
Abstract
This article describes eCHAT (electronic case-finding and help assessment tool), designed to improve health and well-being through systematic screening and intervention for modifiable lifestyle and mental health issues in primary care populations and monitoring to inform continuous quality improvement. eCHAT allows patients to identify unhealthy behaviors (risky substance use, gambling, being subject to abuse, physical inactivity) and negative mood states (depression, anxiety, anger) with which they would like help before a visit using an iPad in the waiting room or via the Internet in the community. Family physicians access summarized results, including scores and interpretations of screening tests at the point of care. eCHAT stimulates conversations between patients and clinicians about life changes they might make, encouraging active participation in decision making and engagement in self-management. Stepped-care clinical decision support tools offer interventions through self-management options to primary care interventions through to secondary care referral. As well as systematically screening and intervening in individual practice populations, anonymous collated and encrypted data also can be used to measure the mental health and lifestyle risk factors and interventions provided at practice network, regional, and national levels to monitor system and organizational performance improvements, identify regional and national variations, benchmark service delivery, and support quality improvement.
- Anxiety
- Decision Making
- Depression
- Mental Health
- Prevention
- Primary Health Care
- Screening
- Sedentary Lifestyle
- Substance Abuse
Improving Health and Well-Being of the Primary Care Population
Risky lifestyle behaviors and mental health issues impact health and well-being; hence early detection and intervention are likely to have substantial long-term health gains. Important risky behaviors that can influence health and well-being include misuse of tobacco, alcohol, recreational drugs, and gambling and physical inactivity. Mental health issues include anxiety, depression, difficulty controlling anger, and abuse, which refers to being hurt, threatened, or controlled by another person. Lifestyle issues, poor mental health, and chronic disease are all interrelated.1,2 People with comorbidities are more likely to be anxious, depressed, or both,3 and these relationships may be bidirectional.4
Addressing risky behaviors such as substance use and physical inactivity has the potential for primary and secondary prevention of chronic illness. Smoking cessation is one of the most important interventions for the prevention of chronic cardiovascular and respiratory diseases.5 However, family physicians have time constraints on systematically exploring these issues when patients present for other reasons. Furthermore patients may feel uneasy when asked about specific “bad” behaviors in isolation. A patient-centered approach is for patients to self-administer an instrument dealing with multiple domains through which they can identify unhealthy behaviors or problematic mood states and indicate which behaviors, if any, they would like the provider's help to address.
Our aim is to improve the health and well-being of the New Zealand population through systematic screening and intervention for modifiable lifestyle and mental health issues in the primary care population and monitoring to inform continuous quality improvement.
Electronic Case-Finding and Help Assessment Tool
For this purpose we have developed the Case-Finding and Help Assessment Tool (CHAT) to identify unhealthy behaviors (risky substance use, gambling, being subject to abuse, physical inactivity) and negative mood states (depression, anxiety, anger) in primary care and community settings, and we have conducted studies to establish that it is feasible for use in these settings.6,7 Previous studies have found high patient acceptability of the CHAT when assessed by 50 consecutive patients from 51 urban and rural practices (2543 patients), with <1% objecting to specific questions.8,9 Practitioners were also positive. When assessed against longer validated questionnaires, most of the screening questions in the CHAT had sensitivities of 81% to 96% and specificities of 74% to 97%.10,11 The drug use, abuse, and anger questions had lower sensitivity (45% to 80%) but higher specificities (87% to 97%). The physical inactivity question had lower sensitivity and specific because of the question format, which has been improved. A paper version of CHAT can be accessed at http://www.annfammed.org/cgi/data/7/3/239/DC1/1.10
Because almost all practices in New Zealand have had electronic medical records for at least a decade and do not refer to paper files, having a paper-based tool would not have been acceptable nor sufficiently useful for most family practices; it was always envisaged that the tool would be made available electronically. We therefore progressed to the electronic version, eCHAT, which allows for added diagnostic tools and integrated decision support.12 Patients who report use of tobacco, alcohol, or other drugs complete the Alcohol, Smoking, and Substance Involvement Screening Test, which is then scored and interpreted in the clinician's report.13 Similarly, patients who indicate issues with the depression or anxiety complete the 9-item Patient Health Questionnaire–Depression (PHQ-9)14 or 7-item Generalized Anxiety Disorder (GAD-7) Assessment,15 respectively. The eCHAT includes an innovative Help question that asks whether patients would like help with specific issues, either during the ensuing visit or at a later time, and whether they want to take any action to improve their mood or health behaviors. The Help question allows patients to prioritize their problems, prevents physician overload, and has been shown to significantly increase the specificity of the test.10,16,17 eCHAT facilitates the conversation between the patient and clinician about aspects of the patient's lives they consider important and wish to change, encouraging the patient to actively participate in decision making and engage in self-management.
