
Abstract
Background: This study describes the contributions of family and general practice physicians from Wyoming to the health care safety net.
Methods: We surveyed family and general practice physicians in Wyoming about provider demographics, practice composition, and policies for treating the underinsured or uninsured. Two-tailed χ2 tests and limited logistic regressions were used to test for differences among characteristics of safety net providers.
Results: From a 50% response rate, 61% made less than the national mean family physician income ($130,000), and women are less likely than men to make this mean income, even when controlling for hours worked (OR, 0.09; CI, 0.009, 0.862). Close to two thirds claimed bad debt of over $10,000, and 29.3% noted forgiven debt of over $10,000. Physicians with less income than the prior year were more likely to decrease their charity care.
Conclusions: Wyoming family and general practice physicians provide significant amounts of informal safety net care, which is threatened by income loss. Thoughtful public policy is needed to ensure that vulnerable rural Americans have access to care that is not tied to the financial well being of their health care providers.
In 2003, the U.S. Census Bureau reported that 43.6 million Americans were uninsured, with a disproportionate number of these uninsured residing in rural areas.1 These Americans, their underinsured counterparts, and even their Medicaid- or Medicare-insured counterparts increasingly relied on a loose and informal network of public and private health centers and hospital emergency and urgent care departments for all or parts of their care. For these services, the term “safety net” has been applied, which can include charity care and bad debt. Charity care is free, discounted, or forgiven charges for care delivered to those deemed unable to pay all or a portion of their billed care and can apply to the uninsured along with the publicly and privately insured. Bad debt comprises losses from services for which a bill was submitted and the patient was expected to pay.2
Several studies have noted that the safety net is tenuous, with physicians accepting financial burden when caring for the underserved.3–5 Rural private physicians are not only a main source of care for these Americans, they also provide stability in communities with fewer resources.4
This capacity to provide charity care is dynamic. Studies suggest that 28 to 33% of American physicians do not provide charity care.6 The Center for Studying Health Systems Change demonstrated the proportion of physicians providing charity care dropped from 76% to 72% between 1997 and 1999. In 2003, it reported the safety net had deteriorated in 25% of the surveyed communities.7 At the same time, between 2001 and 2003, 1.6 million Americans were removed from publicly financed health care programs, with 34 states cutting their Medicaid budgets.8
A 2002 study in New Mexico found the reduced availability of Medicaid funding to be largely accommodated through provider increases in workload and financial stress.9 Among the 246 rural counties in a study specific to the rural safety net, 17% were at risk for losing access to charity care services because of the negative operating margins of their hospitals.10
Our study followed site visits to 7 rural communities, where between 20 and 40% of the residents were uninsured or underinsured. Interviewed physicians indicated that private primary care practices were important providers of free or subsidized care.11 The current study describes the safety net participation of primary care physicians in one largely rural western state, Wyoming, where 16.4% of the residents are uninsured, compared with 14.7% nationally. U.S. Census Bureau information for those without health insurance for the year; national average is from 2001. The Wyoming average represents 3 years, 2000–2002 〈http://www.census.gov/hhes/hlthins/hlthin02/hi02t4.pdf〉.
Methods
Study Design
A 2-page questionnaire was sent to all 161 family practitioners (FPs) and general practitioners (GPs) identified by the Wyoming Medical Association as practicing in the state.
Survey Development and Administration
Survey questions were developed following the series of rural site visits that led to this study.11 The survey collected provider demographic and practice information, including age, gender, years in practice, specialty, hours worked per week, hours spent in direct patient care, type of practice and ownership, and practice policies regarding caring for Medicaid patients and patients needing other payment options. We asked respondents to estimate the proportion of all patient visits covered by different payment possibilities (ie, private not discounted, private discounted, Medicare or Medicaid, free care, sliding scale, negotiated installment plan, bad debt, and debt forgiveness) and to note changes in policies during the prior 2 years. We defined free care as care that was given away with no attempt to bill. We defined bad debt as care that was billed but not collected, and debt forgiveness as care that was billed, negotiated, and nonpayment of the whole or portion forgiven. We asked respondents whether their net salary was more or less than the mean income for family physicians in that year ($130,000). Last, we asked them to comment on their contribution to charity care relative to others in the community and relative to their practices 2 years earlier.
