
Abstract
Background: The doctor-patient relationship has been eroded by many factors. Would e-mail enhance communication and address some of the barriers inherent to our medical practices?
Methods: Of our study population, 4 physicians offered e-mail communication to participating patients and 4 did not. Both patients and physicians completed questionnaires regarding satisfaction, perceived quality, convenience, and promptness of the communication.
Results: Patient satisfaction significantly increased in the e-mail group compared with the control group in the areas of convenience (P < .0001) and the amount of time spent contacting their physician (P < .0001). Physician satisfaction in the e-mail group increased regarding convenience, amount of time spent on messages, and volume of messages. The response time was longer with e-mail. When asked if patients should be able to e-mail their physicians, most patients in the e-mail group and all but 2 of the physicians in the non–e-mail group responded “yes.”
Conclusion: E-mail communication was found to be a more convenient form of communication. Satisfaction by both patients and physicians improved in the e-mail group. The volume of messages and the time spent answering messages for the e-mail group physicians was not increased. E-mail has the potential to improve the doctor-patient relationship as a result of better communication.
Effective communication between patients and doctors has always been the hallmark of a mutually beneficial doctor-patient relationship, contributing to improved clinical outcomes and high rates of patient and physician satisfaction. New technology can dramatically change that communication, from the invention of the telephone in 1876 to the more recent electronic mail (e-mail). These technologies revolutionize doctor and patient contact, with potential benefits tempered by concerns including privacy, security, and unwanted daily intrusions.1,2
Internet use is increasing dramatically and many individuals are using e-mail to communicate with family or friends about health issues.3–5 In one study by Neill et al, 85% of patients believed e-mail “would be a good way for a patient to communicate with his/her physician.”6 Another study suggested that roughly one half of the patients in 2 large primary care centers used e-mail, but only 10.5% had ever used e-mail to communicate with a physician.7 However, 70% of these patients indicated a willingness to use e-mail communication with their physician. In a survey of primary care physicians in Boston, 75% of physicians reported using e-mail with patients, but only with a small subset (5% or less) of their overall patient population.8
When patients e-mail their physicians, the purpose is primarily for prescription refills, nonurgent consultations, and to obtain laboratory test results.9 Physicians’ responses to these e-mail communications range from no reply to providing detailed information.10 This emerging technology, with its variable application to and impact on the doctor-patient relationship, has prompted the American Medical Association to produce the “Guidelines for Patient-Physician Electronic Mail.”11
Benefits and risks associated with using e-mail communication have been identified.12–19 Rapid, inexpensive, simple, convenient, and asynchronous communication are distinct benefits that could result in a reduction in the number of nonurgent telephone calls to the office, an increase in patient participation in medical decision-making, and an improved linkage to patient education materials.20 Concerns about privacy and security, inappropriate use for acute serious illnesses, potential for increased physician workload, and legal liability are serious limitations. Physician concerns regarding time consumption, however, may be overstated.21,22 Patient concerns regarding e-mail communication include routing the message to the right person, length of time for a response, and privacy issues.7
Despite these concerns, e-mail communication between patients and their physicians is likely to increase and may result in a reconfiguration of physician office function.23–26 Therefore, further assessment of patient and physician satisfaction with e-mail communication is indicated. In this article, we report on a 6-month assessment of patient and physician e-mail communication focusing on the following aspects of this interaction:
Patient and physician satisfaction
Perception of convenience
Turnaround time for physician response
Volume of messages received from patients
Types of messages
Physician time requirement to address messages
Methods
Study Population
This Institutional Review Board-approved study was conducted from December 2001 to July 2002 in a faculty-based clinic affiliated with The Penn State Milton S. Hershey Medical Center. The majority of the practice’s patients come from middle- to upper-income communities with high employment rates. Almost all patients have health insurance, including 24% Medicare and 3% Medical Assistance. Only 3% of the patient population have no insurance. Eight family physicians agreed to participate in the study. The investigator assigned the physicians into one of 2 groups: the intervention group, which offered e-mail communication to patients, and the control group, which did not. This assignment was used to achieve a comparable profile for the 2 groups in terms of physician age, sex, and attitude toward offering e-mail access to patients, as well as age of patient population (Table 1).