After pilot trials,12 evaluation of the initial eCHAT deployment with 196 patients (91% patient response rate) found that domains for which patients wanted immediate help were anxiety (9%), depression (7%), physical activity (6%) and smoking (5%), which was not overwhelming for physicians.18 The majority found the iPad easy to use, the questions easy to understand and appropriate, and did not object to questions. Feedback obtained from interviews with 7 doctors, 2 practice managers, 4 nurses, and 5 receptionists was generally very positive, and the practices have continued to use eCHAT regularly since the research was completed.
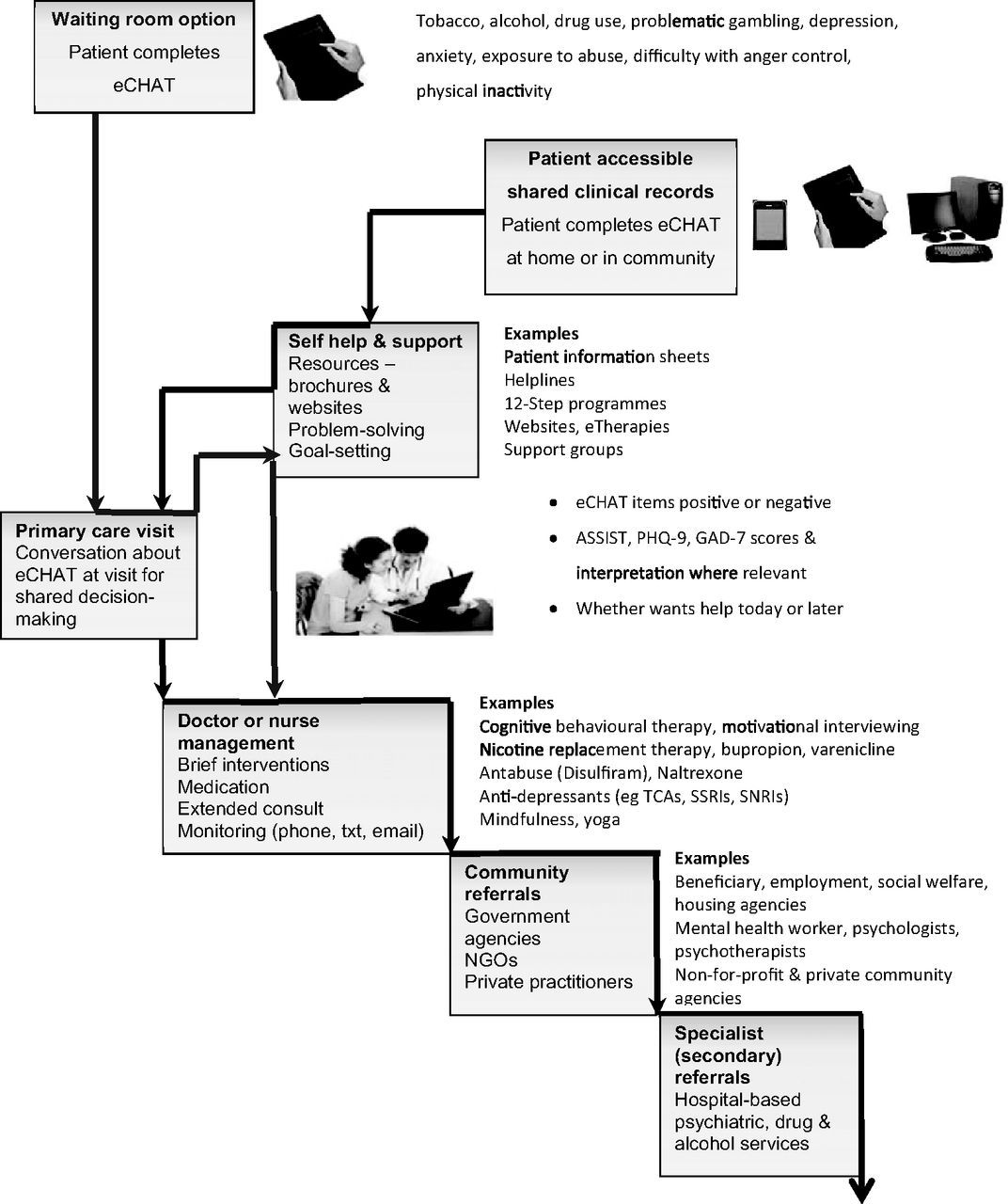
Patients self-administer the eCHAT on an iPad in the waiting room before the clinician visit (2 to 5 minutes), and the clinician receives an electronic summary report at the point of care, including scored and interpreted results and decision support tools, when indicated.12 Where there is the facility for patient access to their electronic medical record, they can be invited to complete eCHAT when they make an appointment electronically. A number of possible interventions can be accessed, using the stepped care model19 (Figure 1). Those in step 1 are self-management resources such as written information, help lines, and links to web sites, some of which include eTherapies. Those in step 2 are primary care clinician treatments including brief interventions and prescriptions. Step 3 includes community-based referrals, and step 4 includes referrals to secondary services. When patients complete eCHAT remotely (not in the waiting room), they can access self-help and support options directly and need to consult their clinician only when further intervention is required.

Case-finding and stepped care integrated decision support using eCHAT. ASSIST, Alcohol, Smoking And Substance Involvement Screening Test; GAD-7, 7-item Generalized Anxiety Disorder Assessment; NGO, nongovernmental organizations; PHQ-9, 9-item Patient Health Questionnaire–Depression; SNRI, serotonin and noradrenaline reuptake inhibitor; SSRI, selective serotonin reuptake inhibitor; TCA, tricyclic antidepressants.
