
Abstract
The growing number of lower-extremity abnormalities that are seen in inpatient and outpatient settings has paralleled the increased number of elderly in the population. Foot and ankle deformities, disorders, and arthritis, which are not manifested until late in life, have become more common as more individuals attain longer lifespans. Although conservative therapies are a priority when addressing the geriatric population, surgical options may be overlooked secondary to a misunderstanding of their ability to overcome perioperative management. Advanced minimally invasive surgical procedures for the foot and ankle have decreased the complications associated with foot surgery, making surgical intervention a viable option for many of the elderly. The newer procedures do not, however, minimize strict perioperative management, including pharmacological and nutritional assessment, and cardiopulmonary precautions. Outpatient surgical intervention may effectively address many ongoing problems associated with pain, decreased ambulation, and decreased quality of life. Current techniques in joint reconstruction in the forefoot and midfoot allow weight bearing from the day of surgery. Most hindfoot and ankle surgeries now permit minimal bone resection and incision through arthroscopy, resulting in improved muscle and tendon repair and early weight bearing. The changes in surgical approaches for the geriatric foot have permitted more effective and rapid intervention in problems affecting ambulation and quality of life in our aged population.
Patients over the age of 65 are the fastest growing segment of the population; this population numbers more than 30 million people (>12.5% of the population).1–3 Increased life spans have been promoted by advances in medicine, science, and healthy lifestyles. Promotion of physical activity and ongoing exercise among the elderly has resulted in these individuals being stronger and healthier than previous generations. Increased activity and increased lifespan both contribute to the development of extensive lower extremity problems, including degeneration of bone and joints. Ligaments, tendons, and muscles are more easily damaged or injured, and the lower extremity, foot, and ankle have been specially affected.4 Once injuries or physical changes occur and impact quality of life, the question arises as to whether a conservative versus a surgical approach is in the patient's best interest. Numerous factors—including but not limited to medical history, physical and mental condition, and ambulatory status—must be considered because age alone is not a direct contraindication for surgical correction of foot and ankle deformities.
Advances in medicine and surgery are providing more low-risk and sophisticated treatment options that have not been previously available. Latest advances in surgical techniques and a better understanding of biomechanics have allowed us to perform surgery in the geriatric patient with functional results equivalent to those found among younger patients.5,6 Figure 1 illustrates successful surgical results of a boney deformity attributed to progressive arthritic changes in the foot. In the absence of any significant contraindications, a forefoot correctional procedure was performed, which decreased patient pain and allowed for improved quality of life.
