
Abstract
Chronic back pain is among the most common patient complaints. Its prevalence and impact have spawned a rapidly expanding range of tests and treatments. Some of these have become widely used for indications that are not well validated, leading to uncertainty about efficacy and safety, increasing complication rates, and marketing abuses. Recent studies document a 629% increase in Medicare expenditures for epidural steroid injections; a 423% increase in expenditures for opioids for back pain; a 307% increase in the number of lumbar magnetic resonance images among Medicare beneficiaries; and a 220% increase in spinal fusion surgery rates. The limited studies available suggest that these increases have not been accompanied by population-level improvements in patient outcomes or disability rates. We suggest a need for a better understanding of the basic science of pain mechanisms, more rigorous and independent trials of many treatments, a stronger regulatory stance toward approval and post-marketing surveillance of new drugs and devices for chronic pain, and a chronic disease model for managing chronic back pain.
Pain complaints are a leading reason for medical visits.1 The most common pain complaints are musculoskeletal, and back pain is the most common of these. The prevalence and impact of back pain have led to an expanding array of tests and treatments, including injections, surgical procedures, implantable devices, and medications. Each is valuable for some patients, but use may be expanding beyond scientifically validated indications,2–4 driven by professional concern, patient advocacy, marketing, and the media.
More tests and treatments do not simply reflect a greater incidence of back pain. The proportion of office visits attributed to back pain has changed little since 1990.5 In recent National Health Interview Surveys, approximately a quarter of US adults reported back pain during the past 3 months, broadly consistent with previous surveys.5
There are important implications of expanded testing and treatment for back pain. Innovation has often outpaced clinical science, leaving uncertainty about the efficacy and safety of many common treatments. Complications and even deaths related to pain management are increasing.6,7 Despite uncertainties, manufacturers aggressively promote new drugs and devices. However, trust in the science supporting these products is eroded by revelations of misleading advertising,8 allegations of kickbacks to physicians,9 and major investments by surgeons in the products they are investigating.10
We focus here on common management decisions in primary care related to imaging, medication, and referral for injections or surgery. Our goal was not to conduct systematic reviews of each of these or to provide a treatment guide, but to summarize data on recent trends, highlight certain risks, provide conclusions from systematic reviews on efficacy, and comment on practice patterns.
Imaging for Low Back Pain