Selected Characteristics of Participating Physicians at Baseline
Recruitment
The inclusion criteria for patients were regular use of e-mail and an existing doctor-patient relationship with one of the participating physicians. During the enrollment period, the office nurses screened all patients who came in for a scheduled appointment with 1 of the 8 participating physicians. The screening consisted of the nurses’ asking whether the patient used e-mail regularly. Patients who said yes were then asked whether they were regular patients of the participating physicians. The nurses also review the patients’ medical records to confirm that they have seen the physician at least 3 times in the past. Those patients identified as regular patients of the participating physicians and that use e-mail regularly were offered an opportunity to participate in the study. Consented patients of doctors in the intervention group were given their physician’s e-mail address for communication. Patients of physicians in the control group were not given e-mail access.
Procedure
A separate e-mail account was established for each of the 4 physicians in the e-mail group following pre-existing guidelines for doctor-patient e-mail at the Hershey Medical Center. These guidelines were adopted from a white paper by Kane on “Guidelines for the Clinical Use of Electronic Mail with Patients.”23 Patients were advised not to use e-mail for emergency or urgent matters that could not wait 3 to 5 days, or issues they felt were sensitive/confidential. An auto-reply feature informed patients of the receipt of their message or if the physician was away for an extended period of time. The e-mail system used for this study was set up by the information technology department specifically for this study and was established within a secure server. Patients in both the e-mail and control group were referred to the patient education web site, http://www.familydoctor.org, created by the American Academy of Family Physicians for health and drug information.
During office hours, clinic secretaries recorded all phone calls from patients to the e-mail and control group physicians on standard message slips. Using these message slips, the physicians recorded their responses to patients, which were later filed in the patients’ records. For data analysis purposes, a copy of all patient messages was collected over a week at baseline and 3 selected weeks during the 6-month study period for data analysis. Phone messages received after normal hours were not tracked. E-mail messages were automatically recorded electronically, and copies of the initial message, physician reply, and subsequent communications (if any) were filed into the patients’ charts. During the 3 selected weeks, all physicians completed a time log and recorded the number of messages received and time spent in answering patient messages each day. All participating patients and physicians completed satisfaction questionnaires at the onset of the study and at the 3-month and 6-month intervals.
Survey Instrument
On the patient questionnaire, participants were asked their age, sex, number of years in the practice, level of education, and comfort and frequency of e-mail usage. Patients were also asked whether they used the Internet for various purposes, including locating health information. In part 2 of the patient questionnaire, patients were asked to rank on a 5-point Likert scale their satisfaction regarding ease and convenience of communication with their physician, promptness of the reply, quality and amount of information in the reply, and the quality of home care instruction they received. They also were asked to rank the health information web site in terms of usefulness and frequency of use. On the physician questionnaire, the physicians were asked similar questions, except that in part 2, they were asked to rank their satisfaction with the practice’s message system overall and the amount of time to reply to messages, their promptness in responding to messages, volume of messages, convenience of the system, quality of the messages, and the amount of patient education offered. Both patients and physicians were asked whether patients should be able to e-mail their physicians and whether e-mail should be used for prescription refills and scheduling appointments. Participants in both the e-mail and control groups completed their respective patient or physician questionnaires.
Analysis
Patient and physician responses to questionnaires were summarized by frequency tables for categorical responses and descriptive statistics for continuous responses. Changes in the level of patient satisfaction across time were assessed within each group using the Friedman test for ordinal responses and repeated measures analysis of variance for continuous responses. Differences between the study and control groups with respect to patient satisfaction were assessed using analysis of variance controlling for physician effects. Given the few physicians in the study, changes in the level of physician satisfaction across time were not statistically significant. However, these data provided some general observations on physician response to e-mail communication with patients. Statistical analyses for other outcome measures were descriptive in nature. These data included the number of messages received, time physicians spent on answering messages, types (categories) of messages received, and response time (time lapse between when a message was received and when the physician replied). The response time and categories of messages were generated for both e-mail and phone messages. All analyses were conducted using SAS statistical software version 8.0 (SAS Institute, Cary, NC).
Results
Of 172 registered participants, 100 patients (58%) completed all questionnaires and were included in the data analyses (67 in the e-mail group, and 33 in the control group). All 8 physicians completed their time logs and questionnaires.