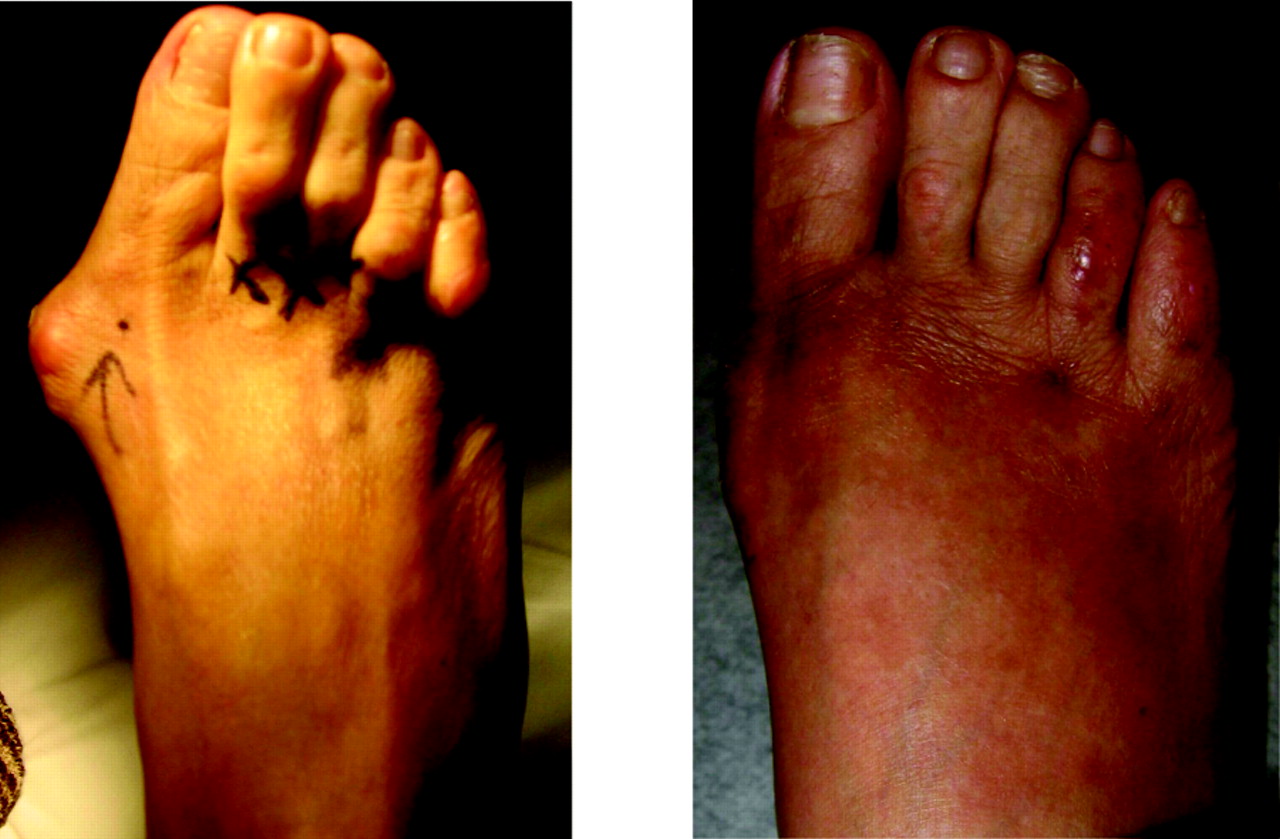
Forefoot arthritis. Preoperative (A) and postoperative (B) clinical views after first metatarsophalangeal joint and digital reconstruction.
Surgery in the geriatric patient had been avoided because it was associated with high morbidity and mortality rates related to surgical procedures and general anesthesia. Currently more than 20% of all surgical admissions in the United States are geriatric patients.7–9 The recent medical literature suggests that there were neither increased complications or deaths with the use of general and local anesthesia in the geriatric patient compared with previously known data.8,10,11 The medical literature suggests that the severity of the disease or illness is a better indicator or predictor of surgical and anesthesia outcome versus the patient's chronological age.12,13 The following is a review of considerations that may assist with referral of the geriatric patient for possible lower extremity surgery.
Surgical Considerations
Nutrition
Foot and ankle deformities, disorders, and arthritis may remain asymptomatic for years before becoming fixed, rigid, and painful among the aged population.11 They are common in the geriatric patient and may lead to loss of lower extremity mobility and function, which in turn may contribute to deterioration of the cardiovascular system, a rapid decline in health, and a reduced life span. The musculoskeletal system undergoes significant change during the aging process as osteoarthritis and osteoporosis develop and progress, especially in women after menopause. Bone loses rigidity and strength and becomes more brittle. Joints and surrounding soft tissue become weak and less flexible with aging.14,15 It is important to consider pharmacological and nutritional management pre- and postoperatively to enhance bone quality and healing.16–19 Maintaining adequate protein levels as well as appropriate dietary supplementation may assist the healing process in patients considered nutritionally compromised. Patient's protein levels need to be assessed, along with a review of the patient's dietary habits. Special considerations need to be given to obese patients because obesity may be an indicator of poor nutritional status. Obesity also places excessive stress on the lower extremity and may contribute to poor healing and surgical outcomes. Laboratory tests recommended for determining to nutritional status include patient's body mass index (BMI; weight in kilograms/height in meters [BMI < 17 kg/m2 is associated with protein–energy undernutrition]); serum albumin (<3.5 mg/dL is a simple indicator of possible malnutrition); serum levels of vitamins A, B1, B12, C, D, E, iron, folic acid, zinc, and magnesium; serum creatinine levels; total urine nitrogen; complete blood count; comprehensive metabolic panel; liver function test; and lipid panel.