The questionnaire was tested with 7 (4 rural) family practice physicians in Washington state and revised with a 15- to 20-minute completion time. An introductory letter was co-signed by a family physician representing the state’s medical association. Surveyed physicians received up to 3 mailings.
Data Analysis
Data were double entered to ensure accuracy using EpiInfo 6.0, and were analyzed in SPSS 10 for the Macintosh. Respondent physician zip codes were used to classify their rural-urban commuting area (RUCA) codes.12 This geographic taxonomy is based on U.S. Census Bureau-designated urbanized areas and places and work commuting patterns, and it categorizes areas as urban, large rural, small rural, and isolated smaller rural.
Our main interest was to describe the characteristics associated with larger (versus smaller) contributions to care for the underinsured and uninsured. When comparing groups, we used 2-tailed χ2 tests to test for the significance of differences (eg, gender and percentage of visits that were publicly funded). Because of the small sample size and the variable number of missing values for different questions in the study, we collapsed some responses into dichotomous categories based on closest quartiles or medians. We performed limited logistic regression analysis to control for possible associations with income level and to explore possible predictors of a decreased amount of charity care over the prior 2 years.
Nonrespondents were compared with respondents, and there was no statistically significant difference based on rural or urban location, or by gender.
Results
Physician Characteristics
The response rate was 50%. The mean age of responding physicians was 45.8 years, and 83.1% were male. They had been in practice for a mean of 15 years (range 2 to 40 years), with a mean of 11.5 years in their current practice location. Approximately 39.0% of respondents had been in their Wyoming community ≤7 years, with only 5.2% having practiced in their communities ≥25 years. Of respondents, 88.2% were FPs and 11.8% were GPs.
The majority of respondents (47 or 60.3%) reported making less than $130,000, the national mean for FPs in the study year (Table 1). Women physicians earned significantly less than their male counterparts. When we controlled for gender, hours of direct patient care, years in practice, and urban-rural practice, only female gender remained significantly associated with income less than $130,000 (OR = 0.09, CI = 0.009, 0.862).
Characteristics of Wyoming Physician Respondents by Income
Between the 2 income groups, there was little variability in employer or practice type. Overall, however, only 11.7% of respondents were employed by a hospital, whereas 40.3% were in solo, self-employed practices. The number of years in practice was not associated with income differences.
Fewer than 25% of physicians answered that they spent under 35 hours a week on direct patient care, whereas 50% said they devoted at least 45 hours per week to direct patient care (not tabled). Reported office-based ambulatory patient visits per week ranged from 12 to 200 per physician, with a mean of 88. Other patient care visits included means of 11.7 inpatient visits, 6.3 emergency department visits, and 5.2 nursing home visits per week.
Characteristics of the Safety Net
The typical physician had a combined 43.2% of visits that were with public insurance patients and/or lost to debt forgiveness, free care, or bad debt. Only 15% reported having no discounted visits.
Public Insurance: The Formal Safety Net
Approximately 47% of physicians reported more than 30% of their patient visits were with patients who had Medicare, Medicaid, or other public insurance discounts (Table 2). Only one respondent did not care for Medicaid patients, and 84.4% had limits in caring for Medicaid patients. Limitations included limiting the number (13.6%), limiting the age (6.8%), limiting care to those already in the practice (6.8%), and limiting care to emergencies only (6.8%) (not tabled).
Physicians’ Reporting of Proportion of Ambulatory Visits by Payment Types
Charity Care, Sliding Scales, Debt Forgiveness, and Other Parts of the Safety Net
Only 17.2% of respondents claimed more than 10% of their visits were billed on a sliding scale, and 59.4% claimed no visits with a sliding scale (Table 2). The decision to offer a sliding fee scale did not differ by years in practice, income, or gender of responding physician.
