
Abstract
The US Preventive Services Task Force has emphasized individualized decision-making regarding participation in screening mammography for women ages 40 to 49. Positive public opinion regarding screening mammography is understandable given that screening advocates have heavily promoted the slogan “early detection saves lives” while ignoring screening harms. The goal of mammography screening advocates is to increase screening participation or uptake. The purpose of this paper is to promote physician and patient insight by presenting the age-related benefit and harms of screening. At age 50, routine screening saves approximately 1 woman per 1000 over 10 years. The life-saving proportion of screen-detected cancers is 5%, which means mammograms must detect 21 cancers to save one life. Almost half of screen-detected cancers represent pseudo-disease and would never become symptomatic yet alone lethal during a woman's lifetime. Consequently, 40- and 50-year-old women are 10 times more likely to experience overdiagnosis and overtreatment than to have their lives saved. Analysis of events and outcomes per single screening round for women ages 40 to 49 show that approximately 9600 screening mammograms, 960 diagnostic exams, and 90 to 140 biopsies are required to save one life. Given the substantial harms of screening, advocates should refocus their priority from promoting uptake to promoting insight.
Judging by recent media coverage, many of the 2.5 million breast cancer survivors in the United States, including 610,000 women with ductal carcinoma in situ (DCIS),1 were outraged at the US Preventive Services Task Force for not continuing to advise routine screening mammography for women ages 40 to 49.2 Based on an update of the evidence regarding the benefits and harms of screening, which was published in November 2009,3 the Task Force is re-emphasizing individualized decision making for these women. The belief that earlier detection of breast cancer almost always is beneficial explains part of the negative public reaction to this recommendation.4–6 Assuming the truth of this premise, a woman with a screen-detected cancer has a valid and sound argument that “mammography saved my life.”7 Consequently, every breast cancer survivor and her friends and family have a reason to become screening mammography advocates. For instance, the founder of the Susan G. Komen Foundation claims that she is “one woman whose life was saved by early detection.”8
Public opinion regarding screening mammography is understandable given that the concept “earlier detection saves lives” has been heavily promoted but not clearly explained by mammography supporters including physician organizations,9 the American Cancer Society,10 and advocacy groups.11 However, the premise of a near universal life-saving benefit from finding presymptomatic breast cancer through mammography is false. The following is a quick analysis of the “life-saving proportion” of screen-detected cancer. Women often die of breast cancer after screening; mammography achieves approximately a 1 in 5 life-saving benefit (the relative mortality risk reduction) in the subgroup of women who have lethal breast cancers. If all screen-detected breast cancers were rapidly lethal, the highest life-saving proportion would be 20%. In the United States, the diagnostic risk for breast cancer (screen-detected or not) is approximately 6 to 7 times the death risk over 15 years. Risk means an outcome for 1000 people at risk for an event over a period of time.12 Therefore, the lowest life-saving proportion would be 3% (1/5 × 1/7) in the larger subgroup of women who have been diagnosed with cancer.13