Preoperative Medical History
Preexisting medical conditions are of as much concern as nutritional status. Medications affecting cellular function and fibroblast activity are known to delay the closure process. It is not uncommon for elderly patients to be taking high levels of nonsteroidal - medications or possibly even steroidal medications for indications, including various arthritic or vasculitic conditions. A history of a previous deep venous thrombosis is important to determine because the risk of a postoperative deep venous thrombosis is increased if the patient has had one previously. Age, sedentary lifestyle, history of previous lower extremity trauma, hypercoagulability, and even family history of deep venous thrombosis are reasons for anticoagulant prophylaxis. Prophylaxis is a further consideration for patients who are expected to remain in bed for >48 hours or whose ambulation will be limited after discharge. Patients with a short hospital stay (<48 hours) and immediate ambulation still require the use of a compression device during the admission period to decrease risk of clot formation. There have been studies to evaluate these guidelines, but the incidence of venous thromboembolism after foot and ankle surgery has been rare (<1%) and the need for routine propylaxis postoperatively is not supported by any high level of evidence studies.20–22
Preoperative Examination
Planning for surgery in the geriatric patient involves all the requirements and criteria of the adult patient with special emphasis on preoperative cardiopulmonary precautions, appropriate surgical procedure selection, and proper postoperative management to maximize bone healing.23 The surgeon should consider obtaining medical clearance for the planned procedure from the patient's primary care physician and cardiologist.
Indications of surgery in the medically cleared patient include the failure of previously attempted conservative management and pain, deformity, and/or functional disability that significantly impairs quality of life. When conservative management provides satisfactory results, surgery should not be encouraged. Postoperative compliance and a suitable postoperative living environment are additional preoperative considerations. Selected patients may require postoperative home care and physical therapy or short-term placement in a rehabilitative or skilled nursing facility. Preoperative considerations include the ability of the planned procedure to address pain, correct deformities, and to restore function, allowing patients to resume their activities of daily living and improve their quality of life.
Preoperatively, patients will require clinical, biomechanical, radiographic, social, and psychological evaluation and preparation. It is imperative to have a thorough discussion of the diagnosis, surgical treatment options, and prognosis with the patient and family involved. Patients may have unrealistic expectations about surgical procedures and may make the assumption that a normal “youthful” lower extremity will result from the intervention. Advantages and disadvantages of the procedure, expected levels of function and pain, level of postoperative care, and anticipated affect on ambulation require clear explanations and realistic expectations before obtaining a signature on an informed consent. Conservative options should have been tried and failed before surgical intervention.
Before scheduling procedures, it is imperative to obtain a medical clearance from the patient's geriatric physician. This is recommended to ascertain the cardiovascular and pulmonary status and risks of perioperative myocardial events, even among healthy geriatric patients.12,24–27 Cardiovascular and pulmonary status are directly related to the rates of morbidity and mortality, and they can pose greater risks and complication when they are not managed properly.7,28–30 Functional assessments using activities of daily living scales can predict perioperative rehabilitation requirements based on observations of their functions and multiple customary activity assessment.31–33 The American Society of Anesthesiologists criteria are also useful guides in the surgical risk assessment and perioperative management of the geriatric patient.8,11,34 When there is doubt concerning the patient's ability to tolerate a procedure, it is wise to choose the conservative option.
Postoperative Considerations
The majority of foot and ankle surgery is performed in an outpatient setting. However, this should not minimize strict perioperative management. Emphasis on mobility and function and aggressive rehabilitation for deep venous thrombosis prophylaxis is important.22,35–37 Time for foot and ankle surgery rehabilitation has previously been documented as 1½ to 2 times that of a young patient, with precautions for a short-leg non-weight-bearing cast, contralateral limb injury, and/or potential for over use and falling.11 With the advent of advanced surgical techniques and ambulatory devices, these practices are changing. Early ambulation is recommended to decrease adverse effects of anesthesia after surgery while minimizing the risks of cardiopulmonary complications commonly associated with surgery and anesthesia. Pain management may be accomplished with regional blocks and continuous local infusion systems, which have eliminated or minimized the intake of postoperative pain medications and narcotics.12,13 Consideration of all the factors previously discussed allow for selection of the appropriate postoperative setting to assist with rapid recovery and a return to the patient's previous lifestyle.