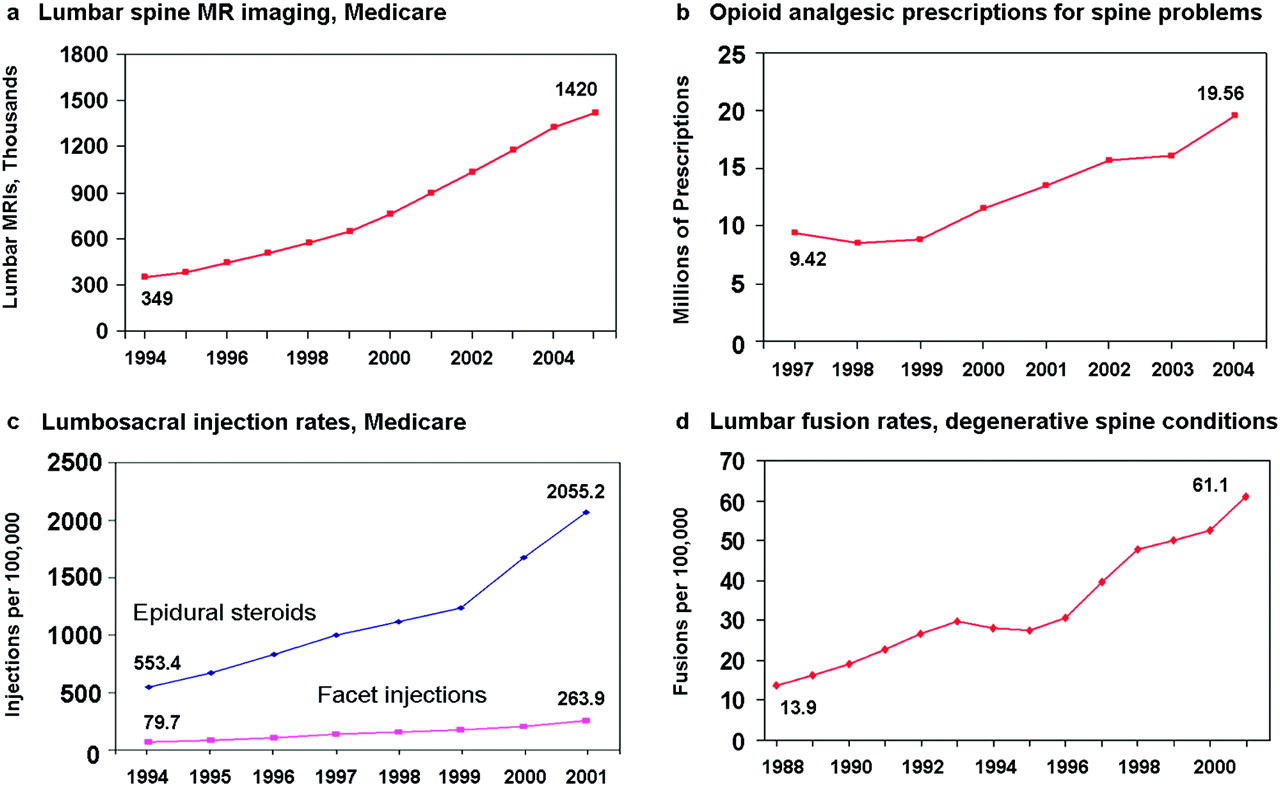
Despite guidelines recommending parsimonious imaging, use of lumbar magnetic resonance imaging (MRI) increased in the Medicare population by 307% during a recent 12-year interval (Figure 1A; previously unpublished data). Others have described rapid increases in spine imaging and for imaging procedures in general.11,12 Spine imaging rates vary dramatically across geographic regions,13 and surgery rates are highest where imaging rates are highest.13 When judged against guidelines, one-third to two-thirds of spinal computed tomography imaging and MRI may be inappropriate.14–16 Many factors probably underlie the growth of imaging, including patient demand,17 the compelling nature of visual evidence,18 fear of lawsuits, and financial incentives.19

Increases in the use of various services for low back pain. A: Lumbar spine magnetic resonance imaging (CPT codes 72148, 72149, 72158); numbers of scans among Medicare beneficiaries from Part B claims. B: Numbers of opioid prescriptions for spine conditions, national data from the Medical Expenditure Panel Survey.11 C: Rates of lumbosacral injections in the Medicare population, age- and sex-adjusted. (Data are from reference 2, adapted with permission.) D: Lumbar spine fusion rates for degenerative conditions, age- and sex-adjusted, National Inpatient Sample. (From reference 3, reproduced with permission.)
One problem with inappropriate imaging is that it may result in findings that are irrelevant but alarming. Positive findings, such as herniated disks, are common in asymptomatic people.20–22 In a randomized trial23 there was a trend toward more surgery and higher costs among patients receiving early spinal MRI than those receiving plain films, but no better clinical outcomes. Six other randomized trials, involving a total of 1804 patients from primary care without features suggesting a serious underlying disease, compared some form of lumbar spine imaging with none.24–29 In these studies, imaging was not associated with an advantage in subsequent pain, function, quality of life, or overall improvement.
Based on an extensive systematic review, the joint guidelines of the American College of Physicians and the American Pain Society explicitly recommend against routine imaging in patients with nonspecific low back pain (ie, no severe or progressive neurologic deficits or evidence of serious underlying conditions).30
Opioid Analgesics
Prescription opioid use is steadily increasing, overall and for musculoskeletal conditions in particular.4,7,31–35 Among patients with spinal disorders, the National Medical Expenditure Panel Survey showed a 108% increase in opioid prescriptions from 1997 through 2004 (Figure 1B). The combination of increasing use and higher drug prices resulted in a 423% inflation-adjusted increase in expenditures.31 These trends have been driven at least partly by concern for the under-treatment of pain in the past, especially among patients with cancer or terminal illness.