The eCHAT differs from existing tools because it is a generic approach intended for all adults. It addresses both behaviors and mood states that impact health and well-being, with a focus on the whole person and not the disease. Because it is self-administered before a visit, it is efficient and reduces clinical staff time spent identifying unhealthy behaviors and negative mood states that are amenable to intervention. It builds on current theoretical models of behavioral change and is premised on the concepts of patient-centeredness, joint decision making, and self-management.20⇓⇓⇓–24
Primary care is the arena for improving population health. Starfield et al.25 made the case that family physicians have to be at the forefront of health care reform. They identified that primary health care needs to be accessible, person-focused over time, comprehensive, and coordinated.26 This is in line with the development of the patient-centered medical home (PCMH) and meets many of their specified criteria.27⇓–29
Because information is collected, analyzed automatically, and transferred seamlessly to the electronic medical record in real-time to be accessed by the clinician, it is an efficient and cost-effective way of assessing some of the major lifestyle health risks of patients. The time needed to case-find problematic lifestyle behaviors and mental health issues is reduced because eCHAT can be self-administered in the waiting room before the visit. Routine case-finding minimizes the chance of missing opportunities to provide early health care. eCHAT puts the patient in the center with a whole-person orientation not a disease focus. The questions on the eCHAT application greatly enhance the potential for clinicians to accurately identify patient needs around sensitive mental health issues such as depression, domestic violence, and use of alcohol or illicit drugs.
Primary care practitioners and practices may choose to screen all adult patients (aged ≥16 years) routinely or may elect to target screening using criteria such as all new patients, those who have not presented for 2 years, and those meeting certain conditions such as pregnancy, chronic illness, or previously identified increased risk of mental health or lifestyle concerns. eCHAT can be used as a repeated measure to track individual patients' progress over time. The practice can also electronically audit the proportion of patients answering positive to each eCHAT domain, those who want help and interventions delivered. These data can inform further development of interventions including provision of group therapies.