Surgical Options for Eligible Candidates
Simple surgical procedures with local anesthesia may provide dramatic relief, permitting normal ambulation and resumption of daily activities while prolonging the length and quality of life. Selection of the most appropriate surgical procedure is paramount to the successful outcome of the surgery. Selection of the specific surgical procedure is based on the patient's health, the location of the problem, the level of severity/deformity, the need for single or multiple staged procedures, the length of rehabilitation, and postoperative course. New advanced procedures allow early weight-bearing and minimal to no use of any non-weight-bearing casts.22 It is not our purpose to describe here the detailed surgical technique of the procedures that will be mentioned; however, a definition of the more common procedures described is given in Table 1.
Common Foot and Ankle Surgical Terms
Osteoarthritis and boney deformity are frequent findings in the forefoot and midfoot of the elderly.38 The etiology can be multifactorial and include muscle imbalance, flat footedness, and trauma. Severity of deformities may be more pronounced with rheumatoid arthritis and other systemic arthritic conditions. Patients typically complain of pain and disability causing difficulty in ambulation, primarily with forefoot loading and propulsion phases of gait, as well as pain with shoe wear at the forefoot or distally from the midfoot. Corns and callouses are findings that may reflect an underlying osseous deformity.
Forefoot Procedures
The most common forefoot deforming arthritic conditions include hammertoes, hallux valgus (“medial bunion”), hallux rigidus (“dorsal bunion”), metatarsophalangeal joint derangement, metatarsalgia, first ray hypermobility and instability, tailor's bunion (fifth metatarsal bunion), and posttraumatic arthritis and deformity (Lisfranc injury, fractures of the phalanx, metatarsal, cuneiforms, cuboid, navicular, and Charcot foot). Figures 2, 3, and 4 These deformities are primarily addressed with less complicated osteotomies and minor bone excision.

Hallux valgus. Note the severe contractures and deviations in the forefoot.

Tailor's bunionette. Note the angular osseous malalignment of the 5th metatarsal.

Diabetic Charcot deformity. Note the osseous destruction and collapse in the midfoot preoperatively (A) and the postoperative view of the reconstruction (B).
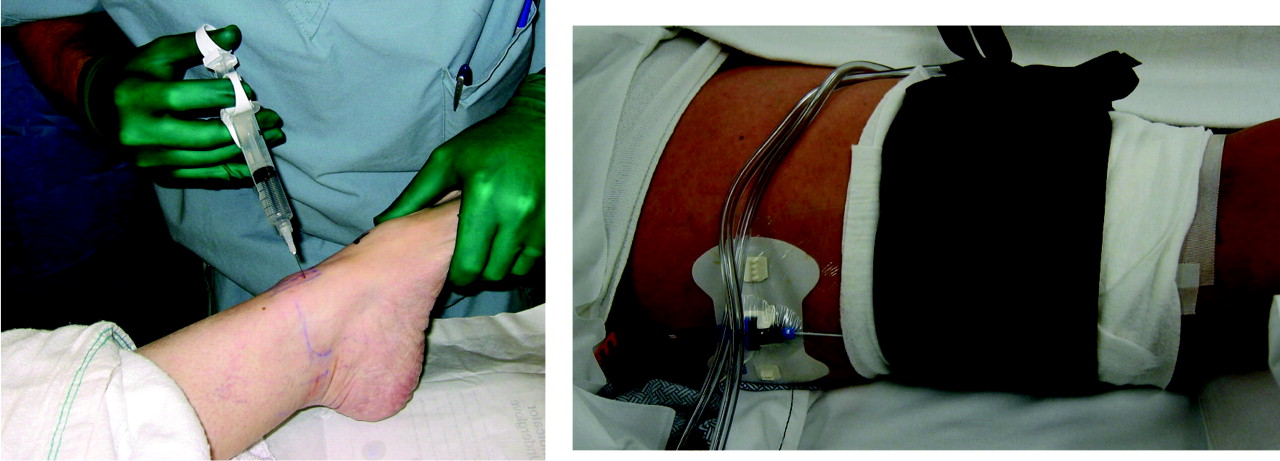
These procedures are usually performed under intravenous sedation (monitored anesthesia care) with regional local blocks (marcaine/lidocaine) in an outpatient setting39,40 (Figure 5). Most patients are treated with a postoperative weight-bearing shoe or a temporary non-weight-bearing splint, which is eventually switched to a walking boot. Patients with gait instability may prefer a walker or Roll-A-Bout device (Roll-A-Bout Corporation, Frederica, DE; Figure 6) because they provide 3-point walking stability over the traditional cane or crutches.

