
Abstract
Context: Cardiovascular disease is common and preventable. Primary care is the preferred setting for individual prevention and management.
Objective: This study analyzed the long-term outcome of cardiovascular risk in a family practice population.
Design: A longitudinal cohort analysis of cardiovascular outcome after 18 years, in participants of a randomized controlled trial (RCT) of cardiovascular prevention. In 1977, a RCT with cluster randomization at practice level assessed the effects of a 1-year preventive intervention in patients 20 to 50 years of age. Cardiovascular risk factors (smoking, body mass index, blood pressure, serum cholesterol, family history, and physical activity) were measured and intervention was a practice-nurse support for the follow-up of those at elevated risk. The control practices prescribed care as usual. Between 1994 and 1995, all participants were approached again, to analyze subsequent (cardiovascular) mortality and morbidity and their cardiovascular risk in a random sample.
Setting: The Nijmegen Academic Family Practices Network, The Netherlands.
Participants: All participants (7092) of the 1977 screening for follow-up morbidity and mortality, 2600 for re-measurement risk factors.
Outcome measures: Cardiovascular risk factors; cardiovascular morbidity and mortality 1977–1995.
Results: Follow-up was achieved in 5945 participants (84%) and 2335 participated in the re-measurement (89%). No effects of the preventive intervention were found, but those initially at low risk profile were still so 18 years later. Risk of subsequent cardiovascular mortality and morbidity was related to baseline risk, but for women, the absolute risk was low in all risk strata and lower than predicted from international references.
Conclusions: This study demonstrated the feasibility of family practice network research in pursuing longitudinal research. A single cardiovascular screening resulted in reliable risk assessment: those initially at low risk still were so after 18 years. Effects of a 1-year intensive intervention could no longer be demonstrated.
Ischemic cardiovascular diseases belong to the most common chronic disorders in the primary care population contributing substantially to the workload of family practice.1,2 Co-morbidity is a frequent feature of patients with ischemic heart disease,1,3 caused by common causal mechanisms (for example diabetes mellitus or smoking-related chronic obstructive pulmonary disease) and/or as the consequence of ageing. This hampers the effectiveness of treatment, and because cardiovascular disease is preventable, underlines the case of prevention. Effective cardiovascular prevention should be directed at persons at elevated risk4 and involves case-finding through the assessment of risk factors (smoking, obesity, diabetes mellitus, hypertension, hyperlipidemia, family history of ischemic heart disease).5 Primary care is the preferred setting for individual prevention and management but family physicians (FP) find it difficult to relate their efforts to established health gains of their patients: postponement of events or death cannot be measured on an individual level, and care is directed at intermediate targets (smoking cessation, weight-loss, and control of diabetes, blood pressure, and serum lipids). There is substantial evidence of the problems to achieve lasting control over these intermediate targets in itself,6,7 but there is also limited insight in the actual impact of cardiovascular prevention in family practice. For that reason, we followed-up a cohort that had been recruited by their FP for individual cardiovascular prevention, 18 years before. The aim of this study was to assess the long-term outcome of cardiovascular risk in a family practice population and their population-specific risks. Based on the experiences, a practice audit-and-support for cardiovascular prevention was developed.
Methods
The study was a longitudinal cohort analysis of cardiovascular outcome of participants of a randomized controlled trial of cardiovascular prevention after 18 years. Participating practices formed the Nijmegen academic family practices network, the practice-based research network of the Department of Family Medicine Nijmegen (The Netherlands). This network records all episodes of presented morbidity since 1971 in a standardized way, and the process and outcome of a number of chronic diseases (diabetes mellitus, hypertension, asthma/chronic obstructive pulmonary disease) since 1986.8–10
The 1977 study was a randomized clinical trial of the feasibility and the effects of intervention on cardiovascular risk factors in family practice conducted between February 1977 to September 1978.11 The intervention consisted of practice support for preventive cardiovascular care: After cluster randomization at practice level 3 practices received support of a practice-nurse for the follow-up and management of patients at elevated cardiovascular risk. The 3 control practices prescribed care as usual. The intervention lasted for a year.