Emergency department reports of opioid overdose parallel the numbers of prescriptions.4 Deaths related to prescription opioids have increased; by 2002 there were 4451 deaths related to opioid analgesics, more than the combined total involving cocaine or heroin alone.7 Diversion of prescription opioids is increasingly common, with broad societal impacts.4,36,37
Unlike advanced cancer or postoperative pain, chronic back pain often persists for years or decades. In this setting, the efficacy and safety of long-term opioid use remain controversial. Nonetheless, more than half of “regular” prescription opioid users have back pain.38 A systematic review concluded that, for chronic back pain, short-term advantages over nonopioid analgesics were modest, whereas data beyond 16 weeks were unavailable.39
The Cochrane Collaboration review of opioids for chronic low back pain similarly concluded that, “Despite concerns surrounding the use of opioids for long-term management of chronic [low back pain], there remain few high-quality trials assessing their efficacy… Based on our results, the benefit of opioids in clinical practice for the long-term management of chronic [low back pain] remains questionable.”40 In population-based studies, many patients receiving opioids for noncancer pain have persistent high levels of pain and poor quality of life.41
Ironically, patients with major depression and other psychiatric disorders are more likely than others to initiate and to continue opioid therapy,42 yet they also are more likely to misuse medication43,44 and may be less likely to experience analgesic benefit.45 Although depression and other psychiatric disorders are common among patients with chronic back pain,42,46–48 patients with such disorders are commonly excluded from trials of opioid therapy,42 which raises questions about the generalizability of efficacy studies to routine practice.
Some adverse effects of opioid use may be underappreciated, including hyperalgesia,49,50 which may result from changes in the brain, spinal cord, and peripheral nerves.51–53 In short, opioid use may paradoxically increase sensitivity to pain. Hypogonadism is another underappreciated consequence of chronic use, resulting in reduced testosterone levels, diminished libido, and erectile dysfunction.54–56
The American College of Physicians/American Pain Society guidelines conclude that “opioid analgesics are an option when used judiciously in patients with acute or chronic low back pain who have severe, disabling pain that is not controlled (or is unlikely to be controlled) with acetaminophen and nonsteroidal anti-inflammatory drugs. Because of substantial risks… potential benefits and harms of opioid analgesics should be carefully weighed before starting therapy. Failure to respond to a time-limited course of opioids should lead to reassessment and consideration of alternative therapies or referral for further evaluation.”30
Spinal Injections
The efficacy of spinal injections is limited. Epidural corticosteroid injections may offer temporary relief of sciatica, but both European and American guidelines, based on systematic reviews, conclude they do not reduce the rate of subsequent surgery.57,58 This conclusion is based on multiple randomized trials comparing epidural steroid injections with placebo injections, and monitoring of subsequent surgery rates.59–62 Facet joint injections with corticosteroids seem no more effective than saline injections.57,63
Despite the limited benefit of epidural injections, Medicare claims showed a 271% increase during a recent 7-year interval (Figure 1C).2 Facet joint injections increased 231%.2 Earlier Medicare claims analyses also demonstrated rapid increases in spinal injection rates.12,64 For patients with axial back pain without sciatica there is no evidence of benefit from spinal injections57; however, many injections given to patients in the Medicare population seemed to be for axial back pain alone.2
Charges per injection rose 100% during the past decade (after inflation), and the combination of increasing rates and charges resulted in a 629% increase in fees for spinal injections.2 During this time, the Medicare population increased by only 12%.