The “pink ribbon” marketing10,14 of breast cancer awareness supports advocacy groups and aims to increase the uptake of (participation in) mammography. Ostensibly for the sake of public health, the advertising campaign has some negative consequences.15 One side effect is distorted physician and public insight about the age-related benefit and the substantial harms of screening. For instance, in one survey more than half of US women thought that mammography helps to prevent or reduce the risk of contracting breast cancer.16 Gigerenzer et al17 reported that less than 2% of European women have insight into the absolute benefit of routine screening mammography, and most women overestimate the benefit by orders of magnitude. The absolute benefit derived from an overview of Swedish randomized screening trials is one breast cancer death averted (or one life saved) in the invited group versus the control group per 1000 women after 10 years.18
The US Preventive Services Task Force deserves praise for promoting insight among younger women by stressing the well-known downstream screening harms that can result from false-positive mammograms. These radiologist interpretations produce anxiety beyond the initial screen and require additional evaluations including diagnostic mammograms, ultrasounds, and biopsies that do not find a cancer. Any breast radiologist who has contact with patients sees this anxiety every day while performing diagnostic evaluations. However, the US Preventive Services Task Force has downplayed the major harm of screening. Overdiagnosis of breast cancer is the preclinical detection of either stable disease, such as forms of DCIS, or indolent or slow-growing tumors in older women. This pseudo-disease would never become symptomatic (and diagnosed) let alone metastatic (and lethal) during a woman's lifetime without screening. Because physicians must treat all true-positive or histologically confirmed mammograms as potentially lethal cancer, women with pseudo-disease can only be harmed by screening mammography.19
In theory, earlier detection of localized cancer through screening mammography should result in a compensatory drop in future advanced cancer and cancer deaths, yet this has not occurred.20,21 Nevertheless, prominent breast radiologists continue to deny a significant problem with overdiagnosis,22 and the 2010 American Cancer Society guidelines do not mention overdiagnosis as a limitation of mammography.23 The problem of overdiagnosis is not publicized during screening invitations24,25 and most women are not aware of nonprogressive cancer.5 The 2009 analysis of the screening trials by the Cochrane Database of Systemic Reviews calculated a 30% overdiagnosis rate (excess cancers and surgeries compared with control), or 0.3 ÷ 1.3 = 23% of all cancers in screened groups.26 Recent articles by Jorgensen and Gotzsche27 and Jorgensen et al28 include an overdiagnosis estimate for invasive cancer of 35% (52% including DCIS) in countries that have organized screening programs (34% of all cancers in screened populations, screen-detected or not),27 and 33% in a country that has organized screening and a control group.28 Morrell et al29 estimated overdiagnosis in an organized program of between 30% and 42% for invasive cancer only. The US Preventive Services Task Force's estimate is between 1% and 10%.3