Patient Profile
The patient characteristics for both e-mail and control groups were similar (Table 2). The e-mail group was slightly younger, with 42% under age 50 vs 21% in the control group. There was equal distribution for the age-group older than 65 and for sex. On average, patients had been in the practice for more than 8 years. Three quarters of the patients had completed at least a college education. Most found it easy to use e-mail, and nearly 50% spent 1 to 10 hours per week on the computer. They used the Internet for health information (58% e-mail group, 70% control group), entertainment (32% e-mail, 49% control), news (32% e-mail, 70% control), business/finance (44% e-mail, 58% control), and shopping (46% e-mail, 52% control).
Selected Characteristics of Participating Patients at Baseline
Satisfaction
Patients
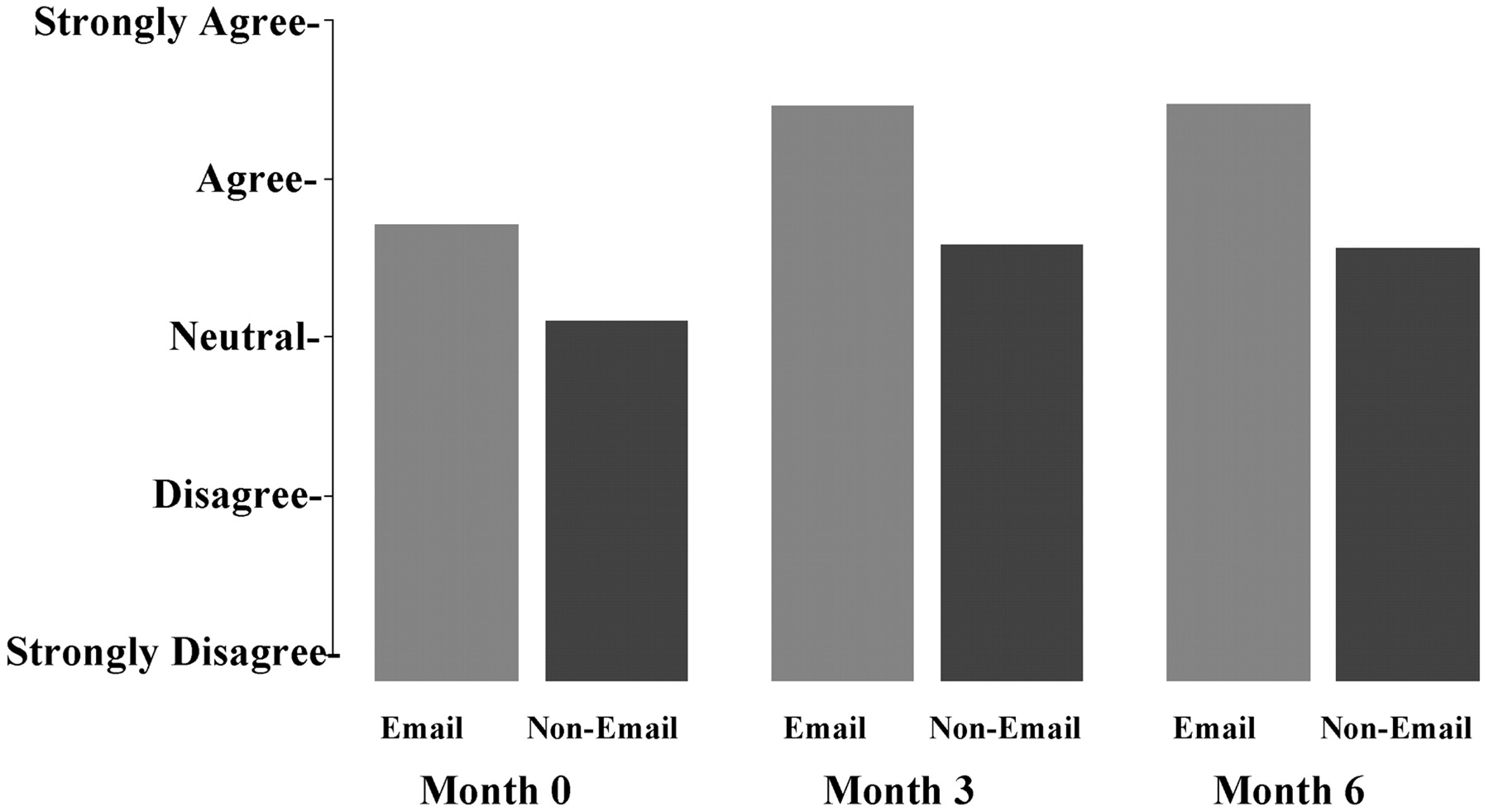
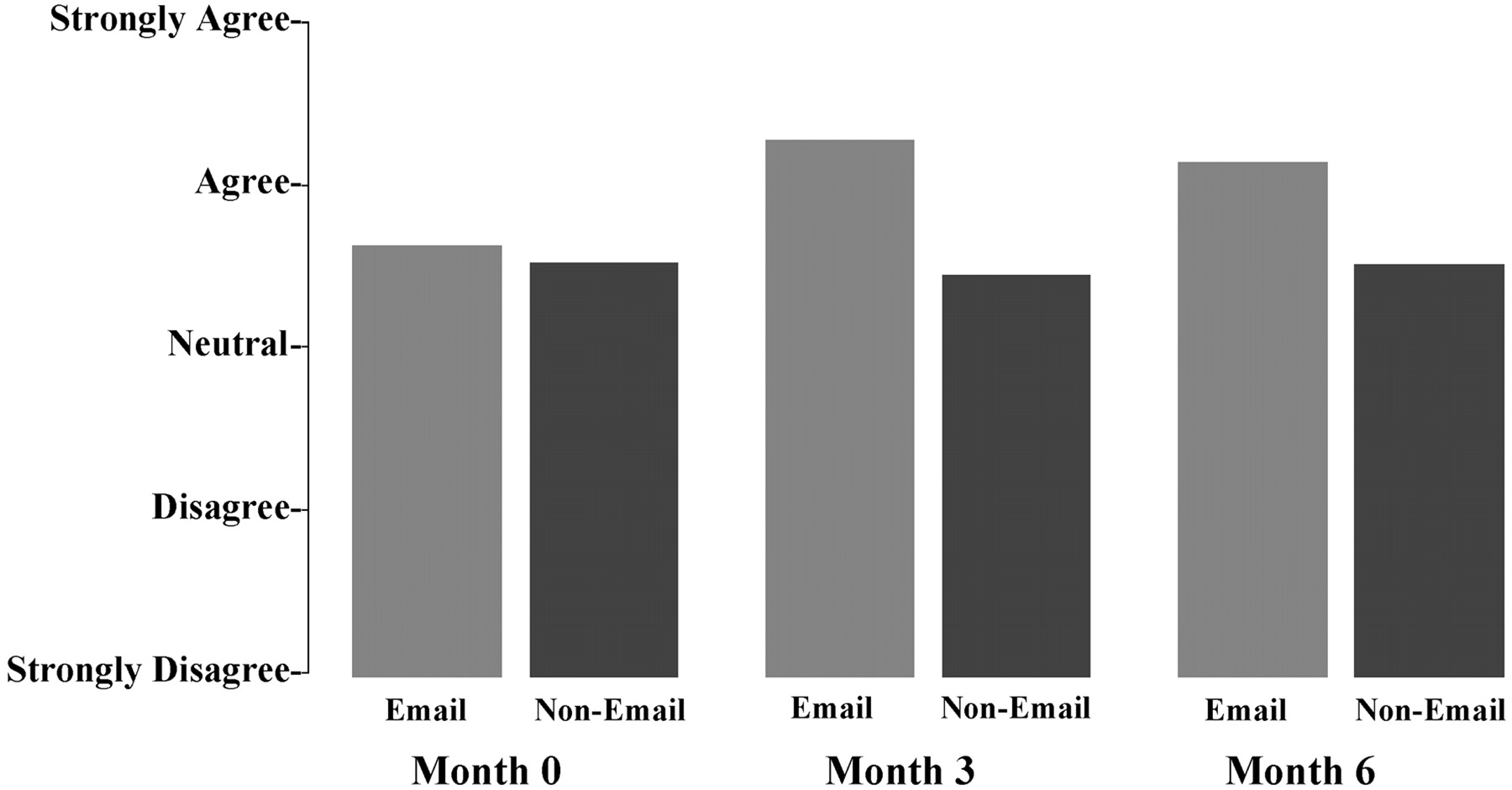
Patients in this study were generally very satisfied with the communication with their doctors at the time of entry into the study, rating most items in the questionnaire 4 or higher on a 5-point scale. However, 2 items showed a statistically significant difference between groups during the study. The level of satisfaction significantly increased in the e-mail group, compared with the control group in the areas of convenience of communicating with their physician (F = 8.29; P < .0001), as shown in Figure 1, and the amount of time spent contacting their physician (F = 7.84; P < .0001), Figure 2.