Spine Surgery
Although spine fusion surgery has a well-established role in treating fractures and deformities, 4 randomized trials indicate that its benefit is more limited when treating degenerative discs with back pain alone (no sciatica).65 Despite no specific concurrent reports of clarified indications or improved efficacy, there was a 220% increase in the rate of lumbar spine fusion surgery from 1990 to 2001 in the United States (Figure 1D).3 The rise accelerated after 1996 when the fusion cage, a new type of surgical implant, was approved.3 Their promotion may have contributed to both the rise in fusion rates and increased use of implants. In the last 5 years of the 1990s, Medicare claims demonstrated a 40% increase in spine surgery rates, a 70% increase in fusion surgery rates, and a 100% increase in use of implants.66
Higher spine surgery rates are sometimes associated with worse outcomes. In the state of Maine, the best surgical outcomes occurred where surgery rates were lowest; the worst results occurred in areas where rates were highest.67 Multiple randomized trials suggest that adding surgical implants to bone grafting slightly improves rates of solid bone fusion but may not improve pain or function.68–70 Implants increase the risk of nerve injury, blood loss, overall complications, operative time, and repeat surgery.68,69 In a large study of injured workers, the rapid increase in the use of intervertebral fusion cages after 1996 was associated with increased complications but not with improved disability or reoperation rates.71 We recently found that reoperation rates after initial spine surgery were higher in the late 1990s than earlier in the decade, despite greater use of fusion procedures and implants.6
Are We Improving Outcomes?
Jumps in imaging, opioid prescriptions, injections, and fusion surgery might be justified if there were substantial improvements in patient outcomes. Even in successful trials of these treatments, though, most patients continue to experience some pain and dysfunction. Population-level data on back-related dysfunction are sparse. However, despite a rise in costs related to spine problems, the US Medical Expenditure Panel Survey showed that self-reported functional limitations, mental health, work limitations, and social limitations were worse among people reporting such problems in 2005 than in 1997.31
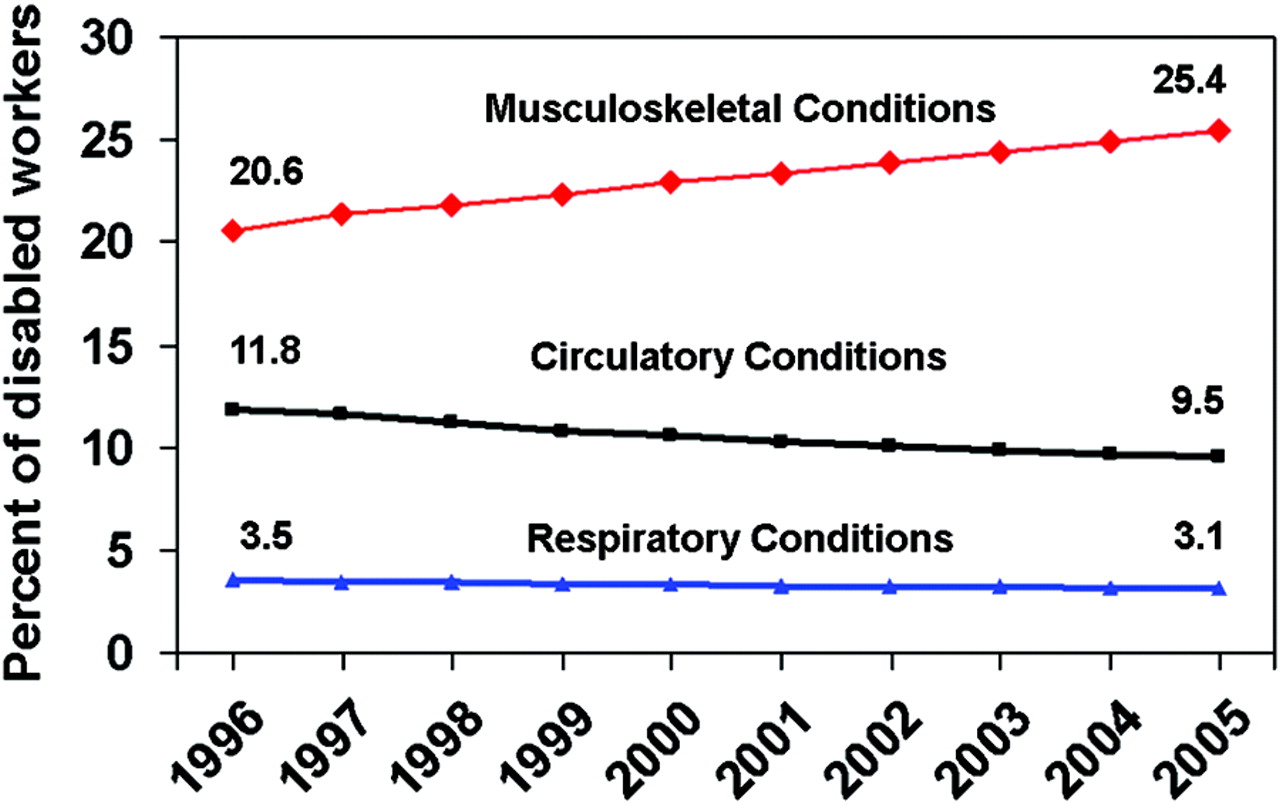
Furthermore, Social Security Disability Insurance statistics suggest that disability from musculoskeletal disorders is rising, not falling. Work disability attributed to musculoskeletal disorders, much of which is back pain, increased from 20.6% of beneficiaries in 1996 to 25.4% in 2005 (Figure 2).72 This was not a growing proportion of a shrinking pie; the number of Social Security Disability Insurance recipients increased over these years. Although it is unclear exactly what proportion of musculoskeletal disability is from back pain, the data suggest that current management of musculoskeletal pain is not highly successful. In contrast, for conditions where effective prevention and treatment have emerged, such as circulatory and respiratory diseases, the proportion of disabled beneficiaries fell.