Measuring Need and Response
eCHAT technology supports best patient care, education, and communication and facilitates performance measurement. It is an evidence-based initiative10,11 that has the potential for the addition of a number of clinical decision-support tools to guide decision making, allows for rapid assessment of patient needs, prompts the patient to develop a proactive plan of care, facilitates communication between patients and providers, provides pathways to connect the patient with community resources, and combines a systems-level approach to assess the needs of populations with individual patient care. It facilitates coordinated and integrated care across community providers, which enhances the value of health care (core value-driving elements of the PCMH).
As well as systematically screening and intervening in individual practice populations, anonymous, collated, and encrypted data also can be used to measure the mental health and lifestyle risk factors and interventions provided at practice network, regional, and national levels. New Zealand practices belong to networks, primary health organizations (PHOs) designed to designed to fund and deliver primary health care services to the community in line with the primary health care strategy.30 All patients registered with a practice are on the practice's PHO register. PHOs are tasked with providing access to comprehensive services to improve, maintain, and restore people's health; coordinating care across service areas; and continuously improving quality using good information.30 As part of this, practices are required to collect quality of care performance indicators, such as smoking status and smoking cessation interventions. The eCHAT assists with this sort of compliance requirement by automatically collecting this data electronically, as well as allowing other audits of mental health or risk factor detection and appropriate intervention.
Work is currently progressing to store summary statistics of eCHAT results (made anonymous) in a data warehouse for service-level monitoring to provide an overall picture of progress in working with mental health and addictions. This monitoring is aimed at measuring system and organizational performance improvements, understanding regional and national variations, providing a basis for benchmarking of service delivery, and supporting continuous quality improvement.31
A rollout to 30 practices throughout New Zealand is now underway, with integrated stepped care decision supports (options for self-management, health provider interventions, community-based referrals and secondary care) for all 9 of the eCHAT domains. We are conducting a quantitative analysis of positive eCHAT responses, requests for help, and interventions initiated as well as quantitative (survey) and qualitative (interviews) study of feedback from all practice staff (doctors, nurses, receptionists, practice managers). A clustered RCT is planned to look at effects of eCHAT or no eCHAT on patient outcomes at the practice level.
Use in Community Settings Other Than the PCMH
eCHAT is beginning to be used in community settings beyond the PCMH. Outside of New Zealand, eCHAT is being deployed in a Cook Inlet Tribal Council community setting for Inuit youth in Alaska. In New Zealand it is being trialed in a decile 1 (low socioeconomic) high school, with students completing eCHAT on their school netbooks and results being responded to by the school nurse. Should evaluation be positive it could be introduced into all high schools with an attached health clinic (deciles 1 to 3). It also is being introduced into student health centers in a number of New Zealand tertiary institutions (universities).
Conclusions
The eCHAT program is an example of systematically identifying and managing mental health and lifestyle issues in primary care practice settings in partnership with primary care organizations, allowing for integration of services across the health sector at the local and regional levels. Early detection and intervention of modifiable risky behaviors and mood issues should have positive effects on the mental and physical well-being of the population.
Acknowledgments
The development of the eCHAT over the past decade has involved many coauthors and collaborators and other contributors too numerous to name.
Notes
This article was externally peer reviewed.
Funding: Funding for various aspects of this work was provided by the Oakley Mental Health Foundation, the Health Research Council, the Charitable Trust of the Auckland Faculty of the Royal New Zealand College of General Practitioners, the Research and Education Charitable Trust of the Royal New Zealand College of General Practitioners, the Ministry of Health Mental Health Directorate, the Institute of Rural Health, Hamilton and The University of Auckland Faculty Research Development Fund.
Conflict of interest: none declared.
- Received for publication August 26, 2012.
- Revision received November 2, 2012.
- Accepted for publication November 27, 2012.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Use of codesign in primary care research: real-life examples
- Factors influencing recording of drug misuse in primary care: a qualitative study of GPs in England
- Screening for lifestyle and mental health risk factors in the waiting room: Feasibility study of the Case-finding Health Assessment Tool
- Successful Behavioral Interventions, International Comparisons, and a Wonderful Variety of Topics for Clinical Practice