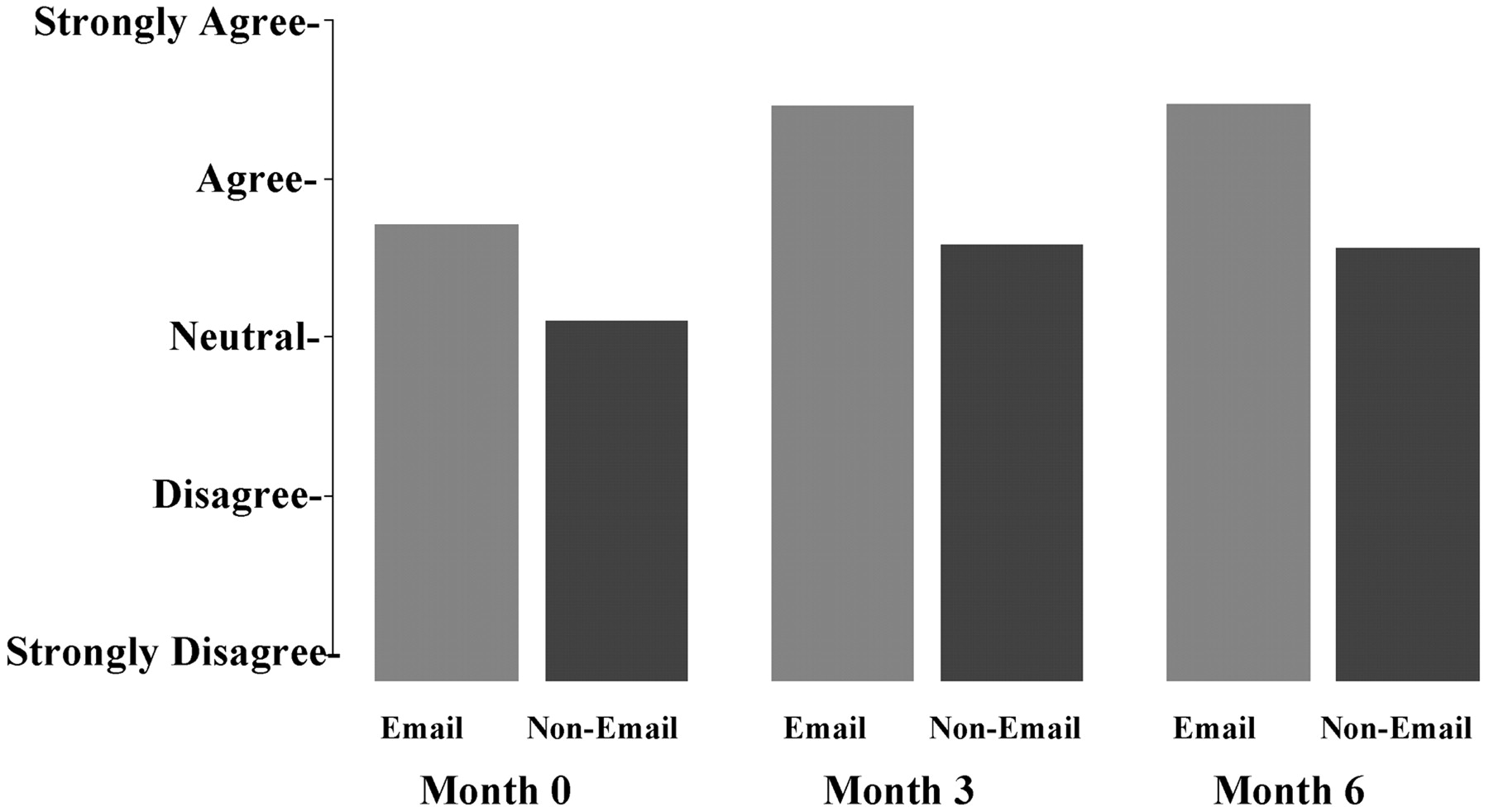
Patient satisfaction with the convenience of contacting doctor (P < .0001).