Percentage of individuals with permanent work disability (Social Security Disability Income beneficiaries) disabled by various medical conditions. (Data are from reference 24.)
Implications and Possible Responses
Prescribing yet more imaging, opioids, injections, and operations is not likely to improve outcomes for patients with chronic back pain. We must rethink chronic back pain at fundamental levels. Our understanding of chronic back pain mechanisms remains rudimentary, including our knowledge of spinal biology, central nervous system processing, genetic factors, and psychosocial and environmental influences. Greater investment is needed in this basic science research.
Clinicians may often be applying an acute care model to a chronic condition. There are no “magic bullets” for chronic back pain, and expecting a cure from a drug, injection, or operation is generally wishful thinking. These approaches risk overlooking the psychosocial, occupational, and lifestyle dimensions of chronic pain. Although evidence remains incomplete and the magnitude of benefits may be modest, data support the benefits of interventions that promote patient involvement and activity (eg, graded exercise programs and group support).73–77 These therapies also have the advantage of being low risk.
A “chronic care model” would acknowledge that chronic back pain, like diabetes or asthma, is a condition we can treat but rarely cure. As with other chronic conditions, care of chronic back pain may benefit from sustained commitment from health care providers; involvement of patients as partners in their care; education in self-care strategies; coordination of care; and involvement of community resources to promote exercise, provide social support, and facilitate a return to work.78,79 Patients need realistic expectations despite product marketing, media reports, and medical rhetoric that promise a pain-free life.
Each treatment and test discussed here has a role in managing back pain, but the evidence base for judicious use remains inadequate. Greater federal involvement in research about therapies and devices may be necessary to provide independent assessments. Initiatives in comparative effectiveness research would be particularly welcome in this regard. Research emphasis should shift from studying fine points of procedural technique to determining who benefits most. Instead of measuring only technical success (solid bony fusion or properly placed injection), research should clarify a treatment's safety and its effects on pain, function, and return to work. Serious complications and unclear benefits highlight the need for more rigorous approval and better post-marketing surveillance of both drugs and devices for treating pain. Without stronger evidence insurers may reasonably question coverage of newer drugs, devices, and procedures.80 In the meantime, we should fully inform patients about available treatment options, including the best available evidence for effectiveness, uncertainties, and risks, and encourage them to play an expanded role in therapeutic decision making.77
Notes
This article was externally peer reviewed.