More than 3 in 4 FP/GPs said they offered free care, debt forgiveness, and had billings for which they did not collect (bad debt), with 4.8%, 6.3%, and 30.2% reporting greater than or equal to 10% of their visits attributed to free care, debt forgiveness, or bad debt, respectively (Table 2). In addition, consistent with the prevalence of insurance discounts, only 9.5% responded that they gave no insurance discounts (not tabled).
The Distribution of Charity Care
There was a significant difference among physicians when comparing those who had greater than or equal to 10% of their visits as nonpaying (free care, debt forgiveness, or bad debt) with those who had fewer than 10% as nonpaying, regarding their perception of whether charity care was evenly or unevenly distributed in the community (P < .05) (Table 3). Of those having fewer than 10% of their visits as nonpaying, 87.1% perceived the distribution to be uneven compared with 67.7% of those with 10% or more.
Distribution of Physicians by Proportion of Visits That Were Nonpaying* and by Physician Characteristics
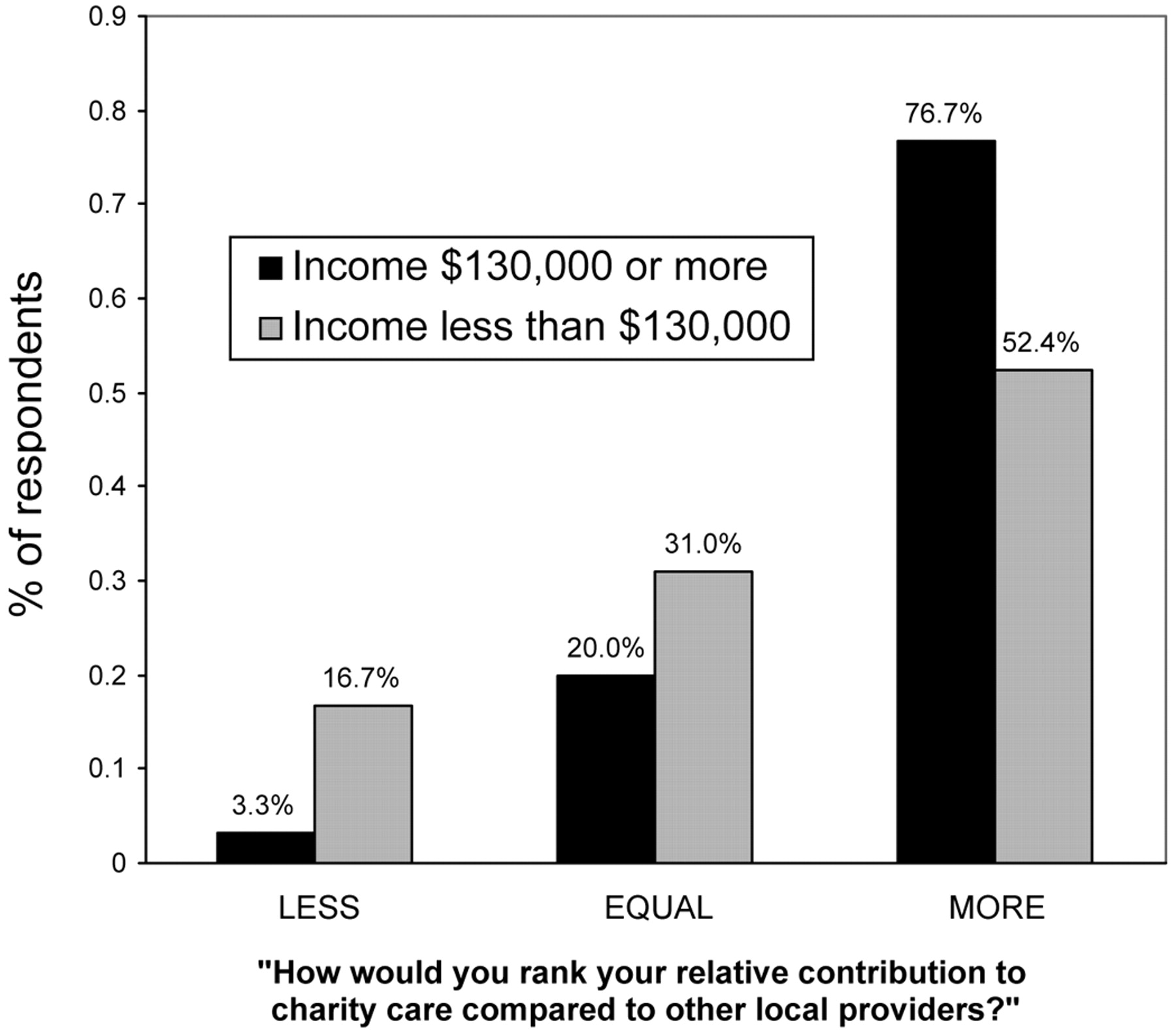
Income was not significantly associated with the perception of one’s relative contribution (Figure 1).