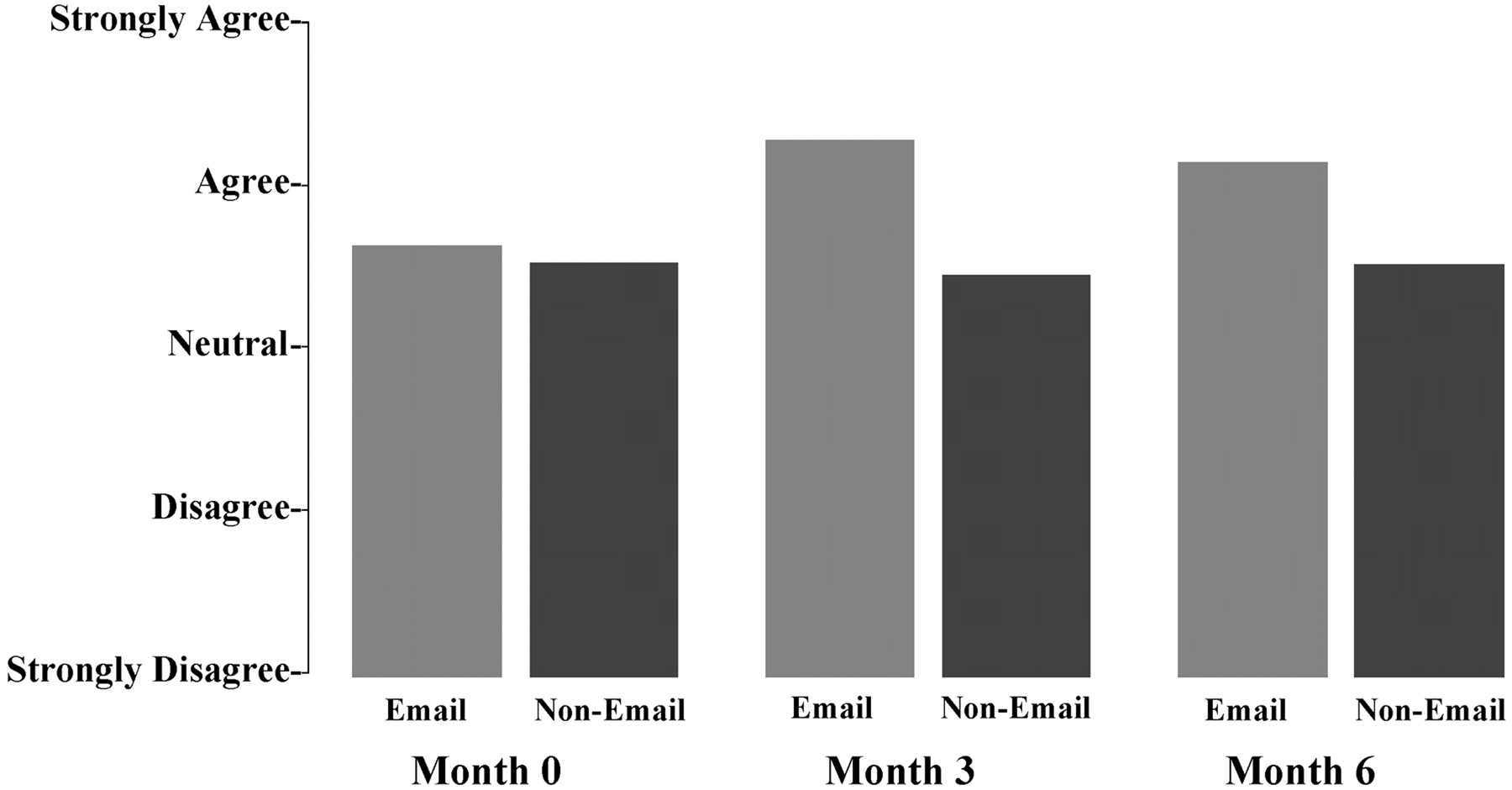
Patient satisfaction with the amount of time spent to contact doctor (P < .0001).
Physicians
Physicians in both the e-mail and the control groups were generally dissatisfied with the practice’s message system, rating it less than 3 on a 5-point scale. Given the few physicians in the study, changes in the level of physician satisfaction across time were not statistically significant; there were, however, some notable trends that seemed to correlate with the patients’ responses. Over the 6-month study period, physicians in the e-mail group seemed to have increased their satisfaction ratings in the message system in the areas of convenience, amount of time spent on messages, and volume of messages. They consistently rated their satisfaction higher than the non–e-mail physician group. These possible trends could be better studied using a larger physician sample. There were no significant changes in the number of messages during the study between the 2 groups either by self-reporting (F = 0.65; P = .42) (Table 3) or by the data gathered by the clinic secretaries (F = 2.71; P = .10). This suggests that perhaps the increased satisfaction may be the result of improved convenience or quality of communicating with patients.