Participants and Measurements
All patients, born between 1927 and 1957, were invited in for a health screening, when they visited their physician. Assessment of cardiovascular risk factors was done with the help of specially trained assistants. A 33% sample of those who had not come to the practice in that period was invited by letter. This resulted in the measurement of cardiovascular risk factors in 7092 persons. A questionnaire about family risk factors, smoking habits, and physical activity was administered. Blood pressure, height, and body weight were assessed, and a blood sample was taken for serum cholesterol. Blood pressure was taken as the average of 2 readings, measured twice in the right arm of sitting subjects after a 5-minute rest. The fifth phase of the Korotkoff sounds was recorded as the diastolic blood pressure. For subjects with an arm circumference of less than 30 cm, a bladder of 13 × 23 cm was used, and for obese subjects, a bladder of 16 × 23 cm.
Non-fasting serum cholesterol concentration was measured with the Liebermann-Burchard reagent with Huang modification at the Laboratory of the Wageningen Agriculture University. The laboratory participated in the “Cooperative Cholesterol Standardization Program” of the World Health Organization, with the Center for Research in Blood Lipids in Atlanta as reference.12
Socioeconomic class was based on the profession of the participants and divided in 3 categories, upper, middle, and lower.
A cardiovascular risk profile was drawn up for every patient, and the 20% with the highest risk level, the so-called high-risk group, were referred to their FP. The cardiovascular risk allocation was based on BP, smoking habits, serum cholesterol, the existence of diabetes, and family history for cardiovascular disease. Criteria for the high-risk profile were derived from the Coronary Risk Handbook from the American Heart Association,13 without the criteria for electrocardiogram abnormalities
Follow-up Study: Health Status Outcome 1978–1995
Participants
As a first step, it was established whether participants of the screening were still alive and lived in the practice area. The files of the deceased patients were studied for the cause of death. Of those who had moved to another area, their new FP was contacted to establish their current health status. The subjects still living in the practice area were considered for the follow-up study 5945 of cardiovascular morbidity. All patients who had an elevated cardiovascular risk during the 1977 screening, as well as a random sample of 33% of those with a low-normal cardiovascular risk at that time were invited. A total of 2600 patients were invited for re-measurement of the cardiovascular risk factors.
Mortality and Cardiovascular Morbidity
Mortality and cause of death (myocardial infarction, sudden death, heart failure, stroke) and cardiovascular morbidity between 1977 and 1995 were recorded according to the ICHPPC-2-defined criteria14 in the Nijmegen morbidity registration.8–10 For this study, the first onset of angina pectoris, myocardial infarction, and stroke were recruited from the registration as the outcome variable for CVD morbidity.
Cardiovascular Risk Status
Cardiovascular risk status in 1995 was assessed during a re-screening, with the help of specially trained assistants. The assistants who measured in 1995 were blinded to the 1977 findings. For blood pressure measurement, a bladder of 13 × 36 cm was used for every one, according to the present guidelines of the Dutch College of General Practitioners.15
The non-fasting serum cholesterol was measured in the Canisius Wilhelmina Hospital in Nijmegen with an enzymatic cholesterol assay method (Technicon method). The quality control data were analyzed to detect laboratory drifts that could influence the results. The Canisius Wilhelmina Hospital, as a member of the Dutch Foundation of Clinical Chemical Laboratories, meets WHO quality control standards. Because of the careful standardization following WHO quality control standards, it can be assumed that cholesterol values from 1977 and 1995 are comparable.
