ministry of Health). The other authors have nothing to declare.
- Received for publication December 10, 2013.
- Revision received February 9, 2014.
- Accepted for publication February 11, 2014.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Prevalence of Group C Streptococcus and Fusobacterium Necrophorum in Patients With Sore Throat: A Meta-Analysis
- Out-of-hours antibiotic prescription after screening with C reactive protein: a randomised controlled study
- The Point-of-Care Laboratory in Clinical Microbiology
- Human Neutrophil Lipocalin as a Superior Diagnostic Means To Distinguish between Acute Bacterial and Viral Infections
- A Panoply of Information for the Practice of Family Medicine