Physician Self-Reported Log on Non–E-Mail and E-mail Messages from Patients
Messages
During the 3 selected weeks when all phone messages were collected for the study, 732 messages with complete information were available for data analyses (329 from the e-mail group and 406 from the control group). Over the study period, 299 emails were received from patients in the e-mail group. For all messages, we analyzed the categories, response time, and time required to address messages.
Categories
Of the phone messages, 270 (37%) were in the categories of administrative (referral, forms completion), 199 (27%) were on questions related to medical condition/consult, and 145 (20%) were on issues related to medications (refill, side effects, instruction on taking medication). A smaller number of messages were related to test results and/or were informational (update of conditions, sharing of information) (Table 4). E-mail messages included 95 (32%) informational, 93 (31%) on medical conditions/consult, 48 (16%) on medication, 43 (14%) administrative, and 20 (6.7%) on test results.
Categories and Response Time of Messages
Response Time
Of all the completed messages, 180 e-mail messages and 340 phone messages had sufficient data to calculate the time it took for the messages to be addressed by the physicians. Most phone messages (284 [83.5%]) were answered in the same day. The response time was longer with e-mail; 68 (38%) were answered in the same day, 53 (29%) in 1 day, and 28 (15.5%) in 2 days (Table 4). This may be the result of several factors. It is the practice’s policy to address phone messages from patients the same day. Phone messages in general are more acute in nature, requiring more urgent attention. There is no policy on e-mail response time because it is not the usual mode of communication for the practice. Patients in the study were advised to use e-mail for only nonurgent messages and that a reply might take 2 to 3 working days. Because there was a separate account for patient e-mail, one physician experienced some difficulties remembering to check that account for messages. In addition, it was not possible to access the account off-campus.
Time Required to Address Messages
During the same 3 selected weeks, the physicians also tracked the number of messages received and reported the time spent addressing messages (Table 3). There was great variation in the volume of messages reported by physicians: 15 to 103 per week in the e-mail group and 21 to 72 per week in the control group. Likewise, physicians differed in the time they took to address messages, from an average of 12 to 62 minutes per day and 2 to 5.5 minutes per message. This variation occurred in both the e-mail and control groups. All but 2 physicians had fewer messages in the third week of the study. Over the study period, 299 emails were received from patients in the e-mail group. Similar to the non–e-mail messages, the volume of messages and the time spent addressing these messages differed from one physician to another. Based on self-reported data, most physicians took less time to address e-mail messages (1 to 3 minutes per message).
Health Information Web Site
Once informed of the http://www.familydoctor.org web site, 97% of the patients visited the site at least once. In the beginning of the study, most of the patients found the web site very useful, but nearly 50% rated it only somewhat useful by the end of the study.
Preferences in E-Mail Communication
At the conclusion of the study, all patients and physicians were asked, “Should patients be able to e-mail their doctors?” All patients in the e-mail group and 97% in the non–e-mail group responded yes to this question. The physicians were less uniform in their answers. All 4 physicians in the e-mail group, but only 2 of the 4 in the non–e-mail group, answered affirmatively. Most patients in the study would like to e-mail physicians; 90% in the e-mail group and 86% in the non–e-mail group would use it for prescription refills, and 39% in the e-mail group and 19% in the non–e-mail group would like to use it for scheduling appointments.
Comments from the Patients
Of the written comments received on the questionnaires, 40% (33 of 83) were comments praising e-mail as a convenient and efficient method of communication. The patients enjoyed being able to give a quick update on their conditions to their physicians or ask questions regarding referrals. Eleven patients expressed frustration when calling the office, citing the long hold time and phone “tag.” One patient in the non–e-mail group wrote a lengthy letter urging the institution to provide e-mail access for all patients. Only 2 patients expressed concern over privacy issues.