Perceived Relative Contribution of Charity Care by Income of Physician.
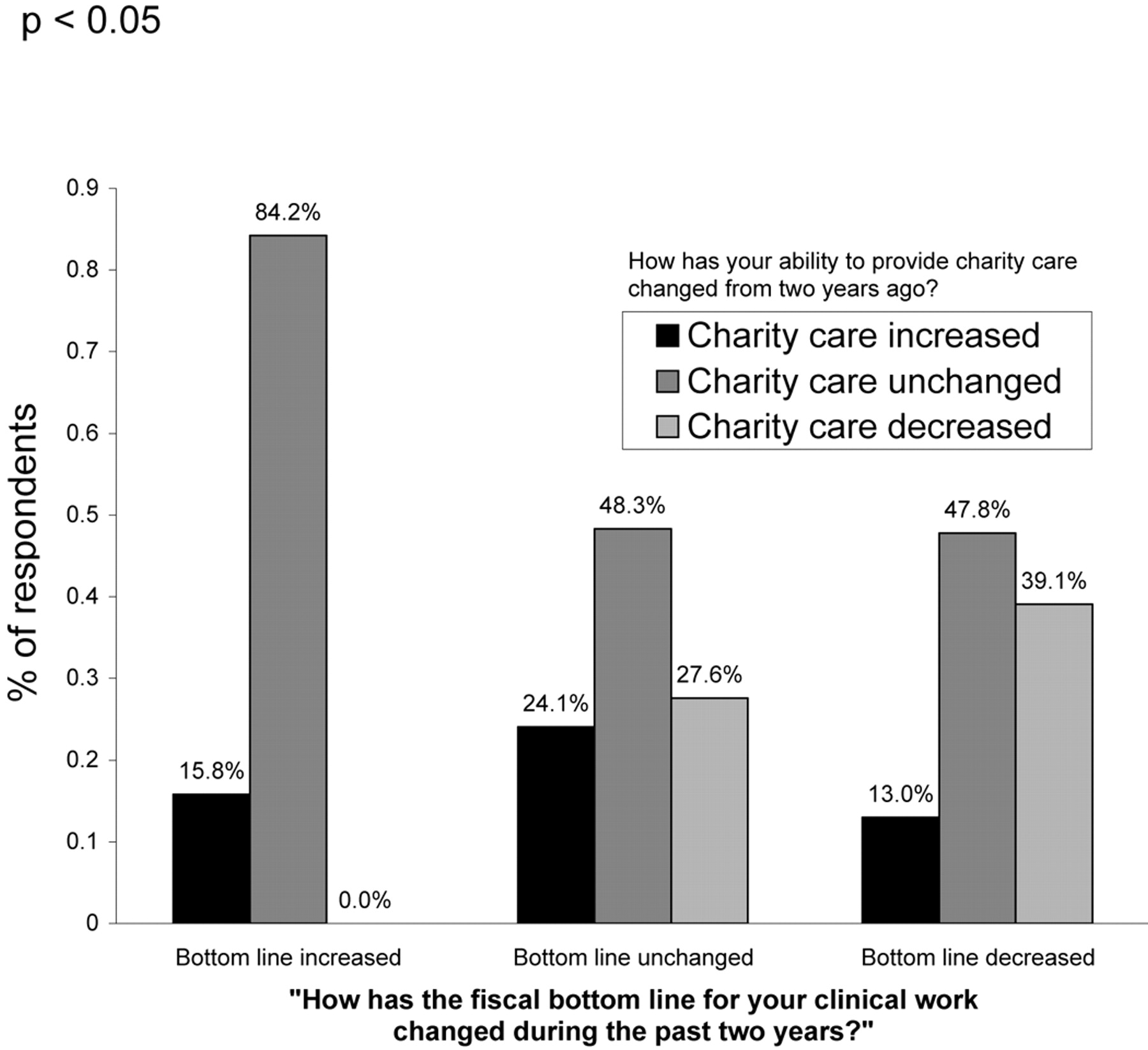
The perception of overall fairness did vary significantly, however, by the physician’s view of the burden s/he had. Of those who perceived the situation as uneven, 75.4% indicated they did more than their share (P < .000) (not tabled), compared with 17.6% of those who thought the burden was distributed evenly. None of those who reported an increase in income during the previous 2 years said they decreased their charity care contribution, whereas 39.1% of those whose income had decreased also decreased their provision of charity care (P < .05) (Figure 2).
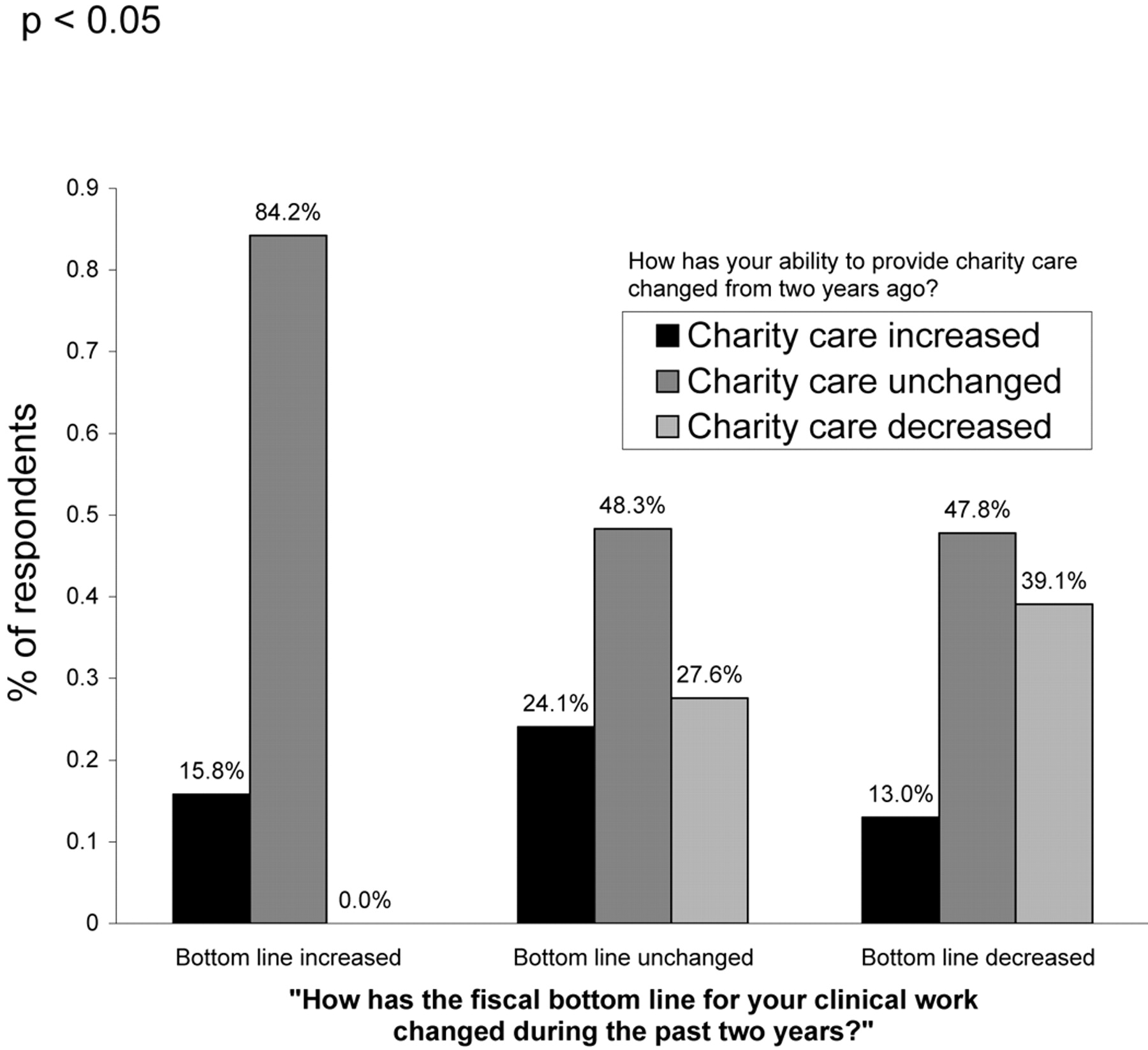
The Relationship between Recent Changes in the Respondent Physicians’ Clinical Income and Changes in the Amount of Charity Care Provided.
Costs of the Safety Net
Respondents were asked to report the extent of their charity care in both percentage of visits as well as dollar amounts, estimating numbers for publicly financed patients, bad debt, free care, sliding scale, and installment plans, as well as the portion of visits that were on private insurance discount. The survey question required that respondents account for all the care they provided for which they did not receive full reimbursement. Although 56.6% of FP/GPs had unbilled charges estimated between $1,001 and $10,000, another 30.4% estimated unbilled charges as greater than $10,000 (Table 4). The range was from $500 to $50,000. Only 4 respondents (9.8%) said they forgave zero debt. Twelve physicians (29.3%) forgave more than $10,000 in debt during the prior year (Table 4).