Sackett30 warned that history shows preventive medicine “experts” can be assertive, presumptuous, and overbearing. In today's mammography debate, some screening advocates claim to support individual decision making yet tell women what to do, confident that screening benefits outweigh the harms,31,32 while attacking those who question their promotion of screening.33,34 Physicians who support insight should be indifferent to uptake.6,35 Given the reaction of specialists who have professional and financial interests in screening, primary care physicians will have to implement the US Preventive Services Task Force's recommendations. In support of this goal, Table 1 summarizes the epidemiology of breast cancer. For perspective on the opportunity cost of the resources devoted to screening mammography, columns A and B show the 10-year, all-cause death risks for smoking and nonsmoking US women at ages 40, 50, and 60.36 In comparison, columns C and D show the diagnosis risk for breast cancer and DCIS,37 whereas column E shows the absolute death risk without screening mammography.13 Barratt et al38 show similar estimates for Australia. Without screening, over a decade a 50-year-old woman has a 5 times greater risk of receiving a diagnosis of breast cancer than of dying from it. She also has a 10 times greater risk of dying from something besides breast cancer.
Death and Diagnosis Risks Per 1000 Women in the United States over 10 Years
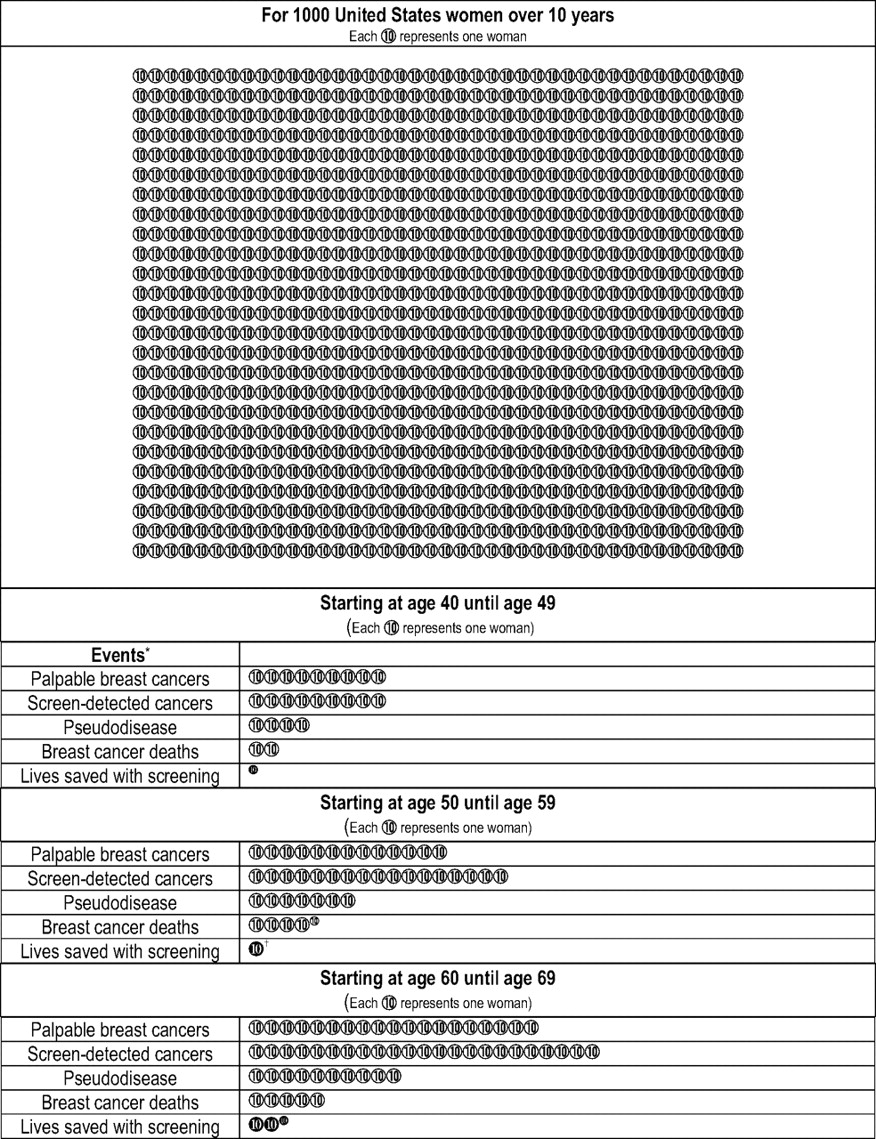
Table 2 derives estimates for the life-saving proportion of screen-detected cancers, the reciprocal or number needed to detect to save one life,13 and the extent of overdiagnosis for US women.39–41 Column F shows lives saved, or the absolute risk reduction from an invitation to routine screening. The absolute risk reduction is simply the relative risk reduction multiplied by the absolute death risk (column E). The reciprocal, or number needed to invite for repeated screening over a decade, are 2500, 1300, and 400. Ignoring volunteer bias and adjusting for compliance,38 at age 50 routine screening saves approximately one woman per 1000 over 10 years. The participation rate for US women and the uptake in the most recent screening mammography trial are 70%.3,42 Column G, or screen-detected cancer among all diagnosed cancer (column C in Table 1) depends on the sensitivity of mammography43 and screening participation. Mathis et al44 found that 57% of breast cancer was screen-detected. Likewise, column H, or pseudo-disease estimates, depend on an overdiagnosis rate applied to all diagnosed cancer, screen-detected or not. At age 50 almost half (42%; range, 9% to 62%) of all screen-detected cancers represent overdiagnosis of pseudo-disease. The only available estimate from the screening trials is 24%.19 Figure 1 presents relevant information in a patient-friendly format.