Discussion
In our study, e-mail communication was judged to be a convenient form of communication between the patient and the physician. Satisfaction for patients was improved, and satisfaction for physicians seemed to be improved, but no improvement could be confirmed through statistical analysis of the data. The volume of messages and time spent answering messages for the e-mail group of physicians was not increased. However, the physicians commented that if e-mail were to be offered to a larger group of patients, additional support staff would be required to effectively manage the e-mail messages from patients. A triage system similar to that used by Stanford Medical Group in Palo Alto, California, where a staff member would route e-mail to the appropriate person could help reduce the time burden on the physicians.16
Table 5 lists some important guidelines for e-mail communication between physician and patient. E-mail communication is ideal for short questions, brief updates, follow-ups, or clarification of instructions. It is not intended to replace the office visit. Issues that are complex, contain uncertainty, or would require negotiation should be addressed face-to-face in the office. To avoid legal and liability complications, an existent patient-physician relationship should be in place before offering advice via e-mail. With the Health Insurance Portability and Accountability Act (HIPAA) regulation, extra diligence is required to insure privacy. Before using e-mail to exchange information, physicians must obtain written informed consent from patients. Patients need to understand that e-mail communication is nonsecure and confidentiality cannot be guaranteed. E-mail should not be used for urgent or sensitive matters. Sands and others12,23 have provided useful guidelines for the appropriate use of e-mail. Since the conclusion of the study in July 2002, the Penn State Hershey Medical Center has issued a set of updated guidelines for e-mail communication with patients based on current national guidelines. The Penn State Hershey Medical Center Patient’s Guide to e-mail is accessible at http://www.hmc.psu.edu/visitors/HIPAAemail.pdf.
Guidelines for E-mail Communication between Physicians and Patients23
One limitation of this study is that neither physicians (who were placed in groups by the principal investigator to maintain a balance in physician characteristics) nor patients (who were assigned to their respective physician’s group to maintain the doctor-patient relationship) were randomized, thereby creating uncertainty regarding the effects of the intervention. The small sample size of 8 physicians limited the potential for yielding statistically significant data. The patients were from a university hospital-affiliated family practice office and were well-educated and Internet-savvy; therefore, the results may not be generalizable to other office settings and patient populations. The control group reported a higher rate of Internet use than the e-mail group (Table 2). The significance of this is unclear. The utility of the health information web site was modest, with declining interest and rating of the site over time. It is not known whether this is a reflection of the quality of the web site or is a typical pattern of use for web resources. More data are needed in this area.
Most e-mail messages from this study were for updates on conditions (32%), short medical consultations (31%), and questions related to medications (16%). These types of information allow the physicians to manage the patients’ medical problems beyond the office visit. By improving access to care and communication between patients and physicians, e-mail has the potential to help prevent medical errors. For example, with the ease of e-mail communication, patients may be more likely to report potential medication side effects before the next office visit, adding to medication safety. Coupled with a well-developed patient education web site, e-mail has the potential to improve patient education and improve management of diseases. In this study, the amount of time used to answer messages from patients was not increased, suggesting that potentially improved access by e-mail does not cause undue burden on the physician or practice.
E-mail is a widely used mode of communication. As we move toward using an electronic medical records system, e-mail would be a useful component. The medical field needs to define appropriate uses for this communication, develop standards and guidelines, ensure privacy and security, and assess and address issues related to compensation for service and legal and ethical implications. After taking the appropriate measures to address these important concerns, e-mail holds enormous potential as a practice tool to enhance health care delivery, as well as the health outcomes of patients.
Acknowledgments
We thank Connie Weirich and Stacey Haak, administrative assistants at Penn State College of Medicine, for their excellence in data collection and manuscript preparation.
Notes
This research was supported in part by a General Clinical Research Center grant from National Institutes of Health (M01-RR10732) awarded to the Pennsylvania State University College of Medicine and the Penn State Milton S. Hershey Medical Center.
This work has been presented at the 36th Society of Teachers of Family Medicine Annual Spring Conference; 2004 Sep 20–24; Atlanta, Georgia, and the 31st Annual North American Primary Care Research Group; 2003 Oct 25–28; Banff, Alberta, Canada.
- Received for publication December 23, 2004.
- Revision received December 23, 2004.
References




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Patients use and experiences with e-consultation and other digital health services with their general practitioner in Norway: results from an online survey
- Prevalence and Factors Associated with Family Physicians Providing E-Visits
- The benefits of encouraging patients to email their doctor: a review of individual practice
- What keeps family physicians busy in Portugal? A multicentre observational study of work other than direct patient contacts
- Triage and remote consultations: moving beyond the rhetoric of access and choice