Body weight was measured, and smoking status and familial risk factors were also administered. Family history of cardiovascular disease was an ischemic cardiovascular event (angina, myocardial infarction, stroke, transient ischemic attack, or peripheral arterial obstruction) and/or sudden death in a first-degree relative before the age of 65 year. Respondents were classified as current smokers, never smokers, and earlier smokers.16–18
Analysis
Normal blood pressure was defined as a systolic blood pressure of <140 mm Hg and a diastolic blood pressure of <90 mm Hg. The high blood pressure group included those currently using antihypertensive medication. The definition of elevated serum total cholesterol was a measurement of >5.8 mmol/L and the definition of overweight was a body mass index measurement of >27 kg/m2. For smoking “past” or “never” were grouped together versus “current”. For analysis of family history, all patients reporting an event in one or more relatives were considered a positive family history, all others a negative one. As no lasting effects of the preventive intervention had been found11,19–21 patients of intervention practices and control practices were combined in this analysis. Cox proportional hazard regression was used with cardiovascular risk status at screening in 1977 to 1978 as the independent variable and the onset of a first cardiovascular disease event as the (dependent) outcome variable. Hazard ratios for separate and combined risk factors and relative risks were estimated. As cardiovascular events were rare in patients 20–30 years at screening in 1977, formal risk calculation has been restricted to the 4207 patients 30–50 years old at baseline (Table 2).
Results
Preliminary Study
In preparing the follow-up measurement differences in medical routines between 1977 and 1995 were identified, but without empirical evidence of their implications. This was in particular the case of the use of cuffs in blood pressure readings –for 1977: in subjects with an arm circumference of less than 30 cm, a bladder of 13 × 23 cm was used,11 and in obese subjects a bladder of 16 × 23 cm., for 1995: a 13 × 36 cm bladder size was recommended irrespective of arm