Costs to Physicians Participating in the Safety Net
Most physicians reported bad debt. Of those who estimated a dollar amount for bad debt, 28.3% said they had lost more than $50,000 (Table 4). The median for free care (not billed), forgiven debt, and bad debt was $39,000, with a mean of $54,283 per physician. Only 26.7% of physicians reported that their collections came to 90% or more of billed charges. A small portion (11.7%) said they collected under 60% of billed charges.
Who Decides about Charity Care?
Most respondents (75.6%) made their own charity care policies. Almost one fourth (23.1%) said their ability to provide charity care had decreased compared with 2 years ago, whereas 16.7% said they were able to provide more. In comments made on the survey, several of those who were providing less said their overhead had increased whereas their incomes had not. Several indicated a belief that Medicare prohibited variation in fee structure or made fiscal accommodations for non-Medicare insured patients. Income, income changes, years in practice, and gender did not significantly predict a decrease in charity care from prior years.
Conclusions
Wyoming FP/GPs, 75% of whom practiced in rural areas, were an important part of the informal health care safety net for vulnerable people in their communities. Although most of the physicians were not earning a mean income of $130,000, most of the respondents perceived themselves to be doing their share in caring for those who could not pay for services.
Most respondents, especially if they reported doing more than their share, thought the safety net burden was not evenly shared within their communities. It is possible that our respondents are a biased group from those more likely to provide more of this care. Alternatively, this finding may simply be representative of the tendency of people to see themselves as above average.
Perhaps most important, those whose bottom line declined or remained static were more likely to have decreased their level of charity care contribution. The finding that charity care declines with declining income is salient. With the average respondent attributing 43% of visits to public insurance, debt forgiveness, free care, or bad debt, these physicians are particularly vulnerable to any decrease in income. With flat Medicare funding and cuts in Medicaid eligibility and scope of coverage, more Americans will become underinsured or uninsured. The need for the safety net will be increasing just as the ability and willingness of these providers to participate is eroded further.
The high-giving group was different from those giving less in other ways as well. Those earning above $130,000 were more likely to perceive themselves as doing more, and women were more likely than men to think the burden was shared evenly.