Regional blocks: (A) ankle and (B) popliteal.

Non-weight bearing assistance devices as alternatives to traditional crutches and walkers.
Digital procedures including arthroplasties or arthrodeses correct multiplanar deformities of the proximal and distal interphalangeal joints. These corrections allow proper alignment of digits and the removal of painful joint surfaces for ease of shoe wear and prevention of arthritic ulcerations.
Midfoot Procedures
Procedures at the first metatarsophalangeal joints are divided into cheilectomy, osteotomy, implant arthroplasty, and arthrodesis.41 They are either joint-sparing or joint-replacing procedures. Joint-sparing procedures (cheilectomy, osteotomy) have an excellent outcome in the presence of end-stage arthritis. Increased deformities have had better outcomes with joint-replacing procedures (implant arthroplasty and arthrodesis). Metatarsophalangeal joint resections and Keller-type procedures are usually reserved for end-stage conditions in which ambulation and flexibility are not a concern. Instability and posttraumatic arthritis in the tarsometatarsal joints require bone resection, which is the simplest approach, or arthrodesis to eliminate the source of pain and provide stability. Although bone resection does not require the use of fixation devices, arthrodesis requires joint preparation and fixation. These particular joints are not essential for gait. Their range of motion is minimal compared with the essential joints of the ankle, subtalar, midtarsal, and first metatarsophalangeal joints.
The fusion of tarsometatarsal joints provides significant pain relief and stability to the midfoot in stance and gait. With the introduction of external fixation they may now be used in combination with internal fixation for further added stability of these bone segments, allowing the patient to perform protected partial to full ambulation postoperatively, which previously required 4 to 8 weeks of non-weight-bearing immobilization.