Estimated Breast Cancer Events Per 1000 Women in the United States over 10 Years
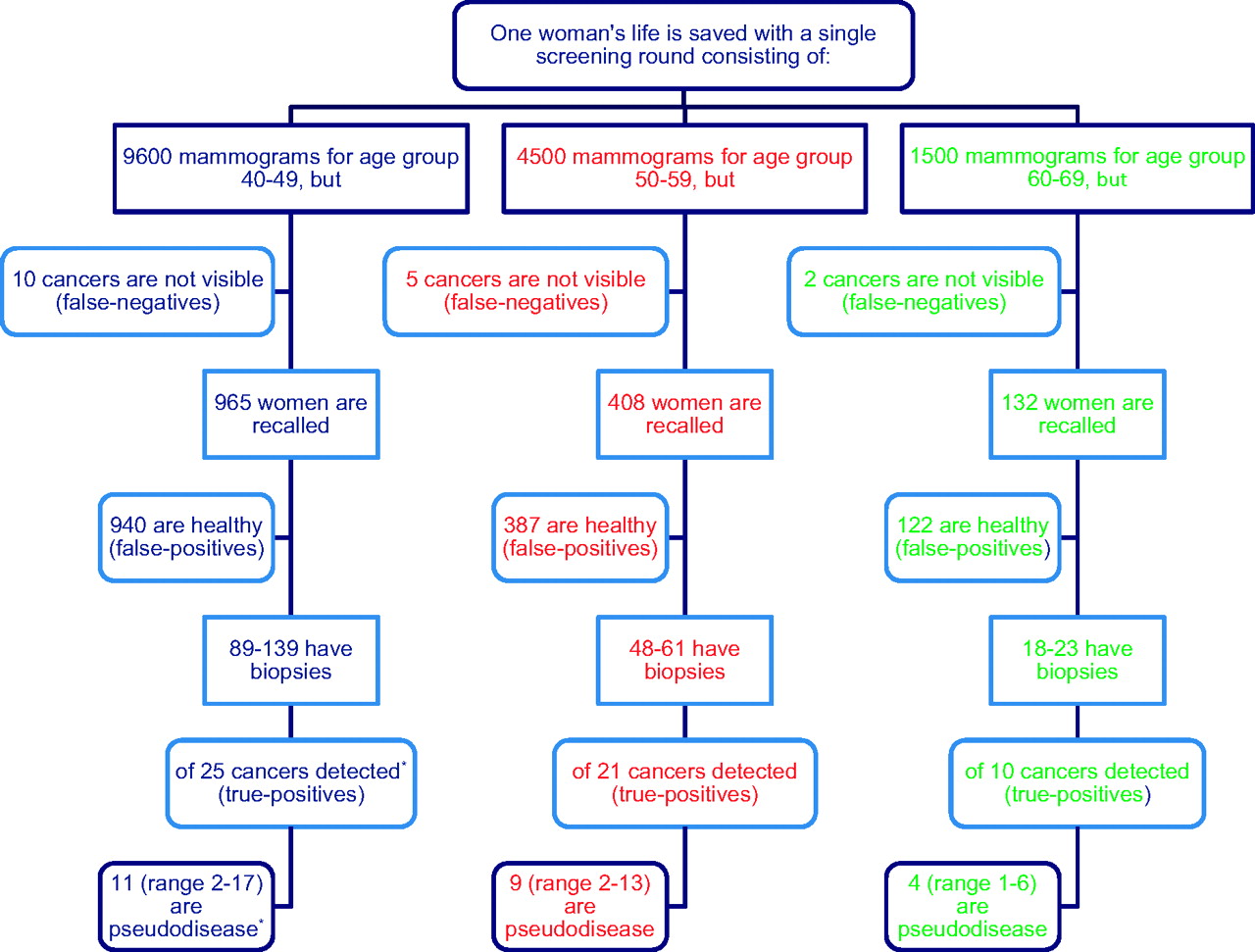
For women at age 50, the benefit “1/1000 over 10” reframed means that through routine screening a woman can increase her breast cancer survival from 99.5% to 99.6%, and her overall survival as a nonsmoker from 96.3% to 96.4% over a decade. Table 2 from the US Preventive Services Task Force update3 provides downstream average outcomes for a single screening round for different age groups. By applying the number needed to detect to save one life, the flowchart in Figure 2 shows estimated events and outcomes per screening round, including false-negative and false-positive mammograms and biopsies needed to save one life. The overdiagnosis ratio at the bottom means that, for women aged 40 to 59, approximately 10 women receive unnecessary mastectomies or lumpectomies and possibly chemotherapy and radiation treatment for every life saved.26

Estimated single-round screening mammography events and outcomes necessary to save one life by age group. Age-specific events and outcomes per screening round per cancer detected are Breast Cancer Surveillance Consortium data from Ref. 3. *The number needed to detect multiplier and overdiagnosis ratio are derived in Table 2.
Figures 3A and B provide additional information for patients. Nekhlyudov and Braddock45 present a model patient-physician dialogue for young women, whereas Gotzsche et al46 have written a screening mammography information leaflet.