Funding: Supported in part by grants # 5P60-AR48093 and #5K23AR48979 from the National Institute of Arthritis, Musculoskeletal and Skin Diseases.
Conflict of interest: The research program of Drs. Deyo and Mirza has benefited from a gift to the University of Washington from Synthes, a surgical device manufacturer. They have not received any personal financial support from this source. Mr. Martin has received partial salary support from this source. Dr. Turner has no conflicts to declare.
- Received for publication May 15, 2008.
- Revision received July 23, 2008.
- Accepted for publication July 29, 2008.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Chronic Low Back Pain in Young Adults: Pathophysiological Aspects of Neuroinflammation and Degeneration
- Implementation of the American- College of Physicians Guideline for Low Back Pain (IMPACt-LBP): protocol for a healthcare systems embedded multisite pragmatic cluster-randomised trial
- Co-creating a Choosing Wisely Leaflet Supporting the Reduction of Imaging Usage in Low Back Pain Management - A Multi-Method Study
- Wearable motion-based platform for functional spine health assessment
- ISASS Policy Statement 2022: Literature Review of Intraosseous Basivertebral Nerve Ablation
- Treating low back pain in athletes: a systematic review with meta-analysis
- Predictors of controlled prescription drug non-medical and lifetime use among patients accessing public mental health services in Uganda: a cross-sectional study
- Quality improvement time-saving intervention to increase use of a clinical decision support tool to reduce low-value diagnostic imaging in a safety net health system
- How common is imaging for low back pain in primary and emergency care? Systematic review and meta-analysis of over 4 million imaging requests across 21 years
- Health Care Utilization and Pain Outcomes Following Early Imaging for Low Back Pain in Older Adults
- Clinicians cognitive biases: a potential barrier to implementation of evidence-based clinical practice
- Does changed referral options affect the use of MRI for patients with low back pain? Evidence from a natural experiment using nationwide data
- Diagnosis and management of low-back pain in primary care
- Imaging studies in patients with spinal pain: Practice audit evaluation of Choosing Wisely Canada recommendations
- Stabbed in the back: catalysts for a paradigm shift in back pain care
- The ineffectiveness of paracetamol for spinal pain provides opportunities to better manage low back pain
- Implementation of a Quality Improvement Process Aimed to Deliver Higher-Value Physical Therapy for Patients With Low Back Pain: Case Report
- Common misconceptions about back pain in sport: Tiger Woods' case brings five fundamental questions into sharp focus
- Biopsychosocial care for chronic back pain
- Report of the NIH Task Force on Research Standards for Chronic Low Back Pain
- Physical Therapists' Clinical Knowledge of Multidisciplinary Low Back Pain Treatment Guidelines
- Under- or Overtreatment of Pain in the Patient With Cancer: How to Achieve Proper Balance
- Effect of Stratified Care for Low Back Pain in Family Practice (IMPaCT Back): A Prospective Population-Based Sequential Comparison
- Disabling chronic low back pain as an iatrogenic disorder: a qualitative study in Aboriginal Australians
- Osteopathic Manual Treatment and Ultrasound Therapy for Chronic Low Back Pain: A Randomized Controlled Trial
- It's time for change with the management of non-specific chronic low back pain
- Influence of Nomenclature in the Interpretation of Lumbar Disk Contour on MR Imaging: A Comparison of the Agreement Using the Combined Task Force and the Nordic Nomenclatures
- Content Usage and the Most Frequently Read Articles in 2009
- Optimism: A Good Theme for Family Medicine