Hindfoot Procedures
At the hindfoot and ankle levels, arthritis, deformity, and muscle imbalance can be common in the geriatric patient. Similar to the forefoot and midfoot, the causes can also be multifactorial and result from osteoarthritis or stroke. The arthritic events affecting the forefoot and midfoot can also affect the hindfoot and ankle. The ankle, subtalar, and midtarsal (talonavicular and calcaneocuboid) joints can be affected in isolation or combination. These joints are very complex and multiplanar in range of motion. Their 3-dimensional joint motion leads to a combination of arthritic events with joint crepitus at multiple levels. Neuromuscular conditions can affect the distal extrinsic muscles in the lower extremity leading to muscle imbalance, weakness, spasticity, and contractures.
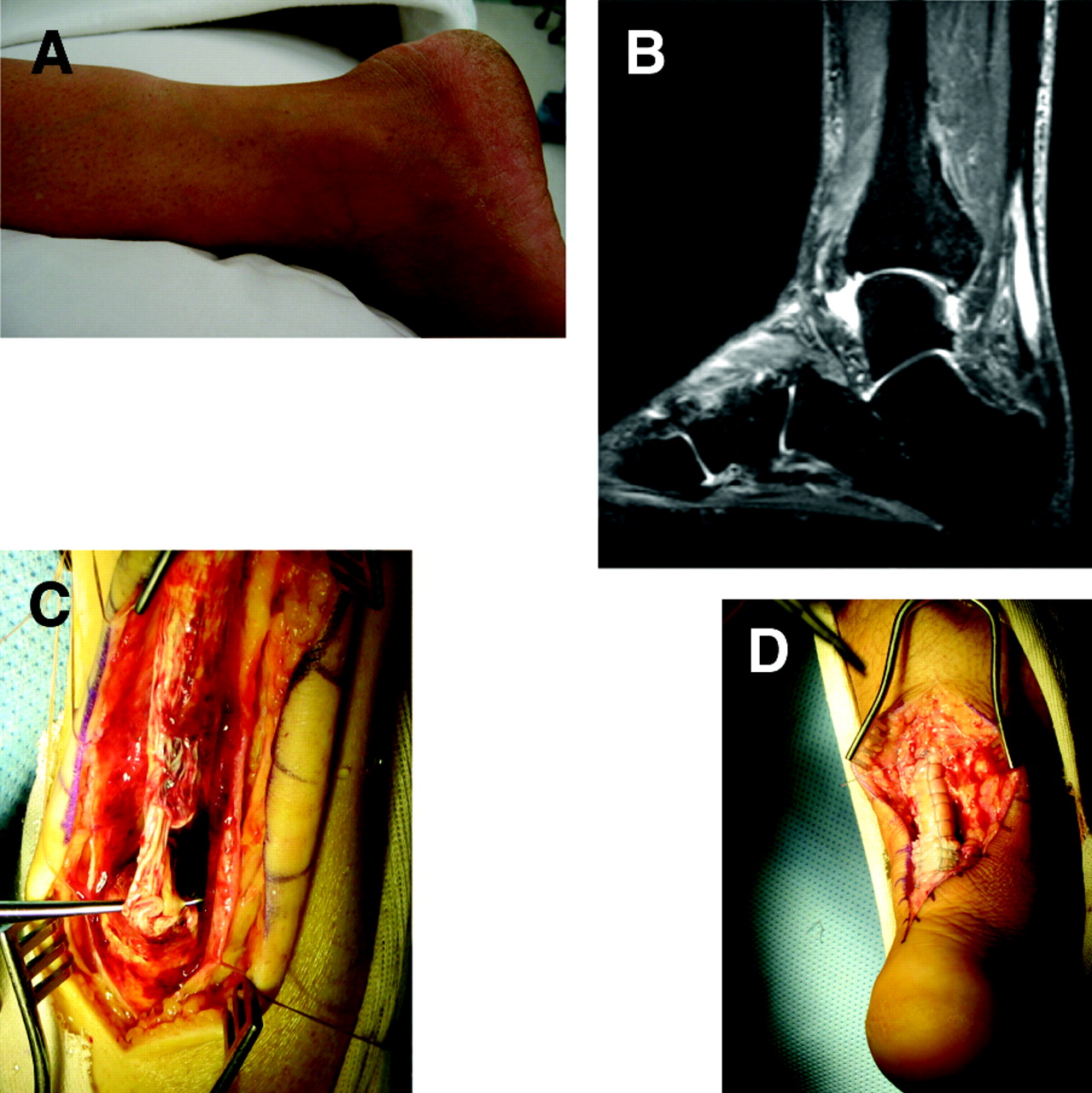
The most common conditions include ankle arthritis, ankle valgum/varum deformity, drop foot, equinus, Achilles partial/full rupture, posterior tibial tendon dysfunction/insufficiency, subtalar arthritis, subtalar valgum/varum deformity, midtarsal joint arthritis, collapsed hindfoot complex, posttraumatic joints, and nonunion/malunion conditions. Typically patients with these conditions complain of pain around the heel and/or ankle. Disability is associated with difficulty standing and/or walking for long distances. It is not uncommon for muscle weakness and imbalance go unnoticed by the patient (Figure 7) During examination the clinician can determine the level of arthritis, misalignment, and deformity through muscle testing and evaluation of range of motion and gait.

Chronic Achilles tendon rupture. Note (A) the clinical view of the interrupted integrity of the Achilles tendon; (B) T2-weighted images of the ruptured Achilles tendon; (C) intraoperative view of the ruptured Achilles tendon; and (D) Achilles tendon reconstruction with graft.