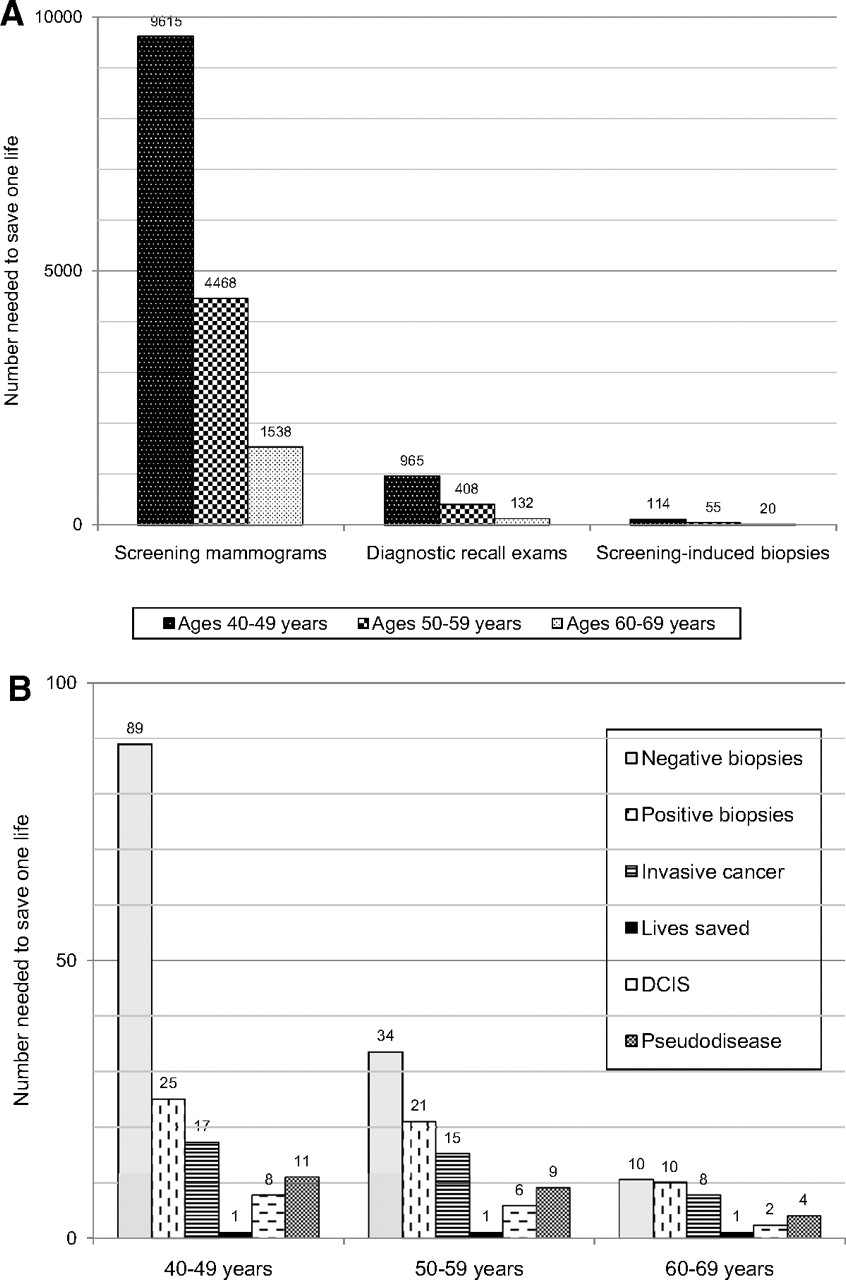
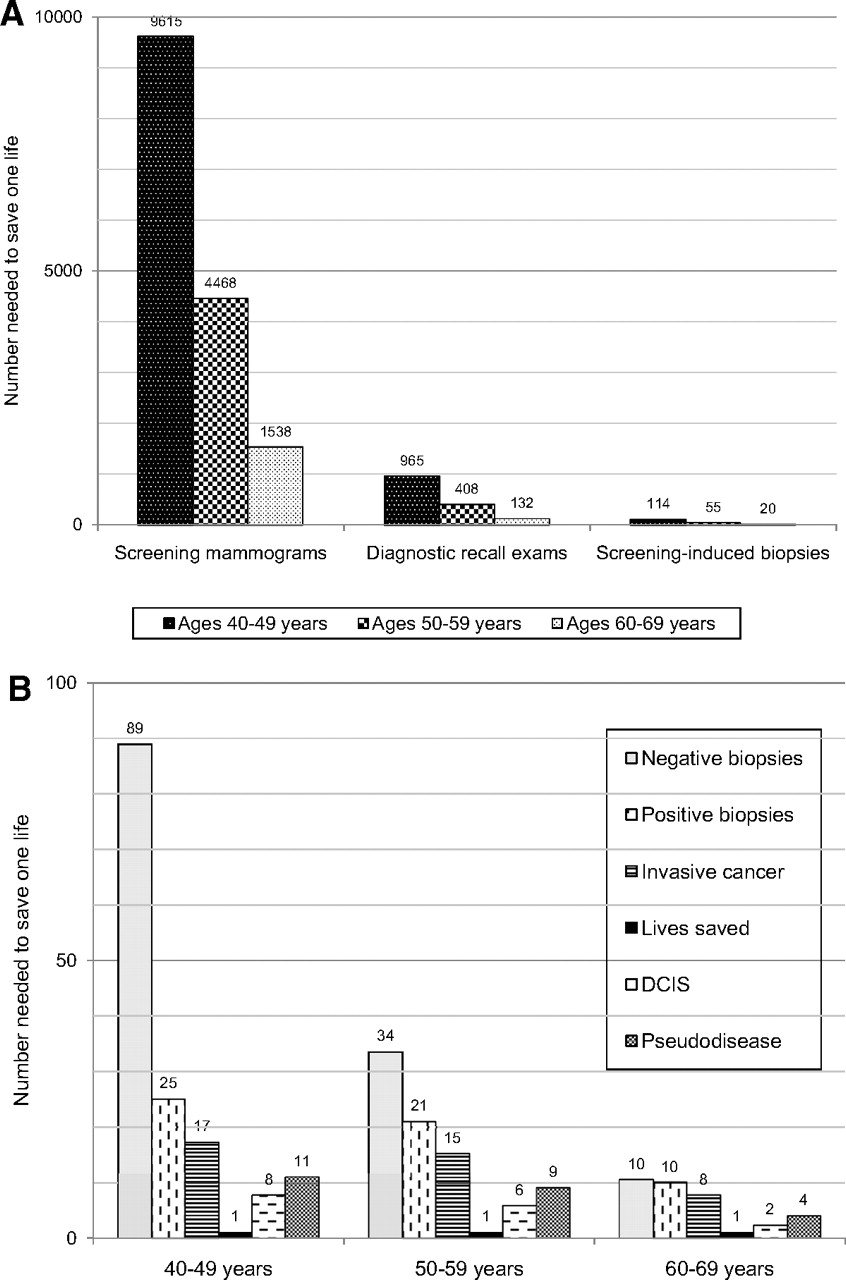
A: Estimated single-round screening mammograms and follow-up diagnostic events necessary to save one life stratified by age. Age-specific events and outcomes per screening round per cancer detected are Breast Cancer Surveillance Consortium data from Ref. 3. B: Augmented view of estimated screening-induced biopsy outcomes necessary to save one life by age group. DCIS, ductal carcinoma in situ.
Conclusion
The limited age-related benefit from screening mammography means that, for younger breast cancer survivors, mammography most likely (>95%) did not save their lives. Forty- and 50-year-old women thinking about participating in screening are 10 times more likely to experience overdiagnosis and overtreatment than to have their lives saved by mammography. Given this reality, screening advocates should refocus their priority from promoting uptake to promoting insight. Primary care physicians have an obligation to understand the harms and benefits of screening to help empower their patients to make individual decisions. If younger women decline screening participation because of increased understanding about benefits and harms, all physicians should appreciate this decision as a reasonable choice.
Acknowledgments
The author wishes to thank James E. Keen for manuscript review and the peer reviewers for their helpful comments.
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: none declared.
- Received for publication March 16, 2010.
- Revision received July 6, 2010.
- Accepted for publication July 28, 2010.




{kind=link}
{kind=link}
{kind=link}