circumference.15 In a comparative study in subjects with different arm circumference, blood pressure readings with cuffs of 13 × 23 cm. and 13 × 36 cm. were taken. In comparing the measurement outcomes, differences were marginal and within the measurement variation,22 which supported the decision to use a 13 × 36 cm bladder size for everyone in the 1995 study.16–18
Longitudinal Analysis
In 1977, 7092 patients participated in the study, of which 1147 had left the practice (area) in 1995. A total of 205 patients had died before 1995, of whom 54 from cardiovascular causes (45 sudden death or myocardial infarction, 9 stroke). Further follow-up was directed at those alive in 1995 (5945 or 84%). There had been 268 cases of non-fatal angina pectoris or myocardial infarction and 69 cases of stroke, transient ischemic attack recorded between 1977 and 1995.
The number of smokers decreased approximately 50% from 63% in 1977 to 35% in 1995 for men (this was 45% and 27%, respectively, for women). Average blood pressure did not increase significantly over the years, but serum cholesterol did, for men and women (Table 1). The number of patients with a blood pressure or cholesterol above the cutoff point, however, did increase (Table 1). For blood pressure, this was partially because of changes in the cutoff point: when the 1995 criteria for hypertension were applied for the situation 1977, 9.5% of the men and 6.5% of the women would have been categorized as hypertensive.16
Development of Blood Pressure and Cholesterol 1977–1995 and Percentage of Categorized Hypertensive, Hypercholestrolemia
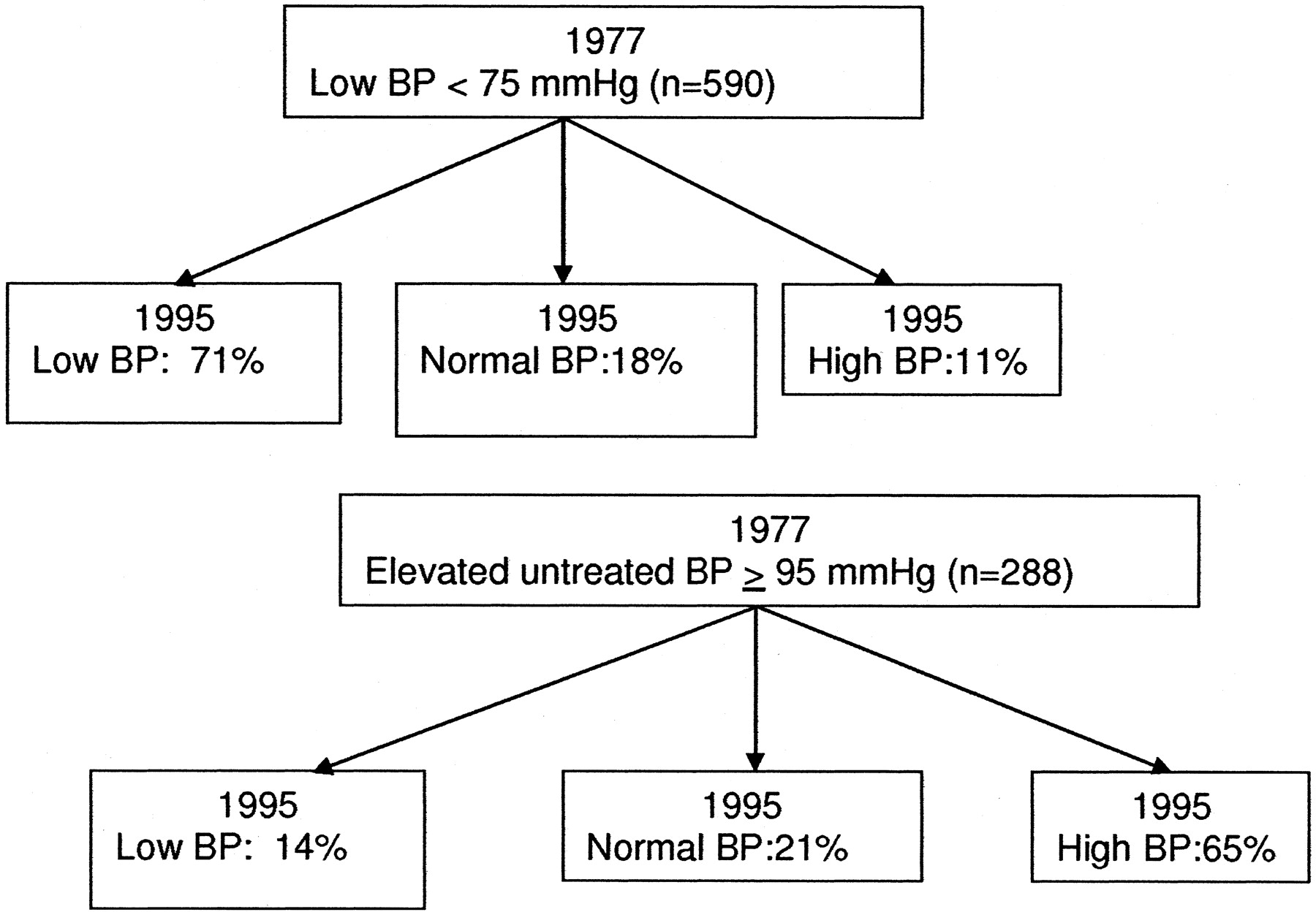
Those initially classified as low-normal blood pressure were for approximately 90% so at follow-up, whereas 65% of patients whose blood pressure had initially been classified as elevated, were still so 18 years later (Figure 1). Table 2 summarizes the relative risk of subsequent cardiovascular mortality and morbidity in relation to baseline risk. All risk factors, and in particular hypercholesterol, were related to cardiovascular morbidity and mortality. The absolute risk of a life-time first myocardial infarction was 3.7 per 1000 for men and 2.7 per 1000 for women.