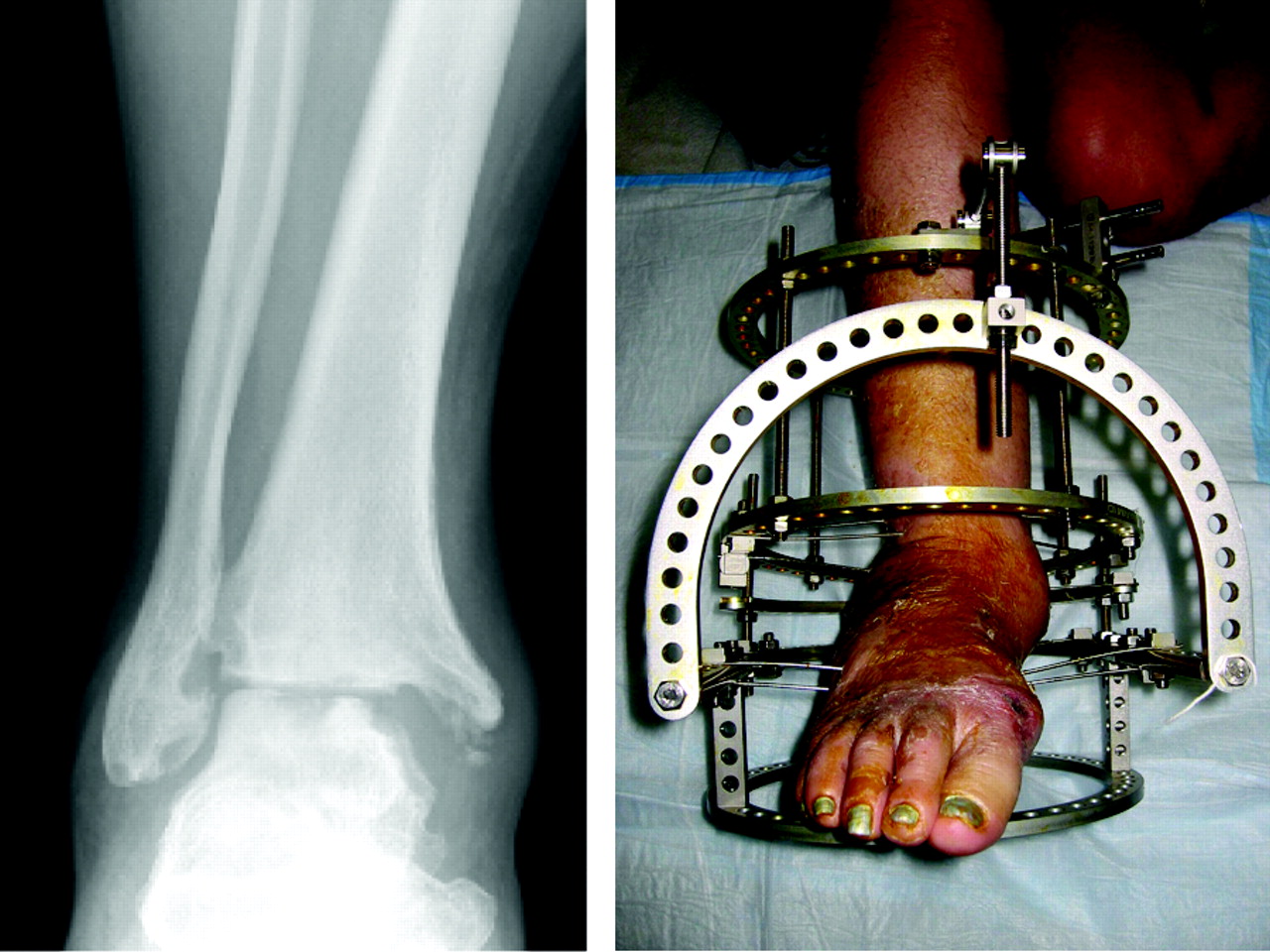
The goals for geriatric hindfoot and ankle surgery are focused on achieving a plantigrade foot, allowing full ground contact, ambulation with a brace, and elimination of the need for a brace.38 Most of these procedures can now be performed under intravenous sedation (monitored anesthesia care) with regional popliteal, sciatic, or femoral local blocks in an outpatient setting. Unlike forefoot and midfoot procedures, most patients are protected with a temporary non-weight-bearing splint, which is then switched to a short-leg partial-walking cast after 2 to 4 weeks, and then to a full-walking cast during the following 3 to 4 weeks. In selected patients, an Ilizarov external fixation may be applied; this can allow postoperative weight bearing beginning in the first 1 to 2 weeks with a walking aid. Patients undergoing an Ilizarov procedure must be selected with special caution because strict compliance is needed (Figure 8). The daily postoperative care for these more complicated procedures are best addressed in a rehabilitative or skilled nursing facility.