The main limitation of this study was the small number of responding physicians. Second, we know little about the nonrespondents except that they do not differ by gender or community size. Our respondents also do not differ significantly in age distribution or gender from all primary care physicians (family medicine, internal medicine, pediatrics) in Wyoming.13 We could not ascertain whether nonrespondents differ from respondents in the care of the underinsured or uninsured. Although a higher response rate would improve the power to discern statistically significant differences between different groups of interest, the respondents do represent half of all the FP/GPs in Wyoming.
Third, the physicians in this study are from only one state and one discipline; this raises questions about the generalizability of the findings. FPs and GPs do, however, account for 62.7% of the primary care doctors in Wyoming.13 Fourth, we cannot differentiate between proportions of physician visits to Medicaid as opposed to Medicare patients. The 2 programs have different discounts for some services. We did not explore the differences among Medicare, Medicaid, and private insurance discounts. Last, more work is needed to replicate and externally validate these findings and to examine both rural and urban components of the provider safety net.
Based on our participation in the previously cited safety net case study,11 we conjecture that physicians do not like to think about how much care they are giving away and actually may be underestimating the amounts. Indeed, during some of those case study visits, physicians said we were welcome to look at their records but to please not inform them of our specific findings. They did not want to know what they were giving away. There are likely complicated psychological and economic reasons for this that have not been explored. Several respondents in this study indicated that they believed Medicare puts constraints on what can be given away, so some of the reticence to discuss the issue may be because of fear that disclosure of charging some patients less could be viewed as unethical or fraudulent. Alternatively, some physicians may choose not to know because of a concern that knowing might influence them to not provide needed care to the vulnerable in their communities. The overall reluctance to discuss may also help explain our relatively low response rate for this study.
Nonetheless, physicians in this one largely rural state, Wyoming, were providing safety net care, serving the uninsured and underinsured, including the publicly insured and other patients with notable discounts. Despite the effects on their economic bottom line, they supported the health care infrastructure in their communities and helped those who had difficulty paying for necessary care.
Whereas the nation’s underinsured and uninsured are increasing, the federal government has taken steps to increase certain components of the formal structure or formal safety net. For instance, a significant increase in funding to increase both capacity and geographic coverage of federally funded health centers is in process. Nevertheless, many Americans still depend on a safety net for their health care characterized by an informal system of individual physicians, hospitals, and other care providers in communities, all of whom absorb loss or displace it to other patients. In Wyoming, a substantial portion of safety net care is provided informally by the family and general physicians.
Our study gives shape and definition to one part of the safety net and raises the question whether relying on private physician good will is the most rational approach to providing a secure health care delivery system for rural or poor Americans, especially when we see that physicians with decreasing incomes report delivering less charity care. Although there are many who argue that physicians are no longer charitable and altruistic, these results show that Wyoming FP/GPs provide substantial amounts of charity care at no small expense to themselves.
It is important to know about this part of the safety net to ensure the policies do not hinder the charity care efforts of FPs and GPs. A thoughtful public policy—formed collectively by physicians, patients, and others—is required to strengthen the safety net at levels other than individual examination rooms.
Acknowledgments
We appreciate the assistance of the Wyoming Medical Society in conducting the survey of family physicians required for this study. The opinions expressed in this article are solely the responsibility of the authors. Contributorship: Sharon Dobie designed the study and the instrument, conducted the study, and was a primary person involved in interpretation of the data, writing, and revising the manuscript. Amy Hagopian was a primary person involved in analyzing the data, interpretation of the data, and writing the manuscript. Beth Kirlin was involved in the analysis of the data. Gary Hart designed the study and the instrument, conducted the study, and was closely involved in interpretation of the data and writing the manuscript.
Notes
Funding: This University of Washington Rural Health Research Center study was funded by the federal Office of Rural Health Policy, Health Resources and Services Administration, Department of Health and Human Services.
Conflict of interest: none declared.
- Received for publication March 24, 2005.
- Revision received July 28, 2005.
- Accepted for publication July 29, 2005.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.