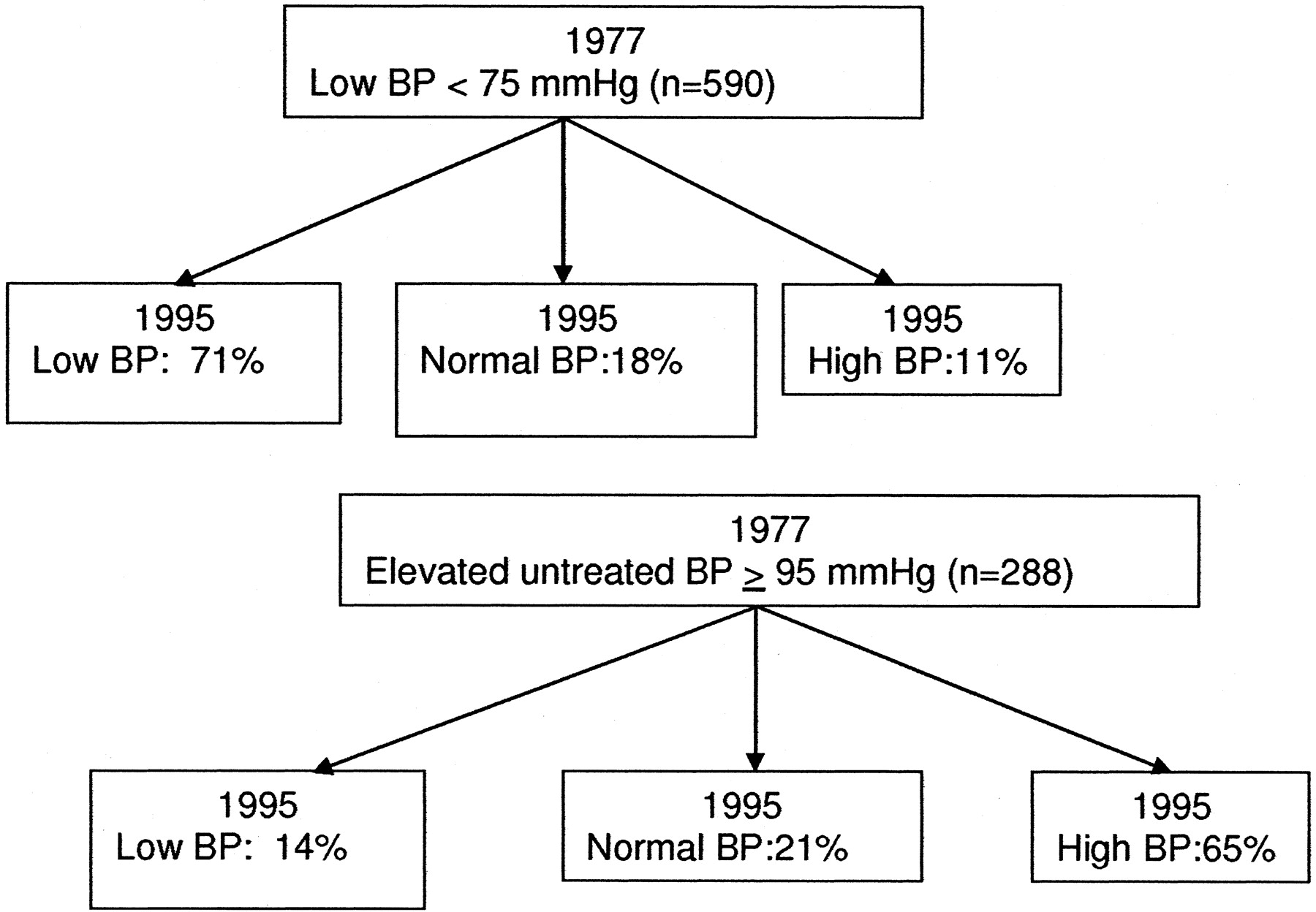
Development of blood pressure from 1977 to 1995 in relation to the diastolic blood pressure (DBP) in 1977.