Severe ankle osteoarthritis. Note the Ilizarov external fixation for earlier postoperative weight-bearing tolerance.
Arthrodesis of the ankle and subtalar joints is still the gold standard in the treatment of end-stage arthritis (Figure 9). Although joint replacements that provide increased range of motion and flexibility are treatment options, the intermediate and short-term results are not as satisfactory and have higher complication rates compared with knee and hip joint replacements (Figure 10). Until this technology improves, extra-articular arthrodesis and joint resection with synovectomy and debridement are better options for geriatric patients. Isolated midtarsal joints arthrodesis reduces pain and disability as well as total range of motion of the subtalar joint. These procedures can proceed with early weight bearing compared with ankle and subtalar joint arthrodesis. There are currently no replacements available for these joints. Osteotomies in the ankle and hindfoot are viable extra-articular procedures, which preserve joints and provide realignment of the structures.

Subtalar joint arthritis. A postoperative view after isolated subtalar joint arthrodesis.

Ankle arthritis. A postoperative view of total ankle replacement. Note the complete bipolar components for the tibiotalar joint.
Tendinopathies associated the Achilles and posterior tibial tendon are the most frequently performed procedures. Although rupture repairs of the Achilles tendon is normally performed in isolation, repairs of the posterior tibial tendon in isolation without bone correction or realignment do not provide enough stability to hold the correction. Because most posterior tibial tendon conditions occur with progressive pes plano valgus and flatfoot deformity, the correction of bone pathology has priority over the tendon repair. Drop foot requires evaluation of in-phase and out-phase muscles because tendon transfer techniques can prevent ankle arthrodesis.42,43
Well-designed and well-controlled clinical trials among the geriatric population are still needed to validate the improvement in reported clinical outcomes and to assist the primary care provider in giving a more accurate description of outcome expectations to the patient. Advantages, disadvantages, benefits, risks, and time to recovery need to be clearly covered by the surgeon, although it is helpful for the primary care physician to inform the patient of options for which a educational visit and consult with the surgeon may be made. We strongly believe that the geriatric patient who is asymptomatic, able to ambulate without significant difficulty, and who is not in a limb threatening situation should not undergo a surgical procedure simply for cosmetic purposes. The primary care physician must carefully screen and the patient's current medical situation and medical and social history to determine whether surgical intervention should be considered. Patients, regardless of age, commonly anticipate that a surgical procedure will create an “anatomically normal,” fully functional, and completely pain-free foot. Surgical procedures are meant to address problematic foot problems, improve ambulation, and to decrease pain. Patients may need to be educated postoperatively about ongoing, albeit decreased, pain, the need for special shoes, and limitations to daily activities. Patients will appreciate an honest and straightforward explanation of what to expect.
Currently, well-powered and controlled trials are not available to provide evidence-based and statistically significant data about the new and advanced surgeries that result in less pain, decreased recovery time, and improved function scores. The aforementioned lack of studies highlights the need for determining the correlation between perioperative medical management and treatment outcomes, as well as any relationship between newer techniques and surgeries on the elderly and common postoperative complications such as the incidence of deep venous thrombosis/pulmonary embolism (PE), postoperative pneumonia, or postoperative injuries (falls). The rise in numbers of senior patients and the parallel increase in surgeries performed on this population justify the need for such studies to be performed in the near future.
Summary
The increase in the aged population and their continued active lifestyles and a desire for a better quality of life make it important for the health care provider to have a basic understanding of conservative versus surgical options for treatment of the geriatric lower extremity. Surgical versus conservative approaches have been emphasized here; however, potential problems from operative intervention as well as postoperative care need to be discussed in detail with patients and family members. Advanced foot and ankle surgery is not immune from common postoperative orthopedic and cardiovascular complications. Conservative options need to be considered before surgery is recommended. Candidates that do qualify for surgery may now benefit from the advanced and improved treatments that have been developed to address lower extremity problems among the aging population.
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: none declared.
- Received for publication June 8, 2008.
- Revision received October 20, 2008.
- Accepted for publication November 3, 2008.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}