Number of Participants with Elevated Risk Factors in 1977 and Their Relative Risk (95% CI) of Cardiovascular Events 1977–1995 in the Nijmegen Cohort Study
Discussion
This study assessed in a family practice population the development of blood pressure and serum cholesterol over a period of 18 years and the cardiovascular morbidity and mortality over that period in relation to cardiovascular risk. It demonstrated that a baseline assessment of blood pressure, and to a lesser degree serum cholesterol, correlated well with the patients’ values nearly 2 decades later. This supports the view that a “one-off” screening of these risk factors allows for long-term risk allocation.23 This is important as biological and measurement variation influence measurement. Although for serum cholesterol, there was a clear increase over time, for men and women. Changing population nutrition24 and ageing of the study group might be responsible for this. The yield of hypertension in 1977 would have been much higher, when the prevailing criteria of 1995 were applied.
This may illustrate the effects of changing diagnostic criteria over time, that is an inherent factor in longitudinal research. During the follow-up, the treatment targets became gradually tighter, particularly for hypertension (<140/90 mm Hg)15 and cholesterol (< 5.0 mmol/L)25 and more and more drugs became available. The Nijmegen academic practice-based research network in which the practices participate has over the years adopted these targets and monitored their achievement.10 Outcome of cardiovascular risk in this study reflects the continuous changing potential of care.
This should be taken into account in revisiting the question of why an initially successful intervention petered-out. Usual explanations are patient and physician compliance and the stripping-down of the research setting. In this study the departure of the study nurse practitioners will have had a tangible effect. But although there is no reason to expect these practices to be exempt from such influences, it is also quite likely that changes in the control practices have influenced the results. Pro-active care for cardiovascular risk has been promoted in (Dutch) family practice, for example in the Dutch college’s guidelines for hypertension15 and cholesterol.25 And the Nijmegen academic practice-based research network has developed its methods of audit and feed-back to foster its objectives in routine care. That under these circumstances the benefits of the intervention can no longer be identified, to a large extent, could be because of improvements in the control practices.
Baseline risk factors were related to subsequent cardiovascular risk, in line with previous population risk studies.26–28 But interestingly, the overall degree of risk of this population was lower than of other populations.
The longitudinal study was superimposed on a RCT of the effectiveness of cardiovascular prevention and it may be assumed that participants of this study received treatment of their cardiovascular risk. This could have influenced the rate of cardiovascular disease and mortality and this would have led to an underestimation of the actual risk. Smoking cessation would also have caused this. The decline of smoking in this population was similar to the secular trend in The Netherlands during the study period.29 But similar effects must have influenced the risk assessment over time in other populations, that are often used as reference values for the rationale of cardiovascular prevention recommendations, and in the initial study of this population no lasting effects of a one-year intensive intervention could be demonstrated.20,21 This would still imply that this family practice population had an overall lower risk of cardiovascular events. This is relevant knowledge as it might influence the cost-effectiveness of prevention in this population.
The risk of a lifetime first myocardial infarction was lower than in the Framingham population—that is the risk-table evidence on which global cardiovascular screening is based. This is in line with other (European) populations30 and emphasizes the need of population-specific research. This lower risk came down even further during the study period; we could demonstrate a decline in the incidence of first myocardial infarction between 1975 and 2003.31
This emphasizes the importance of studying populations under care for their own characteristics of their health status: it is only to a certain degree possible to generalize findings from one population to another. That is also true for the findings of this study that took place in an academic family practice network. The FPs and their care can for that reason not be generalized. But practices provided care for unselected groups of patients, living in the communities the practices serve. As a consequence, the data for cardiovascular risk in relation to cardiovascular morbidity can be generalized –with all the caveats stressed above.
A particular point of this study was that it demonstrated the feasibility of a family practice network research in pursuing longitudinal research. This emphasizes the role of practice-based research networks to track patients’ careers and morbidity events of time,9 which can make a powerful contribution to clinical research.
Notes
This article is based on a presentation made at the 2005 Convocation of Practices, hosted by the American Academy of Family Physicians National Research Network and the Federation of Practice-based Research Networks, Colorado Springs, CO, March 2005.
- Received for publication June 9, 2005.
- Revision received September 14, 2005.
- Accepted for publication September 30, 2005.
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.